
Abstract
Current estimates of the prevalence of opioid withdrawal in newborns from the 2012 Better Outcomes Registry and Network Ontario reveal that more than 4 births per 1000 display recognizable symptoms of neonatal abstinence syndrome (NAS). With a growing consensus surrounding aspects of newborn opioid withdrawal care, clinicians might agree that all infants exposed to maternal opioids require supportive observation and care to ensure appropriate adaptation and growth in the newborn period and, likewise, that there exists a smaller percentage of newborns who require additional pharmacotherapy. However, due to the dearth of comparative studies of NAS tools, there remains a lack of evidence to support the use of a specific NAS method of scoring or treatment. Two types of NAS treatment protocols currently in use include a symptom-only versus weight-based protocols. Our Neonatal Intensive Care Unit (NICU) has used both models. A formal structured NAS tool and weight-based morphine delivery system began in our NICU in 1999. We audited all newborns with known exposure to maternal opioids in our NICU from the years 2000 to 2014. The Finnegan scoring tool was used throughout all years of the chart audit. Modifications made to the Finnegan scoring tool from the MOTHER study were adapted for use in our NICU at the same time as adopting the Johns Hopkins model of symptom-only based morphine delivery in 2006. The objective of this comparative study using a retrospective chart audit is to compare length of stay (LOS) and total accumulative morphine dose across these two morphine delivery protocols. Our audit revealed that there were a significantly higher proportion of newborns in the symptom-only model that received morphine and, perhaps accordingly, also had a significantly higher LOS compared to those in the weight-based model. Comparing only those infants who did receive morphine, the comparative total accumulative dose of morphine and LOS were not significantly different between the weight-based and symptom-only morphine delivery models.
Introduction
The incidence of neonatal abstinence syndrome (NAS) secondary to opioid withdrawal is more than 4 cases per 1000 deliveries in Canada and the US. 1 This translates to an estimated 3%–4% of NICU beds at any given time being utilized for these infants, leading to increased health care expenditures due to prolonged hospital admissions for the management of NAS.4,5
Since the inception of neonatal abstinence tools, there has been a growing evolution toward embracing, where possible, a consensus in the care of newborns with opioid withdrawal. Most, if not all, opioid-exposed infants experience NAS to some degree, 6 which occurs with notable heterogeneity.2,7,8 Furthermore, NAS severity has not been related to maternal methadone dose or cumulative methadone exposure in utero. 9 Most NAS management recommendations suggest that nonpharmacologic therapy should be the standard of care for all opioid-exposed infants.3,10–12 For a subset of infants with NAS, nonpharmacologic therapy alone is insufficient to prevent significant morbidity, and institution of appropriate pharmacologic management is indicated.3,13,14 Most pharmacologic treatment strategies include the use and gradual weaning of a single opioid.10,12,15,16
There are two different strategies for evaluation and treatment of NAS: a weight-based scale, in which medication is dispensed on a milligram per kilogram basis, and a symptom-based scale, in which medication dose is determined by NAS score. 13 These two regimens vary in terms of the recommended initial dose, dose increments, weaning dose, and initiation of adjunctive treatment (Table 1). No standardized approach has been determined due to lack of comparative studies. Furthermore, there are limited studies providing evidence for morphine doses used in either model. On comparing discharge strategies, the accumulative morphine dose of inpatient and combined in- and outpatient models has been described to be around 3.2–3.6 mg/kg/day. Daily doses of morphine ranged from 0.24 to 1.3 mg/kg/day.17,24
Comparison of NAS models.

Since there have been no comparative studies of these two protocols, the objective of this study was to compare NAS outcomes consisting of morphine doses and length of stay (LOS) for the two models of morphine delivery.
A Brief History of NAS at St. Joseph's Health Centre
Our hospital developed the Toronto Centre for Substance Use in Pregnancy (T-CUP) in 1997. 18 With the growing number of women attending T-CUP with a diagnosis of opioid use disorder, so did the census of newborns with NAS. There were frequent occasions during which infants with opioid withdrawal NAS took up to 25% of our given daily census. As a result, we began using a formal structured NAS tool and weight-based morphine delivery system in our NICU in 1999. The Finnegan scoring tool was used until a modified scoring tool was adapted. As a site for the MOTHER study, the NICU switched to the Johns Hopkins model of symptom-only based morphine delivery 13 in 2006.
Our protocol of NAS opioid withdrawal treatment, whether weight based or symptom only, used a monotherapy of morphine sulfate 0.5 mg/mL. Clonidine was used as a co-therapy when the total daily dose of morphine reached 1 mg/kg/day, regardless of morphine delivery model. The protocol did not use barbiturates or benzodiazepines for opioid withdrawal. No infants were discharged from the hospital with prescribed opioid therapy. Infants with known methadone exposure were observed for a minimum of 120 hours. Discharge occurred from hospital after a minimum of 48 hours after discontinuation of morphine.
In our participation in the MOTHER trial, our NICU group believed that the changes to the Finnegan tool, now renamed the MOTHER NAS scale, 12 would result in reductions in the degree of subjectivity needed to measure previously problematic items. Specifically, the MOTHER NAS scale clarified certain items like “tone”, “crying”, and “irritability” that were confusing and subject to inflation by adding objective and concrete descriptions. Further, an experienced rater could modify intermediate scores potentially inflated by “everyday baby crankiness.”
Despite the provincial consensus recommendation to use the Finnegan scoring tool, we remained the only NICU in Ontario using this morphine delivery model. As a result, it became important to discover whether there were differences in how LOS and accumulative morphine were affected by use of these variable morphine delivery systems.
At the onset of the audit, we postulated that the LOS would not be different between the two models. In the symptom-only morphine delivery model, there were babies who would proceed with successful and structured morphine administration and weaning, only to be discharge ready and 48 hours free of morphine, well under our usual expected LOS of 2–3 weeks in these babies. However, we speculated that the audit might not demonstrate a difference in the total amount of morphine delivered between the two cohorts of morphine delivery models.
A stringent NAS treatment and weaning protocol, rather than the particular opioid chosen for treatment, has been shown to be the most important predictor of length of stay and duration of opioid treatment. 10 Our intent of the audit was to shed light only on the choice of morphine treatment and weaning protocols. We postulated that our retrospective chart audit would support that the adoption of a structured model of morphine delivery – be it weight based or symptom-only based, in concert with an accepted neonatal scoring tool like the Finnegan – would result in a similar LOS and accumulative morphine dose. We conclude with recommendations reflected by our audit with respect to a chosen morphine delivery model and discuss the resource management decisions resulting from the audit.
Methods
All newborns born in our hospital from January 1, 2000, to December 31, 2014, inclusive, and whose chart was coded with an ICD10 of P96.1, were identified. A total of 278 charts were flagged for audit during this time period. Those infants exposed to maternal opioids through confirmed drug screen and or self-admitted use were included in the audit (n = 172). Maternal use of other drugs and antidepressant use during pregnancy were captured by either self-report and/or by positive maternal or infant toxicology testing.
Preterm infants with less than 37 completed weeks of Gestational Age (GA) were excluded (n = 23). Any newborn considered to have a condition whose neurologic status would interfere in a proper assessment of neonatal withdrawal was excluded (ie, pain from birth trauma, lethargy from sepsis [n = 2]). Any newborn, whose care required transfer to another NICU, and therefore whose medication administration records could not be assessed in our hospital audit, was also excluded (n = 1). The total number of newborns' charts audited was 146. This research was approved by the Research Ethics Board of St Joseph's Health Centre.
Measurements of Primary Outcomes
Primary outcomes measured were the length of stay (LOS) and the total (all inhospital) accumulative morphine dose used for each newborn. Information for infants' LOS was derived from hospital discharge face sheets. Two parts of a newborn's flagged chart were used to obtain the peak NAS score and the total accumulative morphine dose: the baby's medical administration record and our handwritten NAS scoring records. Each morphine dose from the newborn's medication administration record was added to create a total accumulated morphine dose. This total dose is also displayed in milligrams per kilogram of birth weight. The time of the documented peak NAS score was measured in hours of life.
Statistical Methods
Categorical descriptive variables are summarized using counts and percentages, and group comparisons were carried out using a chi-square test. Continuous variables are summarized using medians and interquartile ranges; groups were compared using a Wilcoxon signed-rank test.
Results
Demographics
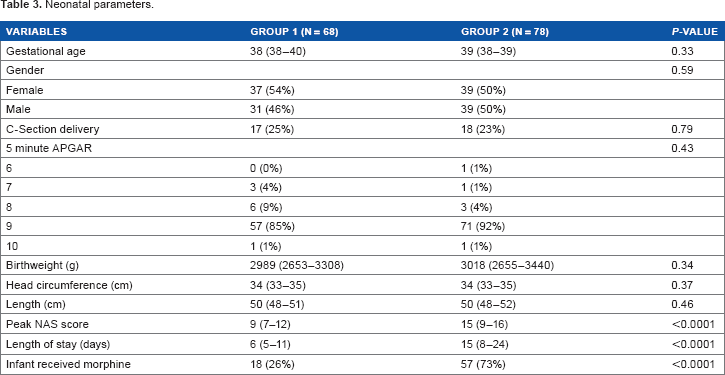
Tables 2 and 3 show the variables collected for the mothers and babies at birth, respectively. Group 1 represents the cohort of mothers and their babies who received morphine using the weight-based delivery system. Group 2 represents the cohort of mothers and their babies who received morphine based on the symptom-only delivery system. The LOS and peak NAS scores of infants audited, broken down by group, are shown in Table 3.
Mother demographics: N (%) or median (25th & 75th percentiles) are reported.

Neonatal parameters.
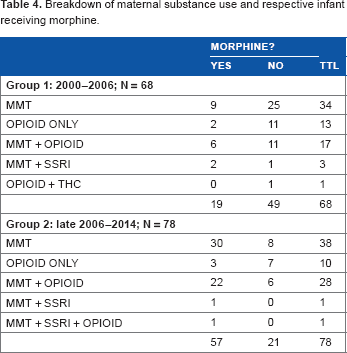
There was no statistically significant difference in the mother's age, mode of delivery, or methadone use between the two groups. Table 4 shows the breakdown of the maternal sources of opioids. There was no statistical difference in the proportions of the mothers on Methadone Maintenance Treatment (MMT) and/or opioids.
Breakdown of maternal substance use and respective infant receiving morphine.
There was no statistically significant difference in the descriptive parameters collected for the babies between the two groups.
There was no statistically significant difference in the age or their opioid use in the mothers whose babies received morphine (Table 5). This holds true when considering each opioid on its own and considering the combination of opioids which the mothers may have used.
Mothers of infants who received morphine.

Assessment of Initiation of Morphine
Table 6 shows the breakdown of the LOS, peak NAS score, timing of morphine initiation, and total accumulative morphine in those babies who received morphine in their group.
Infants who received morphine.

The symptom-only model was associated with a greater proportion of babies assessed as requiring morphine initiation. One might expect that a system that appears to have a lower initiation threshold – that is, only needing one score of 9 versus two or three consecutive scores of 8–11 – might be associated with a greater tendency to initiate morphine administration. However, there was no statistically significant difference in the timing of morphine initiation between the two models in those babies who received morphine (Table 6).
Babies in the symptom-only group were more likely to receive morphine: (odds ratio [OR] = 7.0; 95% confidence interval [CI] = 3.4, 14.5; P < 0.001).
Babies with mothers on MMT were more likely to receive morphine: (OR = 5.3; 95% CI = 1.9, 15.1; P = 0.002).
There was no relation between babies receiving morphine and maternal opioid, Selective Serotonin Re-uptake Inhibitors (SSRI), or Tetra Hydro Cannabinoids (THC) use.
The relationship between babies' morphine receipt, group and MMT were independent, in that after controlling for group, babies whose mothers were on MMT were more likely to receive morphine. Regardless of mother's MMT use, babies in the symptom-only group were also more likely to receive morphine. There was no interaction between group and MMT use.
ORs were similar in the multivariable logistic regression model: Symptom-only group: OR = 7.2; 95% CI = 3.4, 15.5; P < 0.001. Maternal MMT: OR = 5.7; 95% CI = 1.8, 17.8; P = 0.003.
Los, Morphine Onset, and Total Dose
Recent reports on LOS for NAS suggest an average LOS of 15–17.5 days.3,11 This LOS is longer than the average LOS for all cases in a community NICU of 8–9 days. 4 On first inspection of both entire cohorts, the LOS was significantly less in the weight-based cohort. However, the proportion of morphine-treated newborns was also statistically different between the two cohorts. There were a significantly increased number of morphine-treated infants in the symptom-only based model. Interestingly, those infants who received morphine in the symptom-only model, did so at a similar onset of time, and required as much morphine as those who received morphine in the weight-based model, and had similar lengths of stay.
In our experience, some babies in the symptom-only model received prompt morphine at a dose lower than the lowest dose in the weight-based model and were weaned and discharged on par with regular NICU benchmark parameters.
Closer inspection of the symptom-only cohort showed that out of the 57 who received morphine, 5 never reached a dose that represented the lowest dose in the weight-based model (0.32 mg/kg/day). It appears though that these noteworthy cases occurred in a cohort that still had a skew toward both a higher LOS and a higher peak NAS score than the weight-based model.
Peak NAS Score
The symptom-only cohort had a significantly higher median NAS score than that of the weight-based model. Even comparing those newborns who received morphine, and in particular where their LOS and timing of morphine onset and total accumulative morphine were not statistically different, those infants in the symptom-only group still had a higher peak NAS (Table 6). This skew toward a higher NAS score in the symptom-based model, in a cohort that already has a propensity to capture more morphine-treated newborns, might also contribute to an increased LOS in that whole cohort.
Discussion
The overwhelming majority of research and clinical practice since the inception of the Finnegan scoring tool has engaged in some form of weight-based morphine dosing. 21 While the data quality of this audit is boosted by the size of the cohorts, the confidence in the observational data 20 might be described as moderate at best. Accordingly, generalizations gleaned from this audit should mainly be considered when treating a comparable demographic of opioid-exposed newborns from mothers followed in a specialized substance use in pregnancy clinic.
Recommendations derived from this audit might vary depending on the stakeholders involved. A practitioner concerned with the risk of delivering morphine to a newborn in opioid withdrawal, where there exists no standard model, might be relieved to know that there is no difference in the total morphine dose used to treat opioid withdrawal using either model.
Since this practitioner might also be accountable to a budgetary purse-string, the longer LOS in the symptom-only cohort might make its choice as a morphine delivery model too costly until subsequent studies further illuminate this model's patterns of neonatal withdrawal. The symptom-only model appears to have a possibly large propensity toward a higher LOS, which obligates further prospective audits to rule out a possibly false lack of difference of LOS and morphine dose in those babies who did receive morphine.
The barriers that contribute to the lack of comparative studies on the consensus of morphine delivery systems in the NAS literature are inevitable but nonetheless malleable with discussion. The heterogeneous presentation of neonatal opioid withdrawal does not inspire a hospital to readily expend resources to randomize morphine delivery to their newborns concurrently. Further, as we continue to define quality of evidence with disproportionate volumes of citations modified through the GRADE 20 lens, the resulting creation of “weak” and “conditional” recommendations creates equal parts woe and inspiration to audit their care.
We could not control for timely discharges of mothers before the desired duration of neonatal observation was completed. We did not record the temporal dispersion of the babies' hospital admissions. Given the propensity for a mother in the symptom-only group to have her baby need morphine, it is possible that our not being able to house all mothers with their withdrawing newborns might be a cause of that group's inflated NAS scores.
This audit did not include the disposition of the infants to home or social services. Based on the quality of documentation before 1999, we were unable to audit the comparison of the LOS and total accumulative morphine before and after the implementation of our protocol. We chose to audit only the babies' charts for purposes of resource expenditure. The all-paper charts of the babies did not sufficiently include the mothers' antenatal records to properly assess maternal use of cigarettes or race. However, even if said reports were present in the babies' charts, (1) some antenatal records were incomplete and (2) free-form answers to “race/ethnicity” were often reported with only names of countries of origin.
The use of a stringent weaning protocol, rather than the particular opioid chosen for treatment, has been shown to be the most important predictor of length of stay and duration of opioid treatment. 10 However, this argument was developed in centers comparing these outcomes before and after a formal adaptation of a neonatal opioid abstinence protocol. Our audit reveals that length of stay (and hence duration of morphine) and total accumulative morphine might be affected by the choice of morphine delivery model. It is only when comparing those infants who did receive morphine, our audit revealed that there was no difference in their LOS or total accumulative morphine across the two groups of morphine delivery models.
Until such time we can prevent NAS, it remains important to find ways to better define and treat neonatal opioid withdrawal. Based on the results of our study, we offer the following recommendations toward this end.
If the responsibility in data collection already does not inspire a “clean while you cook” mentality in the clinical setting, the emergence of electronic charting might be a driver. It is of course implausible to anticipate all future modifications of study parameters, like mother's demographics, or changes to how we might measure and treat neonatal opioid withdrawal. Upon our ultimate commitment to an electronic charting system, it will be hard to embed future modifications of echarts without a sizable cost, and equally hard not to recommend concurrent use of paper documentation when and where NAS care is performed.
Last, we end with how this paper started: with the developed world lament of the resource expenditure of NAS, and our recommendations of delivering morphine to newborns in opioid withdrawal. The overall conditionality of the recommendation – the best an observational audit could yield using GRADE 20 – dictates the need for continued auditing of the model. The symptom-only model did not demonstrate any advantages with respect to LOS or morphine dose, which would not inspire a center to spend resources in converting from a weight-based to a symptom-based model. We believe that since the symptom-only model appears to have a greater propensity toward a higher LOS and NAS score, despite no apparent differences in other parameters, it obligates continued auditing. There is future direction in testing the sensitivities of these morphine delivery models as a possible explanation for the differences in NAS score.
Conclusions
In our locale, the result of the audit does not indicate a need to discontinue our current model of symptom-based morphine delivery. We do, however, want to substantiate our continued resource usage with the symptom-only model. Following the respective neonatal developmental outcomes may also become a factor in the choice of morphine delivery, if there exists a significant developmental outcome attached to its use.
This audit has motivated two movements in our organization. The first is a low cost but anticipated long-term gain in creating a system that can better collect and connect neonatal outcomes paired with their corresponding maternal demographics. Since the majority of our mothers in our audit attend our specialty clinic with notable compliance, we would like to collect more maternal determinants of health.22,23 To connect the maternal information with the corresponding infant, however, will require that our team add and absorb in-kind time needed to better keep track of these families' changing geography. With the uncertainty regarding our future electronic documentation, we continue to audit all of our information on paper.
The second initiative is one toward a structured sharing of resource intensity of NAS with an inpatient pediatric ward. We hope that this sharing will reduce the geographic barriers in providing optimal support of the mother–baby dyad while also improving the efficiency inherent in a pediatric ward with a labile census. We anticipate a large resource expenditure not only for the support of a new learning curve for the pediatric staff but also with the ultimate goal of having all care givers – in the NICU and pediatric ward – foster a structured integration of the newborns' family in our care of neonatal opioid withdrawal.
Author Contributions
Conceived the design of the data analysis: BC. Analyzed the data: BC, SL, SB, AO. Wrote the first draft of the manuscript: BC. Contributed to the writing of the manuscript: BC, SL, SB, AO. Jointly developed the structure and arguments for the paper: BC, SL, SB, AO. Made critical revisions and approved the final version: BC, SL, SB, AO. All authors reviewed and approved of the final manuscript.