
Abstract
Purposes
This study aimed at investigating the association between interleukin-6 (IL-6), interleukin-12 (IL-12), C-reactive protein (CRP), vascular endothelial growth factor (VEGF) and β-defensin-1 polymorphisms and the susceptibility to periodontitis in the Chinese population.
Methods
DNA was extracted from the blood samples of 532 healthy individuals and 122 chronic periodontitis (CP) patients enrolled in the study. The genes encoding IL-6, IL-12, CRP, VEGF and β-defensin-1 were amplified using PCR and digested with restriction enzymes. The protein expression of the abovementioned genes was determined by ELISA. Differences in the allele/genotype frequencies were assessed with the chi-square test.
Results
The frequencies of the C/C genotypes of IL-6, IL-12, and VEGF were higher in CP patients than healthy controls (66.3% vs 25.9%; 27.8% vs 19.9%; and 64.8% vs 52.1%, respectively). In the patients' group we also recorded frequencies of the A/A genotypes of CRP and VEGF higher than in healthy controls (63.1% vs 58.1% and 64.8% vs 35.2%, respectively). Protein production evaluated by ELISA demonstrated significant differences between CP patients and healthy controls for IL-6, IL-12, CRP, VEGF and β-defensin-1.
Conclusions
The genotypes of IL-6, IL-12, VEGF and β-defensin-1 and their protein productions were associated with CP in a Chinese population. Genotypes and serum levels of CRP were associated with CP, but alleles frequency showed no difference between CP patients and healthy controls.
Introduction
Periodontitis is a multifactorial infection leading to eventual teeth loss (1, 2). Destruction of the underlying ligament and the alveolar bone is influenced by the host immune response to the microbial challenge (3). There is no positive correlation between the quantity of bacterial plaque and the severity of periodontitis (4). However the specific bacterial component, accounting for only 9%-16% of the variance in periodontitis expression (5), suggests that susceptibility to periodontitis may be significantly modified by the host responses to bacterial plaque. In recent years, large scientific evidence showed that several genes influence an individual's predisposition for the initiation and progression of the periodontal disease (6-8).
It is estimated that more than 20 genes and hundreds of polymorphisms of genes are related to chronic periodontitis (CP) (9), and these gene polymorphisms are usually associated with ethnic populations (5). Cytokines, such as interleukin-1 (IL-1), interleukin-6 (IL-6) and interleukin-12 (IL-12) as well as other genes including HLA, immune-receptors (FcR), poteases (MMP), and structural molecules (Cathepsin C and Vitamin D-R) seem to play an important role in the focal immunopathology of periodontal disease (10-12). Polymorphisms within candidate genes may be causally related to changes in protein expression, structure, and function. Thus, the genetic control of the functions of these genes may affect the severity of periodontitis (13).
IL-6 plays an important role in stimulating hematopoiesis and accelerating bone resorption (14). Higher levels of IL-6 were found in sites with gingivitis, compared with healthy sites (15). The C allele at position −174 was shown to alter the IL-6 gene transcription in response to stimuli such as lipopolysaccharides and IL-1 (16). The C allele creates an NlaIII restriction site and has been assigned Genbank accession number AF005845 (17). IL-12 is vital to the orchestration of cell-mediated immune responses in both the innate and adaptive immune responses (18-20). Polymorphisms of these 2 cytokines have also been studied in various immune-related disorders and infections (21). A nucleotide change from +1188A to +1188C in the 3′-untranslated region of the IL-12B locus is associated with diminished cytokine production in various populations (20). The A/C base pair substitution at position 1188 has been associated with interleukin-12B mRNA expression levels, however these reports are somewhat controversial (22).
C-reactive protein (CRP) is an acute phase protein and its levels increase rapidly during infection and inflammation (23). Thus, CRP is recognized as a sensitive and dynamic systemic marker of inflammation. High sensitive CRP (hs-CRP) is reported to be a strong predictor of cardiovascular risk, in spite of conventional cardiovascular risk factors (24). The A/G polymorphism at position 717 of the human CRP gene was found to be associated with coronary heart disease (25). The infection-induced elevation of systemic CRP might account for the relationship between inflammatory and cardiovascular diseases.
Periodontal disease is a chronic inflammatory disease of the highly vascularized supporting tissues of the teeth. Vascular endothelial growth factor (VEGF) is a 45-kd homodimeric glycoprotein with potent vascular permeability and angiogenic effects (26). Several polymorphisms have been described in the VEGF gene. Three single-nucleotide polymorphisms (SNP) (G+405C in the 5′-untranslated region, C-460T in the promoter region, and C+936T in the 3′-untranslated region) are common and related to VEGF protein production (27).
-defensins are cationic antimicrobial peptides expressed in epithelia, exhibiting antibacterial, antifungal, and antiviral properties. Defensins, peptidic components of the innate immune response, are proposed to have a protective role in the oral cavity in periodontal science. Previous studies have shown that human -defensin-1 is constitutively expressed in oral epithelial cells, but that expression varies between individuals. In the oral cavity, human -defensin-1 expression can be found in the gingival, parotid and submandibular glands, as well as in buccal mucosa, palatine tonsil and on the tongue (28).
Since CP is characterized by pathologically elevated host and microbial-derived proteolytic burden, it was hypothesized that human gingival tissue affected by periodontitis expressed elevated levels of inflammation-associated proteins (29). Several inflammation-related gene polymorphisms and their respective serum levels were studied in CP patients and healthy controls for our case-control study.
Materials and Methods
Subject selection
A total of 654 unrelated Chinese subjects, including 532 healthy individuals and 122 CP patients were recruited for this case-control study (Tab. I). Informed consent was obtained from all participants, and the study protocol was approved by the Sichuan University Ethics Committee, China. Clinical examinations were performed in West China Hospital of Stomatology, Sichuan University. All participants were determined to be free of systemic or chronic diseases, past and current smoking habit, swelling of the lymph nodes, temporal mandibular joint disease and soft tissue abnormalities. Only patients with diagnosed CP and healthy subjects who were completely free of periodontitis, based on clinical and radiographic examination, were enrolled.
BASELINE DEMOGRAPHICS AND PERIODONTAL CLINICAL DATA FOR INDIVIDUALS IN THE HEALTHY (H) AND CHRONIC PERIODONTITIS (CP) GROUPS AND THEIR STATISTICAL COMPARISON
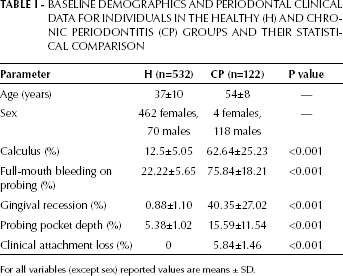
For all variables (except sex) reported values are means ± SD.
Diagnosis of periodontal disease was made on the basis of the 1999 International Classification of the Periodontal Disease and conditions (30). Physical examination, medical and dental history, supragingival calculus, gingival recession, bleeding of probing, probing depth, clinical attachment loss (CAL), tooth mobility and plaque were considered as clinical parameters. Subjects were classified into 2 groups. (i) The healthy group: consisted of 462 females and 70 males between the ages of 18 and 60 (mean age: 37±10). These subjects had no signs of periodontal disease in the absence of gingival recession, CAL and sites with probing depth >3 mm (n=532). (ii) The CP group: included 4 females and 188 males between the ages of 38 and 62 (mean age: 54±8). These subjects presented probing depth >5 mm, CAL >4 mm, some degree of gingival recession and teeth mobility (n=122).
Sample preparation
Ten milliliters of blood from each subject were collected in lithium heparin tubes (Vacueete, Austria). Blood was centrifuged for 10 minutes at 1,500 rotations per minute (rpm), and plasma was removed for ELISA analysis. The remaining cells were transferred to a 50 mL centrifuge tube along with red blood cell lysis buffer, up to a final volume of 45 mL. The mixture was inverted several times followed by centrifugation for 10 minutes at 1,500 rpm. Its supernatant was discarded, and the remaining cells were washed with 0.9% PBS for subsequent DNA extraction.
DNA extraction
Genomic DNA was extracted from all samples using a commercially available Genomic DNA Mini Kit (Qiagen, USA) following the manufacturer's instructions. The extracted DNA was labeled and stored at −80°C until use.
Polymerase chain reaction (PCR) and restriction fragment polymorphism (RFLP) analysis
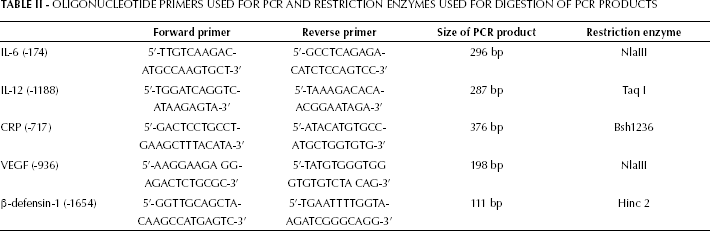
Genomic DNA extracted from blood was subjected to PCR amplification of polymorphic regions. The products were digested by restriction enzymes. The primer pairs and restriction enzymes for IL-6, IL-12, CRP, VEGF and -defensin-1 SNPs (Tab. II) were previously described in literature (20, 28, 31-32). Amplification reactions were performed in a total volume of 50 μL, using 500 ng of genomic DNA as template. The PCR reaction contained 10 mM Tris-HCl (pH 8.3), 50 μM KCl, 1 μM of each primer, 200 μM of each dATP, dCTP, dGTP and dTTP, 4 mM MgCl2, and 2.5 U Taq DNA polymerase (Amersham Pharmacia Biotech, Uppsala, Sweden). The reaction was incubated at 95°C for 5 minutes, followed by 35 cycles at 95°C for 1 minute, 60°C for 1 minute, 72°C for 1 minute, and a final extension at 72°C for 5 minutes. Ten microliters of PCR product was digested with NlaIII for the IL-6 SNP, with Taq I for the IL-12 SNP, with Bsh1236 for the CRP SNP, with NlaIII for the VEGF SNP and with Hinc 2 for the -defensin-1 SNP (Tab. II). After electrophoresis in 3% NuSieve® agarose gel (Invitrogen, Spain), digested fragments were visualized under ultraviolet light to determine the genotypes.
OLIGONUCLEOTIDE PRIMERS USED FOR PCR AND RESTRICTION ENZYMES USED FOR DIGESTION OF PCR PRODUCTS
Electrophoresis and visualization of digestion products
Five microliters of amplified product and 1 mL of Ready-Load 1 kb DNA Ladder (Invitrogen, Spain) were loaded into 3% agarose gel containing 0.5 mg/mL of ethidium bromide. The gel underwent electrophoresis at 100 V, 100 mA for 30 minutes and was visualized using a Dolphin-DOC ultraviolet illuminator (Wealtec, South Africa).
ELISA assay
The serum plasma samples were used to perform ELISA analysis using the IL-16, IL-12, CRP, VEGF and -defensin-1 ELISA Kits (Phoenix Pharmaceuticals, Inc., USA). The procedures, performed following the manufacturer's instructions, are here reported in brief: 50 or 100 μL of the standard group solutions and serum/plasma of each subject were loaded into a 96-well plate. The plate was incubated for 2 to 3 hours at 350 rpm and washed 3 times with washing buffer. Afterwards, the wells were dried and 200 mL of substrate tetramethylbenzidine was added into each well for 20 minutes in the dark at room temperature. The plates were read at a wavelength of 450 nm using the Universal Micro plate Reader (Sunrise, TECAN, Austria). The levels of IL-16, IL-12, CRP, VEGF and -defensin-1 in the samples were obtained by comparison with the standard curves generated from standards supplied by the manufacturer.
Statistical analysis
Differences in genotype, allele frequencies and carriage rates between the CP and control groups were examined by the chi-square test ( 2 ). For risk analysis of alleles and genotypes, the odds ratio (OR) with a 95% confidence interval (CI) was calculated. The soluble protein levels of IL-6, IL-12, CRP, VEGF and -defensin-1 were evaluated using the independent t-test. Results were considered statistically significant when p value was <0.05. Statistical analysis was performed using the statistical software SPSS, version 15.0 for Windows (SPSS Inc., U.S.A.).
Results
Genotypes and allele frequencies of IL-6, IL-12, CRP, VEGF and β-defensin-1 in the CP and control groups
Distribution of the IL-6 polymorphism at position −174
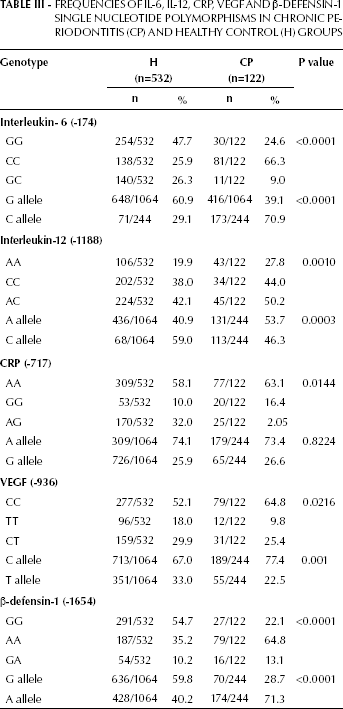
For the −174 site of IL-6, homozygous C alleles presented 4 DNA bands with the sizes of 13, 118, 109 and 59 bp; homozygous G alleles presented 5 DNA bands with the sizes of 13, 118, 108, 227 and 5 bp. Heterozygote individuals for IL-6 at position -174 displayed a combination of both C and G alleles (13, 227, 59 bp). There was a significant difference both in the genotype distribution ( 2 =73.6, p<0.0001) and allele frequency (p<0.0001) between healthy controls and CP patients for this polymorphism of IL-6 (Tab. III). The frequency of the homozygous G alleles for IL-6 was higher in the CP group than the homozygous C alleles in the control group (60.9% vs 29.1%). The result of the chi-square test between the CP and the control groups was 2 =81.1, p<0.001, while the OR was 3.80 (95% CI=2.81-5.14).
Distribution of the IL-12 polymorphism at position -1188
The distribution of the IL-12 polymorphism at position -1188 among the CP and control groups is shown in Table III. For IL-12, homozygous A alleles at this site presented 1 DNA band with the size of 287 bp. Homozygous C alleles presented DNA bands of 183 and 104 bp. Heterozygotes for IL-12 at position -1188 displayed a combination of both C and A alleles (287, 183, 104 bp). The distribution of the IL-12 gene polymorphism at position -1188 was statistically different among the 3 genotypes ( 2 =13.7, p=0.0001) (Tab. III). Significant differences in the allele frequency at the -1188 site between the CP and control groups were confirmed by the OR and 95% CI in all the subjects (OR=0.599, 95% CI=0.453-0.792). The frequency of the A allele in CP patients was much higher than in healthy controls (53.7% vs 40.9%).
FREQUENCIES OF IL-6, IL-12, CRP, VEGF ANDβ-DEFENSIN-1 SINGLE NUCLEOTIDE POLYMORPHISMS IN CHRONIC PERIODONTITIS (CP) AND HEALTHY CONTROL (H) GROUPS
Distribution of the CRP polymorphism at position -717
For the -717 site of the CRP gene, homozygous A alleles presented 1 DNA band of 376 bp whereas homozygous G alleles presented 2 DNA bands with the sizes of 376 and 319 bp. Heterozygotes for CRP at position -717 displayed a combination of both G and A alleles (376, 319, 57 bp). There was a significant difference in the genotype distribution ( 2 =8.48, p=0.014) between healthy controls and CP patients for the CRP polymorphism here considered. There were no differences in terms of frequency of the G/C alleles ( 2 =0.05, p=0.8224): for the G vs C allele, the OR of the control vs the CP group was 1.037 (95% CI=0.756-1.421).
Distribution of the VEGF polymorphism at position -936
With regard to the polymorphism of VEGF at position -936 we found a less significant, but still suggestive, difference between healthy controls and CP patients in the genotype distribution ( 2 =7.68, p=0.022), and a significant difference in the allele frequency ( 2 =10.12, p=0.001) (Tab. III). For the C vs T allele, the OR for the control vs CP group was 0.591 (95% CI=0.427-0.819).
Distribution of the -defensin-1 polymorphism at position -1654
Regarding the distribution of the -defensin-1 genotypes at position -1654, there was a significant difference between CP patients and healthy controls ( 2 =43.85, p<0.001). For the -defensin-1 AA genotype, the frequency was 64.8% in the CP group and 35.2% in the control group. The frequency of the G allele for -defensin-1 was also significantly higher in the CP group (71.3%), than the control group (40.2%) (Tab. III). The chi-square test resulted in a 2 =77.2, and a p<0.001; the OR between the CP and the control group was 0.591 (95% CI=0.427-0.819), indicating a significant difference between the 2 groups.
Table IV shows the serum levels of IL-6, IL-12, CRP, VEGF and -defensin-1 in the control and CP groups and their statistical comparison. Highly statistically significant differences in the serum levels of IL-6, IL-12, CRP, VEGF and -defensin-1 were demonstrated between the 2 groups (p<0.001; Tab. IV).
SERUM LEVELS OF IL-6, IL-12, CRP, VEGF AND β-DEFENSIN-1 IN THE HEALTHY CONTROL (H) AND CHRONIC PERIODONTITIS (CP) GROUPS AND THEIR STATISTICAL COMPARISON
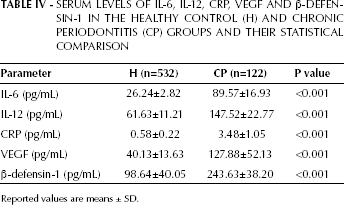
Reported values are means ± SD.
Discussion
Periodontal disease is initiated by the accumulation of plaque bacteria in the gingival sulcus that induces an inflammatory response (3). The individual inflammatory response induced by the pathogens seems to play a critical role in disease pathogenesis (33). Recent evidence has indicated that patients with severe periodontitis have a perturbation of their systemic inflammatory status manifested by increased serum levels of IL-6, IL-1, CRP, fibrinogen and moderate leukocytosis compared with unaffected control populations (34-36). These observations have raised the hypothesis that periodontal infections may significantly contribute to the overall inflammatory burden of the individual.
Cytokines, such as IL-6 and IL-12, and CRP are generally considered to be the most sensitive markers of the acute phase response to infections and inflammation (37). IL-6 is a multifunctional cytokine that regulates immune responses and its effects overlap those of IL-1 and tumor necrosis factor (TNF). It is widely distributed among cells of the periodontium and is thought to play a role in the elevated B-cell response observed in the gingival tissues of patients with CP. In this study, the G/G genotype for the IL-6 gene was statistically associated with susceptibility to CP (OR=3.80, p<0.001), suggesting that the G allele may play a role in the pathogenesis and development of periodontal disease. Fishman et al (16) found G/G homozygote individuals showing circulating IL-6 concentrations approximately twice as high as those with the C allele. After a given inflammatory stimulus, the presence of the C allele would result in a lower IL-6 expression than in the case of the G/G genotype. In our study, the serum level of IL-6 in CP patients was 3 times that in healthy controls (89.57±16.93 vs 26.24±2.82). These findings are in accordance with previously published data (16).
Although IL-12 is a key factor in cell-mediated immunity, and an association between the severity of periodontal disease and IL-12 has been already suggested (38), only few studies have been conducted with regard to the association of the IL-12 gene polymorphisms and periodontal disease. Hu et al (39) found a correlation between IL-12 gene polymorphism at position -1188 and periodontitis in a Taiwanese population. In our study, CP patients expressed higher serum levels of IL-12 than the control group. Individuals who express high levels of IL-12 might be more susceptible to CP as a result of the proinflammatory role of IL-12.
In our study, A/G allele frequencies for the CRP gene exhibited no differences between healthy controls and CP patients. However, the serum levels of CRP showed a significant difference between these 2 groups. Our results confirmed those of Paraskevas et al (40). Analogous to the hypothesis that some infectious and inflammatory diseases may be associated with cardiovascular disease, it is conceivable that the chronically elevated CRP levels in periodontitis patients exacerbate ongoing inflammatory processes in atherosclerotic lesions, thereby increasing cardiovascular and cerebrovascular risks.
VEGF has the ability to increase vascular permeability, because it contributes to inflammation in the early stages of periodontal disease. The role of VEGF in the pathogenesis of periodontal disease showed conflicting results, as VEGF expression increased (41), decreased (42) or was unaffected (43) during the manifestation of the disease. The VEGF level was found to be higher in the CP group of this study. Increased VEGF levels may be caused by induction of either proinflammatory cytokines, such as IL-6 and IL-1 (44), or periodontopathic pathogens.
Odds demonstrated that expression of -defensin-1 varies between individuals, even though this is considered to be a constitutively expressed peptide (45). The variability of expression may be associated with changes in the portion of the gene with the SNP, such as the -defensin-1 G/A alleles at position 1654. The distribution of the G/A alleles for -defensin-1 was significantly associated with CP, and -defensin-1 serum levels were also higher in CP patients. G/A substitution may have an effect on the folding of the peptide and, thus, influence the peptide function (46).
CONCLUSION
As demonstrated in our study polymorphisms in IL-6 (position -174), IL-12 (position -1188), CRP (position -717), VEGF (position -936) and -defensin-1 (position -1654) and their protein levels were associated with a risk of developing CP.