
Abstract
Objective
The present study sought to examine the relations among disruptive behavior disorders (DBDs; ie, attention-deficit/hyperactivity disorder [ADHD], conduct disorder [CD], oppositional defiant disorder [ODD]), depressive symptoms, and marijuana use among a sample of late adolescents and emerging adults.
Method
A total of 900 students (75.8% female, 80.3% Caucasian, Mage = 20) from a large public university completed an online survey.
Results
Findings indicated that depressive symptoms mediated the relation between the marijuana use and past symptoms of ADHD, past diagnosis of ADHD, CD symptoms, CD diagnosis, and ODD diagnosis.
Conclusion
Depressive symptoms represent a link between DBDs and marijuana use that is suggested, but not well documented in the existing literature. The current findings add to this evidence and suggest a need to assess individuals presenting with symptoms of DBDs for depressive symptoms, as this symptom pattern may result in a greater likelihood of marijuana use.
Keywords
Introduction
SAMHSA reports that marijuana is the most commonly used illicit drug among Americans, with approximately 22 million past-month users. 1 Nearly 20% of 18- to 25-year olds report marijuana use. 1 Marijuana use specifically among college students is also prevalent. Approximately 14% of college students report past-month marijuana use, 2 and research suggests that one in four college students meets criteria for a marijuana use disorder. 3
Marijuana use among college students may be linked to academic impairment. In a study of full-time college students, researchers found that increased marijuana use was associated with lower grade point average. 4 Moreover, Martinez et al. 4 documented that the link between marijuana use and grade point average (GPA) remained even when accounting for core features of student identity (eg, sex, age, race, Greek involvement, family history of drug use). Clearly, marijuana use is problematic for many young people.
Although marijuana is increasingly becoming legalized by states in the U.S., its use remains illegal under federal law 1 and in many states. Therefore, it is important for both researchers and clinicians to investigate correlates of marijuana use in an effort to inform policy, prevention, and treatment.
Marijuana use and disruptive behavior disorders
Numerous studies have identified externalizing behaviors’ association with the onset of cannabis use disorders,5–9 with recent research among adolescents and young adults documenting that externalizing psychopathology was predictive of marijuana use disorders in the sample even after controlling for demographic variables and internalizing psychopathology. 10 Specifically, individuals with attention-deficit/hyperactivity disorder (ADHD), conduct disorder (CD), and/or oppositional defiant disorder (ODD) may exhibit defiance, aggression, and impulsivity. 11 Thus, ADHD, CD, and ODD may be collectively referred to as disruptive behavior disorders (DBDs). ADHD is frequently comorbid with marijuana use disorders. 12 ODD has been linked to marijuana use, as research indicates that adults suffering from severe aggression self-medicate with marijuana. 13 CD has also been linked to marijuana use. Adolescents with a childhood diagnosis of ADHD and concurrent CD had higher rates of past six-month marijuana use than adolescents with only an ADHD diagnosis and control adolescents. 14 It is clear that a link exists between marijuana use and DBDs, but it may be the case that a third variable impacts this link.
DBDs and depression
Depression is a potential link between DBDs and marijuana use. Research has identified significant diagnostic overlap between DBDs and depression, with 62% of individuals who met criteria for DBDs also exceeding threshold criteria for major depressive disorder. 15 Bagwell et al. 16 found that ADHD symptoms were related to risk for depressive symptoms among young adults. Furthermore, age of CD onset is significantly associated with increased probability of comorbid depression. 17 In a community sample of children, dimensions of ODD were associated with subsequent symptoms of depression as well. 18 While the literature suggests a correlation between DBDs and depression, a causal relation would lay the groundwork for depression as a mediator of the relation between DBDs and marijuana use. Indeed, recent research found that individuals with childhood ADHD experience significantly higher levels of depressive symptoms than comparison peers by 18 years of age. 19 Community and epidemiological samples have documented that conduct problems precede depression. 20 In a longitudinal study of child and adolescent girls, researchers used path analysis to establish a temporal relation between CD and depression, with CD often preceding depression from childhood to adolescence. 21 However, Hipwell et al. 21 concluded that the overlap between depression and dimensions of ODD accounted for the relation between CD and depression. Overall, existing research suggests that DBDs may precede the onset of depression, although there is still work to be done in elucidating these pathways.
Depression and marijuana use
Depressive symptoms are associated with frequency of marijuana use among adolescents and young adults. 22 Among adults, 3.4% of individuals diagnosed with major depression used marijuana weekly or more, a rate much higher than the 0.6% weekly prevalence among adults without mental illness. 23 In a review of the literature, Serafini et al documented that cannabis use is associated with suicidal behavior in samples of both psychotic and nonpsychotic individuals. 24 Research has also documented that adults with depression or symptoms of serious psychological distress had a lower odds ratio for quitting marijuana use compared to adults without these depressive symptoms. 25 Given that cannabis use is associated with risk for suicidal attempts 24 and individuals who use marijuana often experience comorbid symptoms of depression and psychological distress, 25 it is clear that a robust relation exists between depression and marijuana use.
The self-medication hypothesis
The self-medication hypothesis may explain the relations among DBDs, depression, and marijuana use. Khantzian 26 argues that individuals experiencing negative emotional states may use substances to alleviate such symptoms. The self-medication hypothesis has been studied extensively with marijuana use, and research has identified a link between marijuana use and depression.27–29 ADHD is associated with age-inappropriate levels of inattention and/or hyperactivity and impulsivity across two or more settings; thus, resultant impairment often includes increased risk of interpersonal conflict and poorer school performance and academic attainment. 11 Adults with CD may experience impairment across domains due to aggression, rule violation, and violence against others, while individuals with ODD may experience impairment due to conflict with authority figures, peers, and romantic partners. 11 Given that DBDs are associated with depression, it may be the case that impairment associated with DBDs leads to depressive symptoms.
Marijuana's positive subjective effects include euphoria, relaxation, and enhanced cognition and perception, whereas it's negative subjective effects include depression, anger, and anxiety.30–32 Previous research has found that marijuana use expectancies are predictive of actual use among both young adults with ADHD and a comparison sample. 33 Research has also documented that marijuana may be used to self-medicate problems with aggression. 13 Since individuals with DBDs and depressive symptoms are likely experiencing impairment across domains, marijuana use may be a means of coping with such impairment. Thus, impairment resulting from DBD symptoms may lead to symptoms of depression, which, in turn, leads to marijuana use.
Current study
Given the relationships among DBDs, depression, and marijuana use, the present study sought to investigate whether depression mediates the relationship between DBDs and marijuana use among a large sample of college students. While single relations have been documented to varying degrees in the extant literature, to our knowledge no published study has addressed the hypothesized pathway. Thus, our research question was threefold: Does depression mediate the relation between (1) ADHD and marijuana use? (2) CD and marijuana use? and (3) ODD and marijuana use?
Method
Participants and Procedure
Participants (N = 900, Mage = 20 years, 76% female, 80% Caucasian; Table 1) were recruited from a large Southeastern University. Specifically, participants were recruited via class Facebook pages (eg, Class of 2015), various schools on campus (eg, School of Business), the Psychology Participant Pool, and nonpsychology courses. Upon completion of the study, participants were entered into a drawing for a gift card. Some participants also received course credit for participation. The research complied with the principles of the Declaration of Helsinki.
Results of demographic analyses.

The survey was administered online through Qualtrics in 2014. In order to participate, respondents had to indicate that they were at least 18 years of age and enrolled as an undergraduate student. After completing the IRB-approved informed consent, participants were directed to the remaining survey questions. Most surveys took 30–45 minutes to complete.
As a validity check, a question about alcohol use was included twice in the survey. There were 17 questions between the first and second instance of this identical alcohol use question. For this specific question, there were 12 possible responses, ranging from “not at all” to “several times a day”. Responses of 35 participants were removed from the dataset to create the final N of 900; these participants were removed because they provided responses that were more than two answers apart on the alcohol use manipulation check.
Measures
Demographics
All participants were asked to indicate their gender, race, age, year in school, and family's annual household income. Demographic variables were selected in order to yield information regarding sample characteristics and socioeconomic status.
ADHD symptoms and diagnosis
The Current Symptoms Scale 34 (CSS) was used to assess for current ADHD symptoms. This scale asks the students to indicate their behavior in the last six months based on the 18 symptoms of ADHD from the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR), 35 rating “never or rarely”, “sometimes”, “often”, or “always” for each symptom. As specified in the CSS scoring instructions, 34 indicating “often” or “always” is considered endorsing that particular symptom. Students were also asked to complete the Childhood Symptoms Scale 34 for their behavior when they were 5–12 years old, using the same symptoms and response options as the CSS. 34 Both the current total symptoms (α = 0.94) and past total symptoms (α = 0.96) demonstrated strong reliability in the present study.
For the continuous measure of ADHD symptoms, the number of symptoms meeting threshold criteria (ie, “often” or “always” responses) was used. Students who endorsed (ie, indicated “often” or “always”) six or more current symptoms for either symptom domain (inattention or hyperactive/impulsive) were categorized as meeting symptom count diagnostic criteria for ADHD.
ODD symptoms and diagnosis
The CSS 34 was also used to assess for ODD symptoms. This scale asks the students to indicate their behavior in the last six months based on the eight symptoms of ODD from the DSM-IV-TR, 35 rating “never or rarely”, “sometimes”, “often”, or “always” for each symptom. As specified in the scoring instructions, 34 indicating “often” or “always” is considered endorsing that particular symptom. This scale demonstrated strong reliability (α = 0.85).
The number of symptoms endorsed as “often” or “always” were used to create a continuous ODD symptom count. Students who endorsed four or more symptoms were categorized as meeting symptom count diagnostic criteria for ODD based on the DSM-IV-TR. 35
CD symptoms and diagnosis
Additionally, the CSS 34 was utilized to assess for CD symptoms. This scale asked the students to indicate behaviors they engaged in between 5 and 18 years of age based on the 15 symptoms from the DSM-IV-TR, 35 answering either “yes” or “no”. Indicating “yes” is considered endorsing that particular symptom. 34 This scale demonstrated adequate reliability (α = 0.72).
The continuous CD variable was derived by calculating the total number of symptoms endorsed as “yes”. Students who endorsed three or more symptoms were categorized as meeting symptom count diagnostic criteria for CD based on the DSM-IV-TR. 35
Depression symptoms
The Center for Epidemiologic Studies Depression Scale - Revised 36 (CESD-R) is an updated version of the Center for Epidemiological Studies Depression Scale (CES-D) 37 and was used to assess current symptoms of depression. The CESD-R closely reflects DSM-IV-TR criteria for depression. The scale includes 20 symptoms with participants indicating “not at all or less than one day last week” (0); “one or two days last week” (1); “three or four days last week” (2); “five to seven days last week” (3); or “nearly every day for two weeks” (4). Scores for each question are added to compute a total depression score, and a score of 16 or higher was considered clinically significant. 36 Eaton et al. 36 found that preliminary validation suggested good psychometric properties. In the current study, the scale demonstrated strong reliability (α = 0.94).
Marijuana use
Participants were asked, “In the past 12 months, how often did you use marijuana?” Participants could select one of the 11 response options: not at all; 1–3 times; 4–7 times; 8–11 times; once a month; 2–3 times a month; once a week; 2–3 times a week; 4–6 times a week; once a day; twice a day; or several times a day.
Analytic plan
Prior to data analysis for study hypotheses, a preliminary analysis was completed to examine normality. Histograms of all continuous study variables (ie, current ADHD symptoms, past ADHD symptoms, CD symptoms, ODD symptoms, and total depression score) were run in order to complete a visual check for normality. 38 No further testing was done after the initial visual checks given that the sample size was large and, therefore, normality testing is more likely to be significant. 38 Pearson product-moment correlation coefficients were calculated to determine the strength of associations among study variables. Mediation analyses were conducted using PROCESS 39 for SPSS to test hypotheses of the current study.
Results
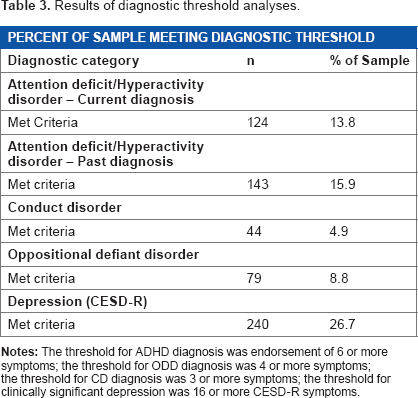
Participants reported an average of 3.42 current symptoms of ADHD, 3.44 past symptoms of ADHD, 0.55 symptoms of CD, 0.94 symptoms of ODD, and an average score of 12.4 on the CESD-R (Table 2). Results indicated that 13.8% of the sample met criteria for current ADHD, 15.9% met criteria for past ADHD, 4.9% met criteria for CD, and 8.8% of the sample met criteria for ODD. More than one quarter of participants (26.7%) met criteria for clinically significant depression based on CESD-R scores. The percentages of participants meeting threshold criteria for each diagnosis are presented in Table 3. Regarding marijuana use, 39.8% of participants reported use in the past year.
Results of symptom endorsement across diagnostic categories.

Results of diagnostic threshold analyses.
Results indicated significant correlations between current ADHD symptoms and continuous depression symptoms, as well as between past ADHD symptoms and continuous depression symptoms. Correlations between both current and past ADHD diagnoses and total depression symptoms were also significant. Similarly, correlations between both CD and ODD symptoms and diagnoses and total depression symptoms were significant.
Regarding past-year marijuana use, both current ADHD variables (eg, diagnosis and symptom count) were significantly correlated with marijuana use. However, past ADHD symptoms were significantly correlated with marijuana use while past diagnosis was not. CD symptoms and diagnosis both significantly correlated with marijuana use, but only ODD symptoms significantly correlated with marijuana use. Although both past ADHD diagnosis and ODD diagnosis were not significantly correlated with marijuana use, these variables were retained in the mediation analyses. Previous research has found that mediation may exist even when the relation between the predictor and outcome variables is nonsignificant. 40 Results of all bivariate correlations are presented in Table 4.
Results of all bivariate correlations.

P < 0.05
P < 0.01. The threshold for ADHD diagnosis was endorsement of 6 or more symptoms; the threshold for ODD diagnosis was 4 or more symptoms; the threshold for CD diagnosis was 3 or more symptoms; the threshold for clinically significant depression was 16 or more CESD-R symptoms.
Results indicated that depressive symptoms significantly mediated the pathway from both past ADHD symptoms and past ADHD diagnosis and marijuana use (Figs. 1 and 2). Depressive symptoms as indicated by CESD-R scores did not mediate the relation between current ADHD symptoms and marijuana use, nor did depressive symptoms mediate the relation between current ADHD diagnosis and marijuana use. Thus, it appears that depression impacts the relation between past, but not current, experience of ADHD to marijuana use.

Significant mediation results for past ADHD symptoms
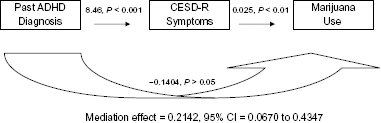
Significant mediation results for past ADHD diagnosis.
Results for hypothesis 2 showed that there was a significant indirect effect of depressive symptoms on the relation between both CD symptoms and CD diagnosis and marijuana use. Depressive symptoms do mediate the relation between CD and marijuana use, for both symptoms (full mediation) and diagnosis (partial mediation) of this DBD. The coefficients and P-values for both models are presented in Figures 3 and 4, respectively. Regarding hypothesis 3, statistical analyses found that depressive symptoms do mediate the relation between ODD diagnosis and marijuana use, but not the relation between ODD symptoms and marijuana use (Fig. 5).

Significant mediation results for CD symptoms.

Significant mediation results for CD diagnosis.

Significant mediation results for ODD diagnosis.
Discussion
Results suggest that depressive symptoms do, to some degree, mediate the relation between DBDs and marijuana use. Specifically, findings indicate that depressive symptoms mediate the relation between the following indicators and marijuana use: past ADHD symptoms, past ADHD diagnosis, CD symptoms, CD diagnosis, and ODD diagnosis. While the existing literature base has focused more on singular relations (eg, marijuana use and DBDs12,41; DBDs and depression 16 ; depression and marijuana use), 22 the current findings extend this literature by documenting a significant indirect pathway through depression on the relation between ADHD, CD, and ODD and marijuana use.
Interestingly, depression symptoms mediated the relation between past ADHD symptoms and diagnosis and marijuana use, but not between current ADHD symptoms or diagnosis and marijuana use. It may be the case that, for some participants, endorsement of current ADHD symptoms are actually reflective of other issues (eg, poor sleep) and less reflective of a true symptom of ADHD. Given that research has indicated that symptoms of childhood ADHD persist into adulthood for the majority of children with symptoms,42,43 young adults may have learned to cope with ADHD symptoms, but are adjusting to challenges associated with the college environment.
Results of hypothesis 2 indicated that depressive symptoms fully mediated the relation between CD symptoms and marijuana use, but partially mediated the relation between CD diagnosis and marijuana use. This finding may be because the diagnosis variable only captured individuals who met threshold criteria for CD; thus, it represents a more stringent cut-off than the continuous symptom count. Nevertheless, this is an interesting finding, and future research should investigate whether similar patterns emerge when testing these relations.
Findings for hypothesis 3 indicated that depressive symptoms mediated the relation between ODD diagnosis and marijuana use, but not ODD symptoms and marijuana use. Given the findings for CD, it is clear that the method in which disorders are conceptualized (eg, threshold diagnosis versus symptom count) impacts results. Future research should continue to investigate this pattern to determine if similar findings emerge across samples for both continuous and categorical diagnostic predictors.
Results may be interpreted through the lens of the self-medication hypothesis. 18 The presence of DBDs may lead to impairment, as is evidenced by the relation between DBDs and depression.15–21 Distress related to experiencing subthreshold or threshold symptoms of both DBDs and depression may lead individuals to look for alternative coping strategies. Consistent with the self-medication hypothesis, marijuana may be used to cope with distress related to DBDs, depression, or both.
Given that findings suggest that depression mediates the relation between DBDs and marijuana use, it would be helpful for practitioners to screen for symptoms of depression when working with someone exhibiting symptoms of ADHD, CD, or ODD. It may be the case that disruptive behavior is given priority in treatment because, as it is externalizing, it may lead to more tangible problems (eg, academic trouble, fights, antisocial behavior). 11 However, depressive symptoms –especially if they are subthreshold – may not be so readily noticed in an assessment of a client presenting with DBD symptoms. Clinicians should not only assess for these symptoms but should also screen for and, when applicable, monitor marijuana use among clients with DBD symptoms. Being able to successfully identify individuals who exhibit symptoms consistent with DBDs and also use marijuana could be an important target for prevention, such that basic coping skills such as relaxation techniques could instead be taught to be used in place of marijuana use. Adoption of healthy coping techniques among individuals with DBDs could have important implications for an overall reduction in marijuana use among this population, which may also lead to a decrease in depressive symptoms among individuals with DBDs, given that marijuana use has been shown to be related to depressive symptoms and suicide attempts.23,24
In conceptualizing each DBD, the present study examined both symptom count and diagnosis, so as to capture DBDs as both continuous and dichotomous variables. While the DSM identifies threshold criteria that are necessary to establish diagnosis of a given disorder 11 and clinical settings typically follow this as standard procedure, research has often utilized continuous symptom counts in conjunction with or as a stand-alone indicator of symptom severity. For example, previous research with college student samples has used the CSS to establish continuous symptom counts.44,45 Furthermore, researchers have criticized the DSM for relying on superficial symptom clusters to denote threshold criteria. 46 Thus, the dual conceptualization of DBDs is a unique strength of the present approach. Many studies in the extant literature take a solely dichotomous approach and investigate diagnosis of a DBD as a single variable. This approach likely misses individuals who do not meet threshold criteria for a DBD, yet still experience impairment from symptoms. Furthermore, from a statistical standpoint, transforming continuous data into categories (eg, meets vs does not meet threshold criteria) reduces their informative value and impacts statistical power. 47 Fedorov et al. 48 demonstrated that categorizing treatment outcome into two categories of equal size results in a loss of power of approximately 36%. The authors concluded that a sample size 1.571 times larger would be required to compensate for such a loss of power. 48
Prevalence findings for diagnostic threshold criteria in the current study are similar to previously documented prevalence rates among adults. Lifetime prevalence of ADHD diagnosis is 7.1%, 49 which is lower than the current prevalence rate for ADHD found in the current study (13.8%). It may be the case that ADHD symptoms were especially salient for students in the current sample, because the inherent academic aspect of college may foster increased awareness of impairment related to academic difficulties. However, research reviewing school-aged estimates of ADHD prevalence has documented rates ranging from 9.5% to 16.1%. 43 Given that 15.9% of the current study sample endorsed past diagnosis of ADHD, current study findings regarding past ADHD diagnosis are within the range of estimates documented in previous research.
The lifetime prevalence of ODD is estimated to be 10.2%, 50 and the current study documented a prevalence of 8.8%. The overall estimated lifetime prevalence of CD is 9.5% in the United States, 51 while the estimated percentage for females alone is 7.1%. 51 While the present study included a predominately female sample, we found a CD prevalence rate of 4.9%. The greater prevalence of ADHD, ODD, and CD among males11,49–51 may explain the lower rates of threshold criteria for DBDs in the current sample.
The current study had several limitations. A significant limitation is the self-reported nature of symptoms. Although the current study was offered exclusively in an online format and was able to achieve a large sample size, several alternative formats may be preferable for establishing symptoms and diagnostic threshold criteria for study variables. For example, future research could require that participants come in person and receive a standardized screening by a qualified professional in order to establish symptom counts and threshold criteria. Additionally, an objective measurement of behavior across settings may be helpful in establishing threshold criteria. However, among studies of college students and ADHD, for example, studies using self-reported data are very common; several self-reported studies of ADHD symptoms and related impairment are outlined in the work by Weyandt and DuPaul. 52 Furthermore, many studies have collected self-reported data from young adults and have found such data to be valid. For example, Internet-based research on drug and alcohol use among young adults has been found to yield valid and reliable estimates of use.53–55 Thus, the online format and self-reported nature of the present study may be viewed as strengths. Offering the study online increased convenience of participation and may have reduced bias in response to sensitive questions (eg, marijuana use, mental health symptoms) and was also more time efficient for both participants and researchers. Furthermore, both the convenience and small time commitment associated with the present study facilitated collecting data from a large sample size.
Another limitation of the present study was the use of a single question about marijuana use to establish frequency of past-year use. Because a sole question was asked about the entire past year, it was not possible to determine whether frequency of use was consistent for all respondents. Similarly, it was not possible to determine whether marijuana use resulted in impairment for the participant. Future studies should consider using a longer, validated measure to establish marijuana frequency over time, as well as any resultant impairment.
Furthermore, because the sample was drawn from college students at a large Southeastern University, it may not be generalizable to students at all universities or to individuals outside of the sampled age range. Also, the study included more females than males, so findings may not be the same in a predominately male sample. Future research should aim to collect data from a more representative sample and should also analyze results by gender, given gender differences in diagnosis of DBDs. 11 Finally, because the present study was cross sectional, it is not possible to establish causality or clearly elucidate the hypothesized developmental pathway. Future research should conduct longitudinal studies to better understand the relations among DBDs, depression, and marijuana use from childhood to early adulthood.
Author Contributions
Conceived and designed the experiments: KB, KF. Analyzed the data: MCM. Wrote the first draft of the manuscript: MCM. Contributed to the writing of the manuscript: KF, KB. Agreed with manuscript results and conclusions: MCM, KB, KF. Jointly developed the structure and arguments for the paper: MCM, KF. Made critical revisions and approved the final version: MCM, KB, KF. All the authors reviewed and approved the final manuscript.