
Abstract
Background
This study was designed to assess oral ulcerative mucositis, C-reactive protein, blood pressure, heart rate and thyroid function in breast cancer patients in relation to the occurrence of posttraumatic stress disorder (PTSD).
Methods
A total of 120 female breast cancer patients and women 100 healthy subjects were enrolled in this study. PTSD status was assessed by questionnaire. Before and after treatment (modified radical mastectomy and chemotherapy), serum samples were collected and measured for levels of triiodothyronine (T3), thyroxine (T4), thyroid stimulating hormone (TSH) and high-sensitivity C-reactive protein (hs-CRP) by ELISA. Oral ulcerative mucositis was evaluated by the number and duration of oral ulcers and the degree of pain.
Results
Breast cancer patients experienced long-term PTSD and had elevated serum T3 and T4 levels. Patients experienced more severe pain and longer duration of oral ulcers compared with the healthy group. Oral ulcers were significantly associated with PTSD score in terms of the number of ulcers (p=0.0025), the degree of pain (p<0.0001) and the duration of ulcers (p<0.0001).
Conclusion
These findings support that thyroid function is altered in breast cancer patients with PTSD. Elevation of T3 and T4 and oral ulcerative mucositis might be indicative of the emotional status of breast cancer patients.
Introduction
Posttraumatic stress disorder (PTSD) is a severe anxiety disorder that develops as a result of exposure to any incident (such as car crash accidents, earthquakes, cancer, etc.) resulting in psychological trauma (1). As an effect of neural trauma, PTSD is less common and more permanent than acute stress response, which happens more frequently (2). The symptoms of PTSD include difficulty in falling or staying asleep, irritation, hypervigilance (3), rise in heart rate, blood pressure and plasma levels of glucose, and alteration of some biomarkers such as cortisol, serotonin, C-reactive protein (CRP) and interleukin-6 (IL-6) (4-6). Formal diagnostic criteria require the symptoms to last more than 1 month and cause significant impairment in social, occupational, or other important areas of function (7).
Suffering from cancer can be a source of PTSD for patients. The physical and mental shock of having a life-threatening disease, receiving treatment for cancer, and living with repeated threats to one's body and life are traumatic experiences for many cancer patients (8, 9). For the person with a diagnosis of cancer, the specific trauma that triggers PTSD is unclear. The anxiety may be attributed to the diagnosis of a life-threatening illness, aspects of the treatment process, and recurrence of the disease. There are gender differences in the experience to different types of trauma, or differences in the neurobiological response to trauma.
PTSD exhibits physiological or biochemical changes in the neuroendocrine axis that differ from other psychiatric disorders (13, 14). The majority of people with PTSD show a low level of cortisol and high levels of catecholamines in urine, with a norepinephrine/cortisol ratio higher than that in comparable non-diagnosed people (15) through the activation of the hypothalamic-pituitary-adrenal (HPA) axis, which has been a major focus of scrutiny in patients with PTSD. Elevated T3 has also been found in patients diagnosed with PTSD (16, 17). Since the blood levels of thyroid hormones are controlled by the hypothalamic-pituitarythyroid (HPT) axis, a possible role for the HPT axis in stress-related syndromes has been suspected because it is known that trauma can trigger thyroid abnormalities (16). Another chief characteristic of patients with PTSD is continuous hyperactivity of the sympathetic branch of the autonomic nervous system such as increased heart rate and blood pressure. In addition, increased urinary excretion of norepinephrine and epinephrine, and their metabolites, has been recognized in people with PTSD (18, 19). Furthermore, inflammation might link PTSD with an increased risk of cardiovascular events through the pathway of proinflammatory activity (20). A low-grade systemic proinflammatory state related to PTSD symptom levels suggests that PTSD may contribute to atherosclerotic disease and systemic inflammation (21-23).
Oral ulcerative stomatitis or mucositis is possibly associated with PTSD (24). Oral mucositis is a major nonhematological complication of cytotoxic chemotherapy and radiotherapy associated with significant morbidity: pain, odynodysphagia, dysgeusia, and subsequent dehydration and malnutrition, which reduce the quality of patients’ lives. Patients who are diagnosed with cancer may experience oral mucositis before, during and after treatment. In addition, oral mucositis represents a significant risk factor for systemic infections, particularly in neutropenic patients. It affects approximately one-third of patients who receive chemotherapy for the treatment of cancer (25, 26). In our follow-up data, oral mucositis was more often present in women than in men after they were administered chemotherapeutic drugs for 6, 12 and 24 months (27).
Mucositis can also be a normal occurrence in healthy subjects and may be caused by restlessness, nervousness, environmental factors, influenza, viral infection, anxiety or even a weakened immune system (27).
PTSD affects a person's physiological and psychological condition and may indirectly affect the patient's general health and quality of life, thereby lowering their interrelationship activity. If patients with PTSD can be diagnosed and treated at an early stage, the burden on the overall medical system will be alleviated. In the present study, we investigated the change in biological biomarkers and the status of oral ulcerative mucositis, and evaluated PTSD effects in women with breast cancer.
Materials and Methods
Study design
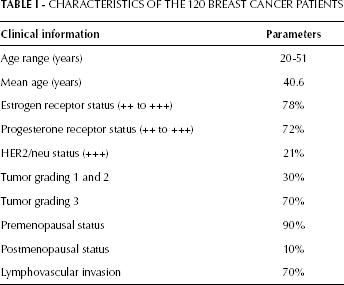
A total of 120 female breast cancer patients from the West China School of Medicine, West China Hospital, Sichuan University, Chengdu treated between 2010 and 2012 with a mean age of 40.6 years were included in the study (Fig. 1). Written informed consent was obtained from all patients prior to the study procedures and the study was approved by the institutional ethical board of Sichuan University. One hundred community women subjects were invited as controls (healthy group) and gave their signed consent for us to conduct similar measurements as in the patient group. All patients were diagnosed with invasive ductal carcinoma and treated with modified radical mastectomy (MRM). Adjuvant chemotherapy consisting of 4 cycles of FEC (5-fluorouracil 500 mg/m2, epirubicin 75 mg/m2 and cyclophosphamide 500 mg/m2) every 3 weeks was given. There were 20% triple positive patients (ER, PR and HER2) and 7% triple negative patients. Most of them were premenopausal and 70% were diagnosed with grade 3 tumors with lymphovascular invasion and did not show any recurrence, distant metastasis or other systemic diseases after chemotherapy up to 12 months (Tab. I). A PTSD questionnaire, clinical measurements including pulse, blood pressure and oral examination, and blood sampling for high-sensitivity CRP (hs-CRP) and thyroid function tests were conducted before MRM and 12 months after chemotherapy.

Flowchart of the study.
Characteristics Of The 120 Breast Cancer Patients
Measurement of serum biomarkers
Peripheral blood samples (6 mL) were collected by direct venipuncture from the arm vein of each subject into clot tubes (Vacutainer, BD, Franklin Lakes, NJ, USA). After blood clot removal and centrifugation, serum was frozen at −70°C until assayed. Sera were taken for the hs-CRP test (COBAS INTEGRA 400 plus, Roche, Germany) and thyroid function tests (Elecsys 2010, Roche, Germany) in the automation machines on the day before treatment and 12 months after chemotherapy.
Clinical measures
The questions regarding levels of anxiety, depression and PTSD were referenced from the Anxiety Disorders Resource Center (USA) and some modifications were made. In order to make it easier for the patients to answer the questions, we set the answers to “Yes” or “No”. Age, heart rate and blood pressure were also recorded during the interview.
Oral examination
All subjects were given 0.2% chlorhexidine mouthwash once a day. The monitoring of oral ulcers started on the days of the interviews (before the operation and 12 months after the end of chemotherapy) and lasted 30 days. The Oral Mucositis Assessment Scale (OMAS) was used to evaluate the size, number and duration of oral ulcers (28). The degree of pain was assessed by a numeric rating scale system (29) with a score from 0-10 (0, no pain at all; 10, intolerable pain).
Data analysis
Statistical analysis was performed using analysis of variance (1-way ANOVA) and Student's t-test of SPSS (v. 17.0) to measure emotional and biological parameters, which were compared between the groups. The correlation between the number of oral ulcers, degree of pain and duration of oral ulcers and PTSD were determined by Pearson's correlation coefficients. A p value less than 0.05 was considered statistically significant.
Results
The mean duration of oral ulcers was significantly longer in the patient group than the healthy group. Compared to healthy individuals with oral ulcers for an average of 4 days, patients had a longer mean duration of ulcers before treatment (9 days) (p=0.0001) and after chemotherapy (9 days) (p<0.0001). A significant difference was also observed for the number of oral mucosal lesions between patients and healthy subjects (1.9 vs 0.9, p<0.01). Mucositis-related pain was assessed with the numeric rating scale system before and after treatment, and the scores were 7.5±1.25 and 7.1±1.19, respectively, which were more severe than the score of 3.4±1.90 measured in the healthy group (p<0.01) (Tab. II). There were no differences between measurements before and after treatment concerning the duration of ulcers, number of ulcers and degree of pain (p=0.9697, p=0.9485 and p=0.4225, respectively). PTSD scores assessed by questionnaire were similar before and after treatment (73.0±0.976 vs 75.7±7.25, p=0.3548). More severe emotional difficulty was experienced in patients before treatment (p=0.001) and after treatment (p<0.001) than in the healthy group. The association between PTSD score and oral ulcers was assessed using the Pearson correlation test. PTSD score showed a positive correlation with oral ulcer number (r=0.356, p=0.0025), pain degree (r=0.645, p<0.0001) and oral ulcer duration (r=0.670, p=0.0001) (Tab. III).
Comparison Of Oral Ulcers And Ptsd Scores Between Breast Cancer Patients And Healthy Controls
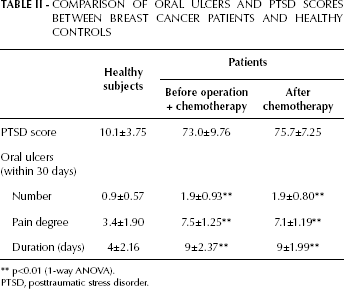
p<0.01 (1-way ANOVA).
PTSD, posttraumatic stress disorder.
Association Between Ptsd Score And Oral Ulcers
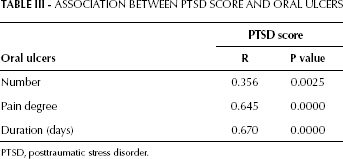
PTSD, posttraumatic stress disorder.
Multivariate ANOVA including all serum measurements of thyroid function showed a significant overall mean difference between the healthy group and the patient group (Tab. IV). Significant elevations of serum total T3 and T4 were found in the patient group compared with control subjects (p<0.01). The TSH level in patients before treatment and 12 months after chemotherapy was lower than in healthy subjects (p<0.05). No significant differences were found in the levels of T3, T4 or TSH in breast cancer patients before and after treatment. As shown in Table IV, the hs-CRP levels were also significantly higher in patients compared to healthy subjects (patients before treatment vs control, 2.117±0.931 vs 0.62±0.240; patients after treatment vs control, 2.09±0.754 vs 0.62±0.240). Other physiological parameters, such as blood pressure and pulse rate, were also significantly higher in patients than in the healthy group and no significant differences were observed between patients before and after treatment (Tab. V).
Serum Hs-Crp, T3, T4 And Tsh In Breast Cancer Patients And Healthy Controls
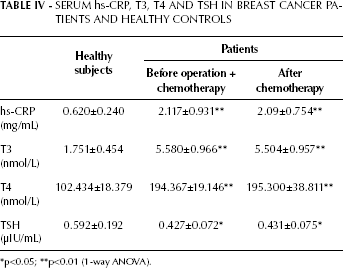
p<0.05;
p<0.01 (1-way ANOVA).
Blood Pressure And Pulse In Breast Cancer Patients And Healthy Controls
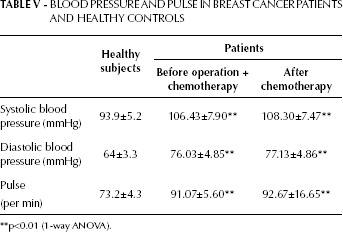
p<0.01 (1-way ANOVA).
Discussion
Previous studies have demonstrated that women suffer from anxious emotion when diagnosed with breast cancer, which was also observed in the present study (30, 31). Compared with the healthy subjects, patients exhibited a higher degree of anxiety both before and after treatment. The serum level of hs-CRP was dramatically increased in patients before surgery and chemotherapy and this high level continued after chemotherapy. As shown by Howren et al (32), the prominent inflammatory markers such as CRP are positively associated with depression and there is a dose-response relationship between depression and these inflammatory markers (32, 33). Physiological stress was also evident from the elevated blood pressure and pulse in patients compared to age-matched healthy subjects. These data indicate that breast cancer is an experience of repeated trauma of undetermined duration. Patients may experience stress symptoms anytime from diagnosis through completion of treatment and cancer recurrence.
Traditionally, it is believed that radiation and chemotherapy agents induce mucositis due to the depletion of basal cell layer stem cells of the oral mucosa. Because of the loss of basal cell stem cells, the uppermost layers of the mucosal epithelium slough off, resulting in discontinuity of the mucosa and the formation of ulcers (34). In this study, we noticed that breast cancer patients already suffered from oral mucositis before the introduction of chemotherapy. Before MRM, patients had suffered more severe pain from oral ulcers than healthy subjects. At 12 months after 4 cycles of adjuvant chemotherapy, the severity of oral ulcers remained the same in terms of the number of ulcers, degree of pain, and duration or ulcers. In addition to the effect of cytotoxic agents used in chemotherapy, we hypothesized that oral ulcer development in breast cancer patients might be attributable to PTSD. It was found that PTSD score showed a significantly positive correlation with oral ulcer number, pain degree and oral ulcer duration. These data suggested that psychological conditions such as PTSD might involve physiological changes such as oral mucositis. Although the molecular and cellular pathways that lead to oral mucositis are unclear, it is well accepted that the production of proinflammatory cytokines, caspases, matrix metalloproteinases, leukotrienes, and ceramides are related to the pathology of oral mucositis (35, 36), among which inflammation is an important component (34). Recent studies indicated an excess of inflammatory actions of the immune system in individuals with chronic PTSD (37). High levels of inflammatory cytokines including hs-CRP, tumor necrosis factor alpha (TNF-α), IL-6, IL-1α, IL-1β, IL-8, GM-CSF, and interferon alpha (INF-α) have been linked to PTSD vulnerability in traumatized individuals (22, 38, 39). These proinflammatory cytokines in patients with PTSD exert cellular damage and induce apoptosis; for example, TNF-α activates caspase pathways leading to tissue damage and also activates the transcription pathways mediated by NF-κB. In a feedback loop, the process results in further production of TNF-α, IL-1β, and IL-6 (36). Finally, direct and indirect damage to epithelial stem cells results in loss of renewal capacity. As a result, the mucosal epithelium gets thinner and patients experience the symptoms of mucositis.
Biological studies of traumatic stress in humans have focused mainly on the responses of the HPA axis, but little attention has been paid to the HPT axis. In this study we also investigated the relationship between thyroid function and PTSD. The normal ranges for serum total T3 and T4 are 1.3 to 3.1 nmol/L and 66.0 to 181.0 nmol/L, respectively. Before treatment and 12 months after treatment, we conducted a thyroid function test on the breast cancer patients. Elevated T3 and T4, but no elevated TSH, was found in patients compared to age-matched healthy subjects with normal values for the tests. Our data were consistent with the study performed by Wong et al (17), who found a significantly positive relationship between total and free T3 and PTSD symptoms. Our study supports the observation that the thyroid system is altered in breast cancer patients suffering from PTSD. No differences in the levels of T3, T4 and TSH were observed between patients before treatment and after chemotherapy. The observed changes of thyroid function along with PTSD symptoms appear to be chronic.
The effects of PTSD are long-lasting and serious, which may affect the patient's psychological and physiological health. Oral ulcerative mucositis and several blood biomarkers might be useful in the long-term monitoring of PTSD so that early symptoms may be identified and treated.