
Abstract
Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 infection, has led to a pandemic of acute respiratory illness. Pharmacologic treatments for COVID-19 have included treatments that target infection prevention, prevention of viral replication, reduce inflammation, and manage symptoms of respiratory failure caused by the disease. This is a review of key pharmacologic treatments for COVID-19 based on peer-reviewed articles from 2020.
Introduction
The novel coronavirus, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), was first identified in Wuhan, China, at the end of 2019. 1 Since that time, it has affected > 100 million people around the world, which led to > 2 million deaths. 2 The virus causes an acute respiratory illness that the World Health Organization has termed coronavirus disease 2019 (COVID-19). Due to the severity and effects of this illness, great efforts have been undertaken to identify effective pharmacologic therapies to prevent infection, prevent viral replication, prevent damaging inflammation, or to manage the symptoms of respiratory failure caused by the virus.
This review includes 6 pharmacologic treatments currently being used in the management of patients with COVID-19. Remdesivir, REGN-CoV-2 (Regeneron Pharmaceuticals, Tarrytwon, NY), and Optate (Airbase Breathing Company, Indianapolis, IN) directly target viral infection and replication. Dexamethasone is a corticosteroid that reduces inflammation after infection. Oxygen and inhaled pulmonary vasodilators are used to treat and manage respiratory symptoms in patients with COVID-19. The purpose of this article is to review the literature available in the past year with regard to these pharmacologic therapies for COVID-19. Recent pharmacologic treatment strategies for COVID-19 are also summarized.
Methods
Pharmacologic agents included in the National Institutes of Health COVID-19 Treatment Guidelines 3 with the most supporting evidence at the time of this publication were included in this review. A PubMed search was conducted to identify articles published in 2020 that related to these COVID-19 pharmacologic treatments. Searches were conducted by using the key words “remdesivir,” “REGN-CoV-2,” “Optate,” “dexamethasone,” “oxygen” and “inhaled pulmonary vasodilators” in conjunction with “COVID-19.” A summary for each of the reviewed pharmacologic agents, based on the findings of this literature search, is included below.
Discussion
Remdesivir
Remdesivir is an intravenous prodrug of an adenosine analog that incorporates into viral RNA and results in premature termination. It has a broad-spectrum antiviral activity against several viruses, such as respiratory syncytial virus, Nipah virus, Ebola virus, Middle East respiratory syndrome, and severe acute respiratory syndrome coronavirus-1 (SARS-CoV-1). 4-6 Remdesivir was authorized for emergency use by the FDA in May of 2020 for hospitalized adults with severe COVID-19. This emergency use authorization led to a double-blind, randomized, placebo controlled trial sponsored by the National Institutes of Health. 7
This initial trial enrolled hospitalized adults with confirmed cases of COVID-19 and evidence of lower respiratory tract infections, treated them with either 10 d of remdesivir or placebo, and monitored their time to recovery. 7 In this study, the subjects who received remdesivir had a significantly decreased median recovery time versus the subjects who received the placebo (95% CI 9–11 d vs 95% CI 13–18 d) (Fig. 1). 7 The subjects who received remdesivir were also more likely to have clinical improvement at day 15 (odds ratio 1.5, 95% CI 1.2–1.9; after adjustment for disease severity) when compared with those treated with placebo. 7 Although there was no statistically significant difference in mortality noted between the 2 groups, the investigators concluded that remdesivir shortened the time to recovery and hastened clinical improvement when compared with the placebo group and may have prevented progression to more serious illness in some cases. 7
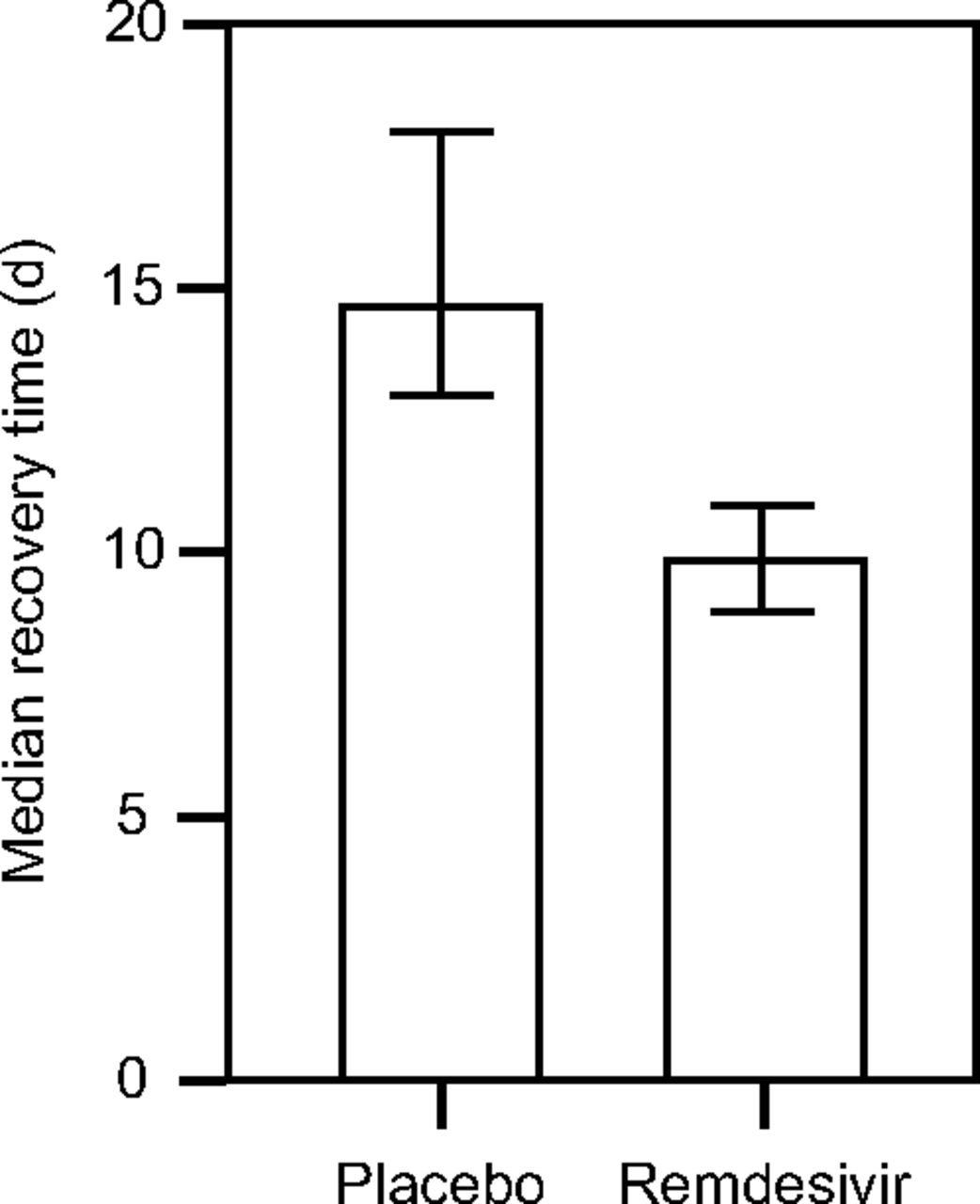
Remdesivir shortens the time to recovery in patients with coronavirus disease 2019 (COVID-19). The subjects who received remdesivir had a median recovery time of 10 (95% CI 9–11) d compared with the subjects who received the placebo whose median recovery time was 15 (95% CI 13–18) d. Data from Reference 7.
A subsequent trial evaluated different courses of remdesivir (5 vs 10 d), compared against each other and the standard of care. 8 The subjects who received 5 d of remdesivir had significantly higher odds of having a better clinical status than those who received standard care alone (odds ratio 1.65, 95% CI 1.09–2.48; P = .02). Of note, those who received 10 d of remdesivir therapy did not show a statistically significant difference when compared with the standard of care group (P = .18) and there was no significant difference in mortality among the 3 groups after 28 d. Although results of repeated studies suggest that remdesivir is a promising therapy for COVID-19, ongoing studies are needed to determine whether it reduces mortality. 8
REGN-CoV-2
REGN-CoV-2 is an antibody cocktail that prevents viral entry into human cells via the angiotensin-converting enzyme 2 receptor. It is made up of 2 noncompeting, neutralizing human immunoglobulin G1 antibodies, REGN10933 and REGN10987, that target the SARS-CoV-2 spike protein. 9 Viruses mutate frequently, which may result in new mutant viruses that are not affected by a specific antibody, a process known as viral escape. By combining ≥ 2 antibodies, a therapy is less vulnerable to viral escape because the virus would have to mutate in multiple specific ways. 10 Initial trials evaluated the effects of 8.0 or 2.4 g of REGN-CoV-2 compared with placebo on non-hospitalized subjects with COVID-19. The subjects who received either dose of REGN-CoV-2 had a significantly decreased SARS-CoV-2 viral load than those who received the placebo (95% CI −1.02 to −0.11) (Fig. 2). In addition, medical visits for COVID-19 were significantly decreased in the subjects who received REGN-CoV-2 than in those who received the placebo (95% CI −29 to 11). 11 As with remdesivir, further studies are needed to determine the effects of REGN-CoV-2 on mortality in patients with COVID-19.
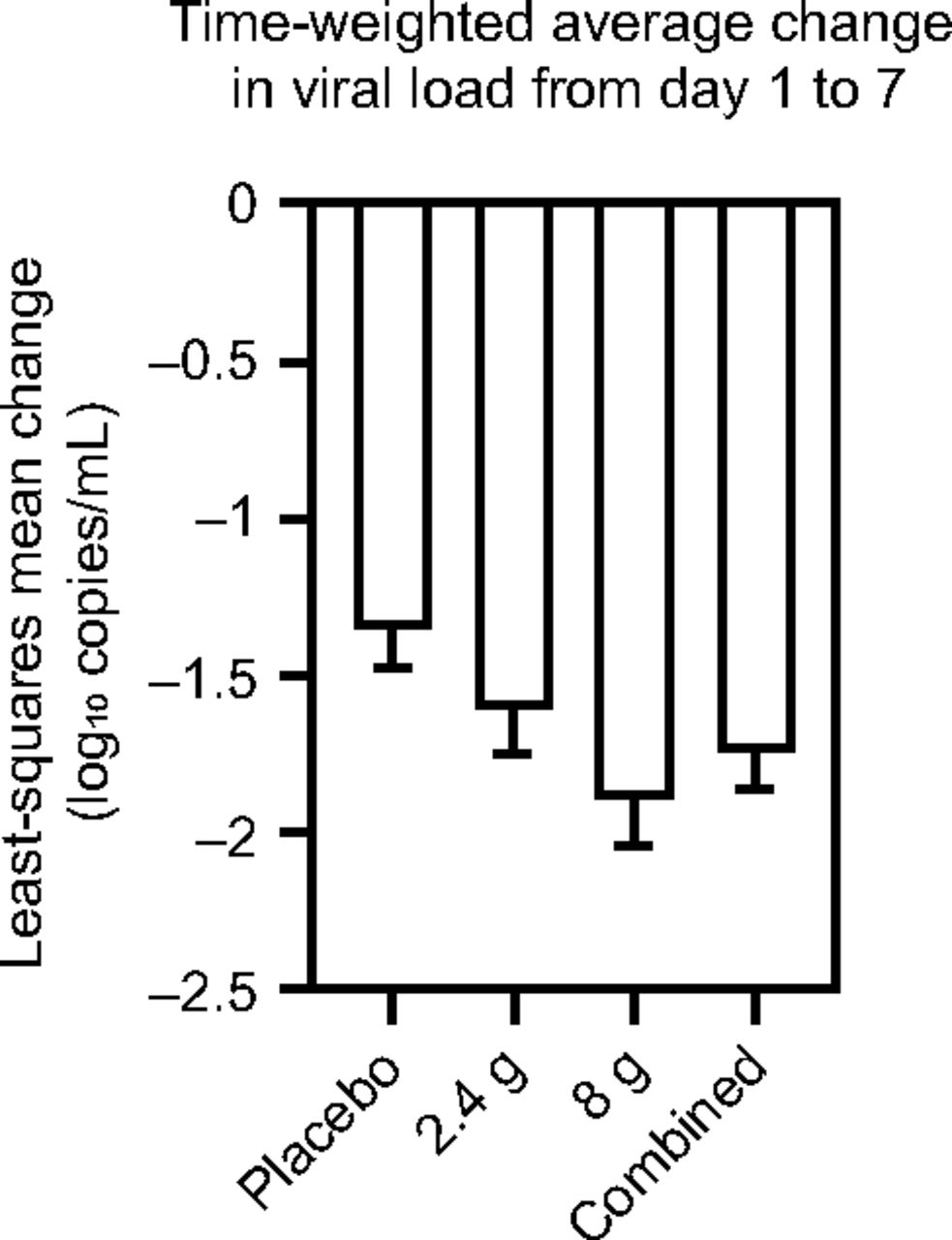
REGN-CoV-2 significantly decreases the viral load compared with placebo. The time-weighted average change in viral load from day 1 to day 7. The subjects who received REGN-CoV-2 had a significantly decreased severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) viral load than those who received the placebo (95% CI −1.02 to −0.11). Data from Reference 11.
Optate
Optate is an inhaled isotonic, isosmotic, alkaline medication designed to safely raise airway pH without irritating the airway epithelium. Raising intracellular pH partially prevents activation of SARS-CoV-2 in normal primary human airway epithelial cells, which decreases viral replication by altering endosomal trafficking and preventing viral entry and replication. 12 Optate has previously been shown to be safe to inhale in healthy human subjects and in those with stable airways disease. 13 These studies also demonstrated that Optate raised airway lining fluid pH, with it’s airway epithelial extracellular pH. In 2020, in vitro studies demonstrated that Optate also safely increases intracellular pH of normal primary human airway epithelial cells. Optate also ablated SARS-CoV-2 viral infection and replication in normal primary human airway epithelial cells after 48 h compared with placebo (P < .001) (Fig. 3). Due to its demonstrated safety profile in humans and antiviral effects in vitro, Optate inhalation may be well suited for a clinical trial in patients with COVID-19 infection. 14
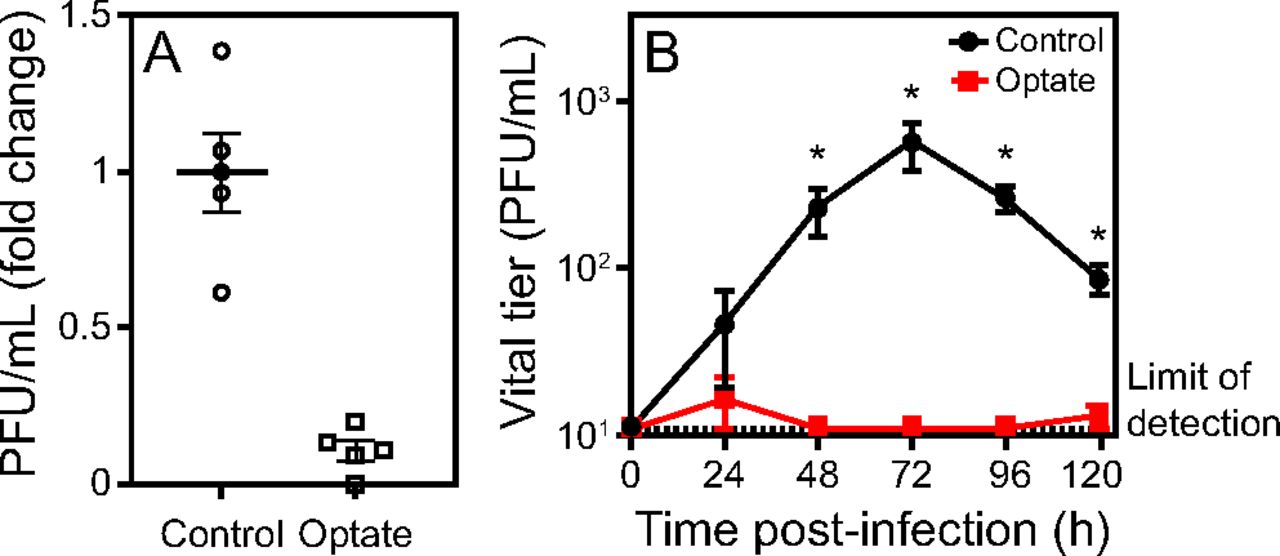
Optate decreases severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) viral replication in Vero E6 and normal primary human airway epithelial (NHAE) cells. A: PFUs were measured in culture media from control and Optate-treated Vero E6 cells infected with SARS-CoV-2. Optate ablated viral infection in the Vero E6 cells (P < .001). B: Control and Optate-treated primary NHAE cell cultures were infected with SARS-CoV-2, PFUs in culture media were analyzed under similar conditions for 120 h, starting from 24 h after infection. After the infection was established (24 h), viral infection was ablated in the Optate-treated cells (P < .001). PFU, Plaque forming units. From Reference 14.
Dexamethasone
Dexamethasone is a potent corticosteroid with anti-inflammatory properties that has often been used as a supplemental treatment for viral pneumonia. 15 Inflammation is a known component of COVID-19, which leads to rationale of dexamethasone as a potential therapy. 16 The RECOVERY Trial Collaborative Group 17 performed a randomized controlled, open-label trial that compared subjects treated with oral or intravenous dexamethasone (6 mg daily for up to 10 d) to those who received the standard of care alone and assessed mortality at 28 d. They found that those who received dexamethasone had significantly decreased mortality within 28 d versus those who received the standard of care (22.9 vs 25.7%; age-adjusted rate ratio, 0.83; 95% CI 0.75–0.93; P < .001) (Fig. 4). The subjects who required mechanical ventilation at the time of randomization also had lower mortality rates when receiving dexamethasone therapy versus the standard of care (29.3 vs 41.4%; rate ratio 0.64, 95% CI 0.51–0.81) (Fig. 4). Similarly, those who received noninvasive oxygen therapy at the time of randomization had lower mortality rates when they were randomized to the dexamethasone group (23.3 vs 26.2%; rate ratio 0.82, 95% CI 0.72–0.94) (Fig. 4). Of note, this decrease in mortality was not noted in the subjects who did not require oxygen therapy at the time of randomization (17.8 vs 14.0%; rate ratio 1.19, 95% CI 0.92–1.55) (Fig. 4). 17
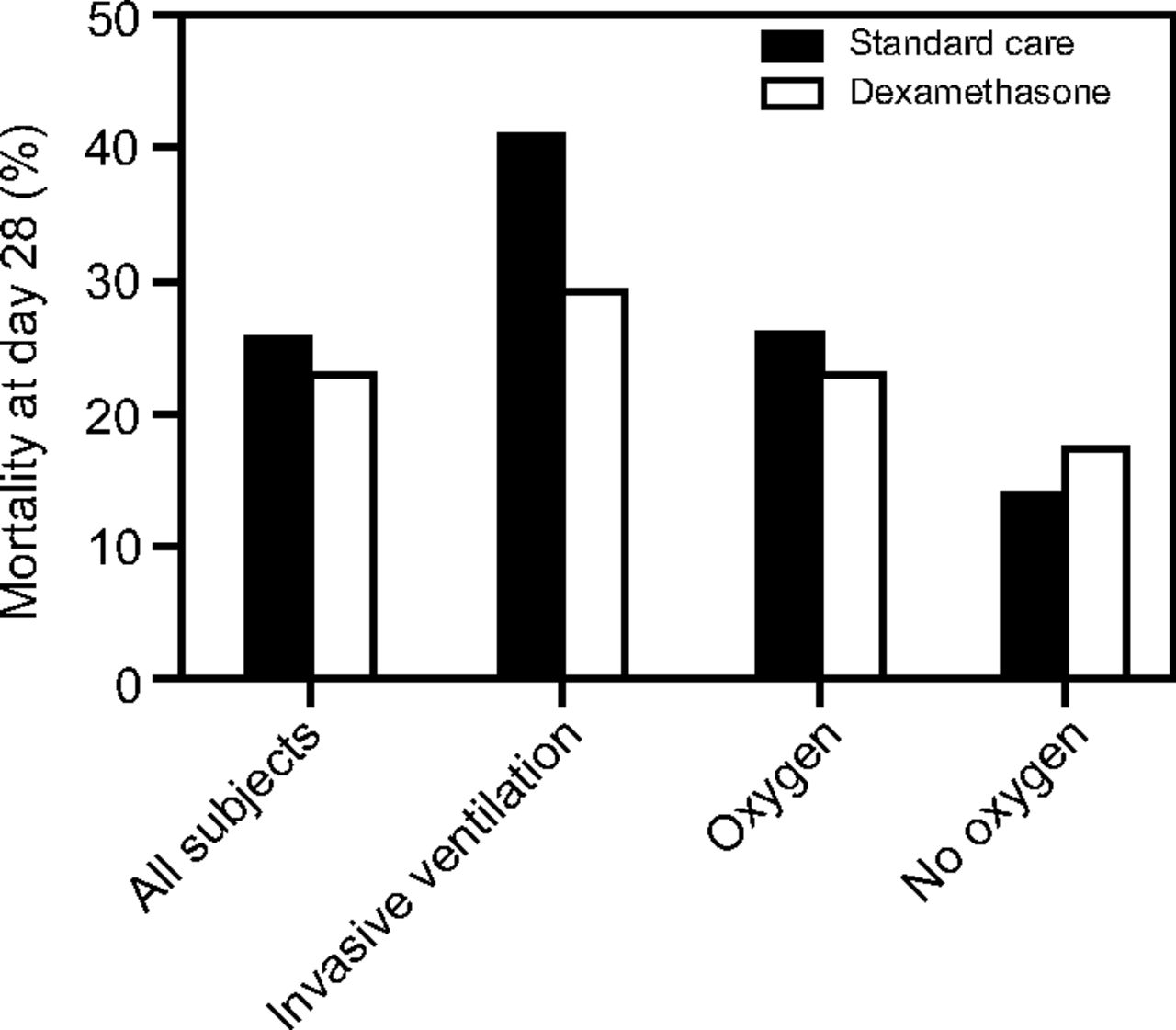
Dexamethasone decreases mortality in hospitalized patients with coronavirus disease 2019 (COVID-19). Shown is the effect of dexamethasone on 28-d mortality according to respiratory support at the time of randomization. Subgroups included all the subjects, those who were undergoing mechanical ventilation, those who were receiving supplemental oxygen, and those who were receiving no oxygen at the time of randomization. Data from Reference 17.
Oxygen
Hypoxic respiratory failure is a severe complication of SARS-CoV-2 and affects ∼19% of patients with COVID-19.
18
The Surviving Sepsis Campaign COVID-19 panel issued several recommendations with regard to oxygen use in adults with COVID-19, including start supplemental oxygen if start supplemental oxygen if maintain
There is some rationale for heightened caution of the overuse of supplemental oxygen therapy in patients with COVID-19 due to concern for upregulation of SARS-CoV-2 receptor expression in airway epithelium. Increased receptor expression could lead to increased susceptibility to SARS-CoV-2 infection. Myti et al
20
compared levels of messenger RNA for genes encoding SARS-CoV-2 receptors in lung cells of mouse pups and preterm human infants exposed to chronically elevated
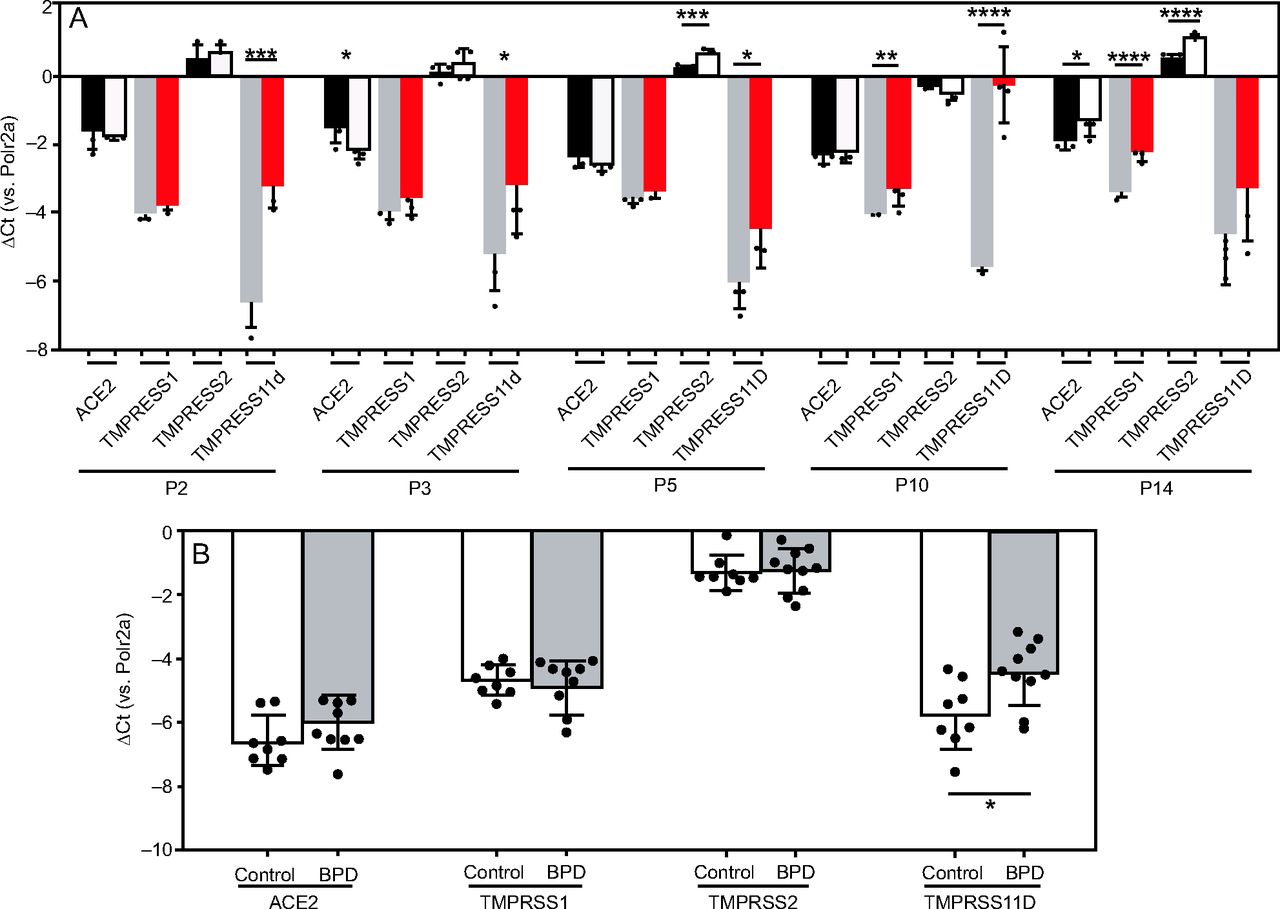
Steady-state levels of lung messenger RNA (mRNA) transcripts encoding severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) entry receptors and co-receptors in experimental animals and clinical subjects chronically exposed to elevated
Inhaled Pulmonary Vasodilators
Inhaled pulmonary vasodilators have been shown to improve oxygenation and
Franco et al
21
explored the mechanism of action of several inhaled pulmonary vasodilators and current ongoing clinical trials. They discussed the potential benefits of nitric oxide for patients with COVID-19 by directly treating endothelial dysfunction/
Summary
In 2020, several pharmacologic agents were identified and trialed for use in patients with COVID-19. Several of these treatments target viral replication, inflammation, and symptom management. Due to the ongoing nature of this novel pandemic, recommendations for treatment of patients with COVID-19 are ever evolving. The most up-to-date guidelines from the National Institutes of Health can be found at https://www.covid19treatmentguidelines.nih.gov/, Accessed March 17, 2021. Knowledge of therapeutic options and best practice of their use is crucial for battling this pandemic. Of note, at the time of this publication, vaccination against SARS-CoV-2 is recommended as an effective prevention of COVID-19. 24
Footnotes
Dr Davis is funded by the National Heart, Lung, and Blood Institute 1 P01 HL128192 and P01 HL158507, the Indiana Clinical and Translational Sciences Institute UL 1 TR002529; he also is a patent holder of Optate and a co-founder of Airbase Breathing Company. Dr Saunders is funded by the Cystic Fibrosis Foundation First and Second Year Clinical Fellowship Grant.