
Abstract
Background:
Individuals with chronic conditions often use opioids for pain and the broadening legalization of marijuana and its potential analgesic effects may prompt some individuals to use marijuana as an additional option. Both substances have been individually linked to adverse effects on major depressive disorder (MDD), but little is known about their co-use. This study examined the association between co-use and MDD among US adults with chronic conditions.
Methods:
This cross-sectional analysis used 2022 National Survey of Drug Use and Health data from 35 585 adults older than 18 years with chronic conditions. Participants were categorized into 4 groups: (1) co-use of marijuana and opioids, (2) opioid only, (3) marijuana only, and (4) neither in the past year. MDD was defined using DSM-5 criteria (⩾2 weeks of depressed mood or anhedonia with ⩾5 symptoms). Associations between substance use and MDD were assessed with Rao-Scott chi-square tests and multivariable logistic regression, adjusting for demographic, behavioral, clinical, and social determinants of health as well as COVID-19-related mental health and past-year benzodiazepine use.
Results:
Overall, 8.5% reported co-use; 26.1% reported opioid use and no marijuana use; and 10.9% reported marijuana use and no opioid use. Past year MDD was highest among those with co-use (20.8%) followed by marijuana only (18.4%); opioid only (9.3%); and neither (5.6%). In fully adjusted logistic regression, co-use had the strongest association with past year MDD (AOR = 1.92, 95% CI = 1.45, 2.50) followed by marijuana only (AOR = 1.72, 95% CI = 1.31, 2.26) and opioid only (AOR = 1.44, 95% CI = 1.14, 1.82) compared to the neither opioids nor marijuana group.
Conclusion:
Co-use of opioids and marijuana is not uncommon among adults with chronic conditions and is associated with higher odds of MDD. These findings underscore the importance of monitoring substance use in people with chronic conditions, especially to detect co-use that may worsen mental health.
Keywords
Introduction
Existing research demonstrates that chronic pain frequently co-occurs with chronic physical illnesses, with prevalence rates ranging from 26% to nearly 50%, depending on the condition. 1 For example, pain affects approximately 46% of adults with diabetes, 41% with heart disease, 33% with asthma, and almost half of those with chronic obstructive pulmonary disease (COPD). 1 Managing pain in chronic conditions involves the use of analgesics medications. When conventional treatments such as nonsteroidal anti-inflammatory drugs (NSAIDs), topical agents, or corticosteroids do not provide adequate relief, opioids are often prescribed as part of a pain management plan. For example, in 2019, 22.1% of U.S. adults with chronic pain reported using prescription opioids within 3 months. 2
However, the long-term benefits of opioids for chronic pain management are limited, and national prescribing guidelines have shifted to reflect growing safety concerns. 3 Therefore, in recent years, marijuana has also emerged as an alternative or adjunctive therapy for pain management. 4 In 2022, 31% of adults reported using marijuana to manage their pain. 5 However, evidence regarding marijuana’s effectiveness is mixed: a large prospective study found no significant pain-relieving benefit, 6 whereas a systematic review of 15 randomized clinical trials reported modest benefits for certain chronic conditions. 7
Despite mixed evidence, national efforts to curb opioid prescribing may have accelerated the use of marijuana as a substitute or companion therapy.8,9 In the US, states that have legalized marijuana use report lower opioid prescribing rates, suggesting that marijuana may partially replace opioids for pain management.10,11 Some adults report using marijuana to reduce opioid consumption,12-14 enhance analgesic effects when combined with low-dose opioids, 15 or achieve better overall pain control.16,17
As a result, co-use of opioids and marijuana may be increasingly common. For example, among U.S. veterans prescribed opioids, 9.7% reported marijuana co-use in 2018, 18 and among individuals with chronic pain treated with opioids, 8.6% reported co-use. 19 Among pregnant women treated for opioid use disorder, co-use prevalence ranged from 24% 20 to 45%. 21 Given these patterns of co-use, it is critical to consider the broader mental health implications of opioid and marijuana use. Separate lines of research have shown a strong link between opioid use and depression, 22 potentially mediated by emotion dysregulation 23 or genetic vulnerability. 24 Likewise, marijuana use has been associated with an increased risk of depressive disorders.25,26 For example, a systematic review of 14 longitudinal studies concluded that frequent and heavy consumption of marijuana could lead to increased risk of incident depressive disorders, 25 potentially due to structural and functional changes in emotion-regulating brain regions such as the amygdala and prefrontal cortex. 27 It is plausible that co-use of substances may compound this risk. For example, in comparison to those who used only opioids, individuals who co-used opioids and cannabis exhibited heightened anxiety and depression symptoms. 28 In a study of participants from 2 large pain centers in Israel, those with co-use had higher adjusted odds of depression (aOR = 3.34, 95% CI = 1.52, 7.34) compared to those with only marijuana use. 19
Adults with chronic physical conditions represent an important population in which to understand these patterns, given their higher likelihood of experiencing pain and using multiple substances for pain relief. However, research on the association of co-use with depression, among adults with chronic conditions in the US remains limited, highlighting the need for further investigation in this area. Therefore, the aim of this study is to investigate the association between the co-use of opioids and marijuana and MDD among adults with chronic conditions in the US. Based on existing evidence linking substance co-use to adverse mental health outcomes, we hypothesized that individuals reporting co-use would have higher odds of MDD compared to those reporting no use.
Methods
Study Design
We used a cross-sectional study design. The data source was the 2022 National Survey of Drug Use and Health (NSDUH, 2022). NSDUH is an annual survey for the collection of self-reported data on tobacco, alcohol and drug use, and health status. NSDUH has a nationally representative sample of non-institutionalized individuals in the US. Their 2022 weighted sample covered approximately 224 million adults representing the US non-institutionalized population. We focused on individuals aged 18 or older (n = 15 527) with chronic conditions. In NSDUH the respondents were provided with a list of chronic conditions and were asked “Below is a list of health conditions that you may have had during your lifetime. Please read the list and type in the numbers of all of the conditions that a doctor or other health care professional has ever told you that you had.” The following conditions were listed: asthma, cancer, kidney disease, cirrhosis of the liver, chronic obstructive pulmonary disease, diabetes, heart disease, hypertension, hepatitis B or C, and HIV or AIDS. Adults who have never had any of these conditions were classified as a “No chronic condition” group. Thus, our analytical sample consisted of adults aged 18 or older only with the chronic conditions listed above.
Measures
Dependent Variable: Major Depressive Disorder (Yes/No)
NSDUH defined MDD based on Diagnostic and Statistical Manual of Mental Disorders (DSM-5) criteria.29,30 Based on DSM-5 criteria, those who felt depressed or lost interest or pleasure in daily activities for ⩾2 weeks in the past year and those experiencing ⩾5 of 9 symptoms during the same 2-week period were classified as MDD.
Key Independent Variable: Marijuana and Opioid Use Categories
Opioid use in the NSDUH was identified if the participant used opioids as a prescription medication (as directed by a doctor) or used in any way not directed by a doctor in terms of amount, duration, other during the previous year (yes, no). Separation of prescription use, and opioid use not directed by a doctor was not available in the NSDUH, 2022. Participants were also asked if they had any marijuana product use during the past 12 months (yes, no). We combined opioid and marijuana use to create the following 4 mutually exclusive groups of past year use: (1) co-use of opioids and marijuana; (2) opioid only; (3) marijuana only; and (4) no use of opioids/marijuana. Our marijuana measure reflects any past-year use regardless of purpose or source.
Other Independent Variables
As MDD is affected by many factors, we also included other explanatory variables such as age, sex, race and ethnicity education, poverty status, marital status, and insurance coverage. We also included health-related variables (multimorbidity) and lifestyle factors such as smoking, alcohol use, and obesity (body mass index). As COVID-19 has been shown to affect mental health, 31 NSDUH has a question on whether COVID-19 negatively affected mental health (not at all, a little or some, quite a bit or lot). Because the COVID-19 pandemic had a profound and lasting impact on mental health, we included this NSDUH variable on self-reported COVID-19-related mental health effects as a covariate. Multiple studies have documented that COVID-19-related stress, isolation, and socioeconomic disruptions substantially increased the prevalence and severity of depressive and anxiety symptoms in the general population, particularly among adults with chronic conditions who were already vulnerable to psychological distress.32-34 Including this variable allowed us to account for pandemic-related mental health changes that might confound the relationship between opioid and marijuana use and major depressive disorder. We included benzodiazepine as it is used to treat MDD. 35 As MDD is affected by many factors, we also included other explanatory variables such as demographics (age, sex, race, and ethnicity), social determinants of health (SDOH) including education, poverty status, marital status, and insurance coverage and lifestyle factors (smoking, alcohol use, and obesity). Moreover, we included multimorbidity, defined as having 2 or more chronic conditions. Detailed chronic conditions percentages for our study sample are provided in the Appendix.
Statistical Analyses
Rao-Scott Chi-square tests that accounted for clustering, stratification and weights were used to analyze the unadjusted association of opioid and marijuana use categories with MDD. Nested multivariable logistic regressions were used to adjust for other explanatory variables that may be associated with MDD. We built 4 nested models. The first model included only opioid and marijuana use categories; model 2 additionally included sex, age, and race and ethnicity. Model 3 furthermore included SDOH. The fully adjusted logistic regression model (Model 4) incorporated age, sex, race, and ethnicity, SDOH, benzodiazepine use, multimorbidity, body mass index, smoking and alcohol use and negative mental health effects due to COVID-19. All analyses were conducted in SAS 9.4 using survey procedures (SAS Institute, Cary, NC).
Results
In this study of adults with chronic conditions, 52.2% were female, 66.7% were non-Hispanic White, and 12.2% were non-Hispanic Black. 37.2% had multimorbidity, defined as the concurrent presence of 2 or more chronic conditions (Table 1). There were 8.5% reporting co-use of opioids and marijuana; 26.1% reported opioid use only; 10.9% reported marijuana use only; and over half (54.5%) reported no opioid or marijuana use within the past year.
Description of Selected Characteristics Among Adults (⩾18 years) with Chronic Conditions National Survey Drug Use and Health (NSDUH), 2022.
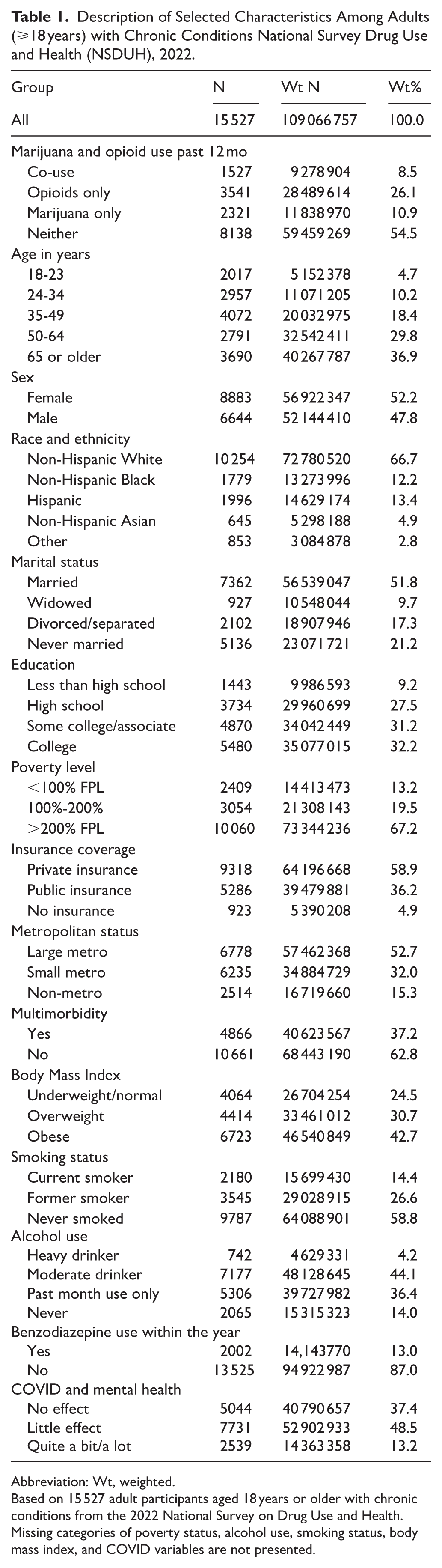
Abbreviation: Wt, weighted.
Based on 15 527 adult participants aged 18 years or older with chronic conditions from the 2022 National Survey on Drug Use and Health. Missing categories of poverty status, alcohol use, smoking status, body mass index, and COVID variables are not presented.
Table 2 provides the frequencies and weighted percentages of opioid and marijuana use categories by individual characteristics. Females had a higher prevalence of opioid-only use compared to males (28.9% vs 23.1%; P < .001). Males had a higher prevalence of marijuana-only use compared to females (12.4% vs 9.4%; P < .001). Considering age, the highest prevalence of co-use of opioids and marijuana was among adults aged 25 to 34 years (15.0%), whereas adults aged ⩾ 65 years had the lowest prevalence (3.7%; P < .001). In terms of race/ethnicity, non-Hispanic White and non-Hispanic Black individuals had the highest opioid-only use (27.5%), while Asians had the lowest (19.3%; P < .001). Rates of co-use of opioids and marijuana were similar among non-Hispanic Black (8.1%) and non-Hispanic White individuals (8.8%), and lower among Hispanics (7.5%) and Asians (2.5%).
Description of Selected Characteristics by Marijuana & Opioid Use Among Adults (>18 years) with Chronic Conditions National Survey of Drug Use and Health, 2022.

Abbreviation: Wt, weighted.
Based on 15 527 adult participants aged 18 years or older with chronic conditions from the 2022 National Survey on Drug Use and Health. Missing categories of poverty status, alcohol use, smoking, and body mass index are not presented. Group differences in marijuana and opioid use categories in the past 12 months were tested with Rao-Scott chi square statistics.
Table 3 presents the sample characteristics by whether the individual had MDD. Overall, 9.3% of individuals with chronic conditions had MDD. MDD prevalence differed significantly (P < .001) across opioid and marijuana use categories. Specifically, individuals with co-use of opioids and marijuana had the highest prevalence of MDD (20.8%), followed by individuals with marijuana use only (18.4%), opioid use only (9.3%), and neither substance use (5.6%). MDD prevalence was also significantly associated with demographic and social determinants of health factors. For example, MDD prevalence was significantly higher among women (11.2%) than men (7.1%) and was lower among non-Hispanic Black individuals (7.6%) compared to non-Hispanic White individuals (9.4%).
Description of Selected Characteristics by Major Depressive Disorder Among Adults (>18 years) with Chronic Conditions, National Survey of Drug Use and Health (NSDUH), 2022.
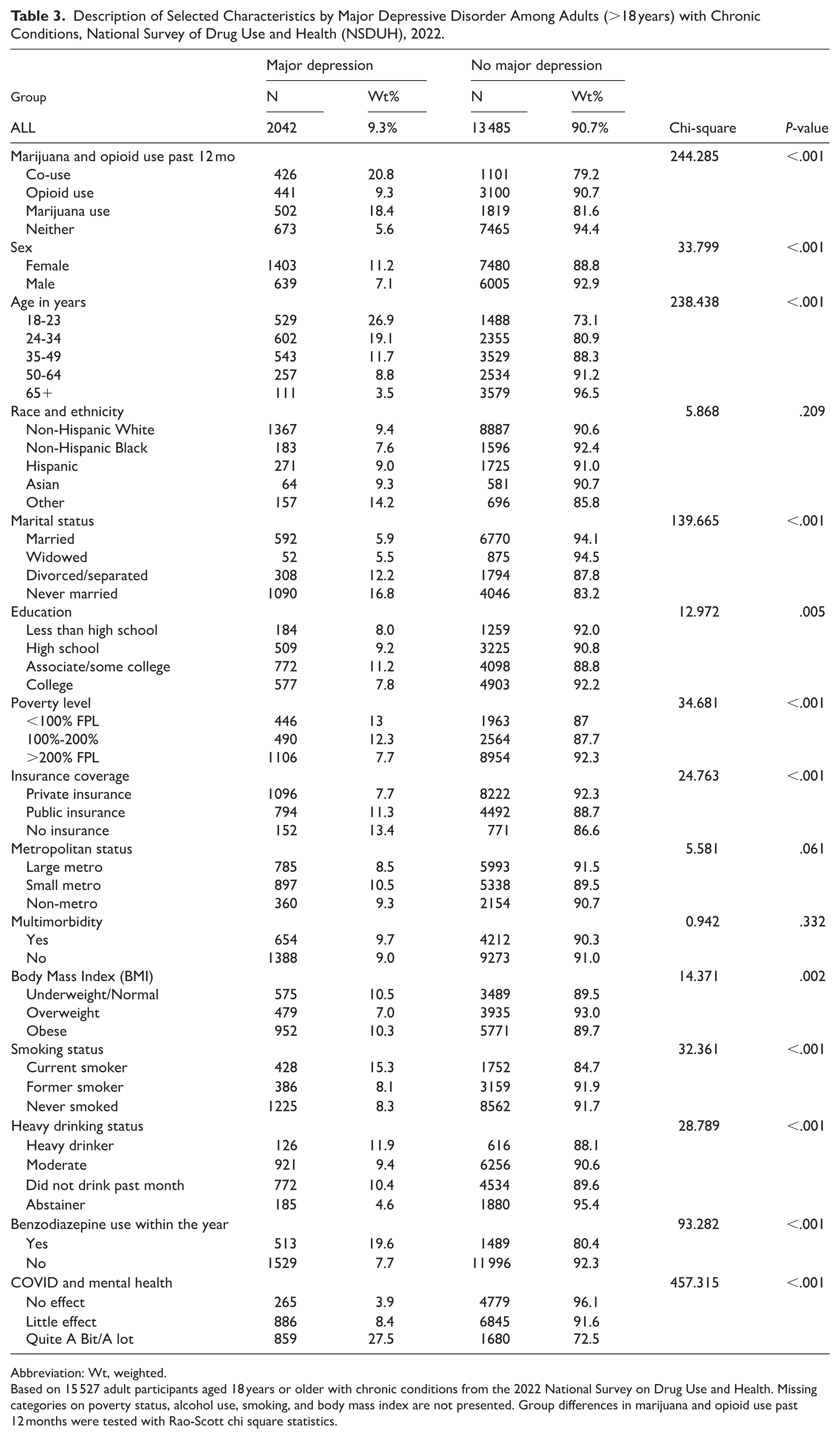
Abbreviation: Wt, weighted.
Based on 15 527 adult participants aged 18 years or older with chronic conditions from the 2022 National Survey on Drug Use and Health. Missing categories on poverty status, alcohol use, smoking, and body mass index are not presented. Group differences in marijuana and opioid use past 12 months were tested with Rao-Scott chi square statistics.
Table 4 presents the results of the multivariable logistic regression analyses examining the association between past-year marijuana and opioid use and MDD. In the unadjusted model (Model 1), individuals who reported co-use of marijuana and opioids in the past 12 months were over 4 times as likely to meet criteria for MDD compared to those who used neither substance (UOR = 4.42; 95% CI: 3.45-5.66). Meanwhile, those who used opioids only (UOR = 1.74; 95% CI: 1.42-2.13) and those who used marijuana only (UOR = 3.81; 95% CI: 3.00-4.84) also had significantly higher odds of MDD compared to non-users.
Unadjusted and Adjusted Odds Ratios (AOR) and 95% CI of Opioid and Marijuana Use Categories From Logistic Regression on Major Depressive Disorder, Adults (>23 years) with Chronic Conditions National Survey of Drug Use and Health (NSDUH), 2022.

Based on 15 527 adult participants aged 18 or older, with chronic conditions from the 2022 National Survey on Drug Use and Health. Missing indicators for poverty status, heavy drinking, heavy smoking and body mass index categories were included in the regression analyses.
After sequentially adjusting for demographic, socioeconomic, and health status (Models 2 and 3), the odds ratios decreased but remained above 1 (P < .001), indicating higher adjusted odds of MDD among all 3 user groups compared to adults who did not use either marijuana or opioids. In the fully adjusted model (Model 4), which controlled for additional covariates such as COVID-related mental health concerns, multimorbidity, and benzodiazepine use, co-use remained significantly associated with MDD (AOR = 1.91; 95% CI: 1.45-2.50), indicating 91% higher odds compared to individuals who used neither marijuana nor opioids. Those who used opioids only (AOR = 1.44; 95% CI: 1.14-1.82) and marijuana only (AOR = 1.72; 95% CI: 1.31-2.26) continued to have significantly higher adjusted odds of MDD as well.
Discussion
This nation-wide study set out to examine the association of co-use of marijuana and opioids with MDD among US adults with chronic conditions. Our study found that 8.5% of adults 18 years or older with chronic conditions reported co-use of marijuana and opioids Previous studies have reported a broad range of co-use rates, from as low as 1% in some populations with persistent pain to as high as 45% in certain subgroups (eg, pregnant women), highlighting the influence of demographic and health status on these patterns. Although pain was not directly measured in the NSDUH, both opioids and marijuana are commonly used to manage pain, and individuals with chronic conditions are particularly likely to use these substances for analgesic purposes.12,36-41 Accordingly, our focus on adults with chronic conditions, who are more likely to experience pain, provides an important context in which to understand the potential overlap between pain management behaviors and mental health outcomes.
Our main findings on the association of co-use with MDD consistently demonstrated the largest odds ratios, suggesting that concurrent use of marijuana and opioids carries a distinct, stronger association with MDD than using either substance alone. However, our study focused on adults with chronic conditions and to-date, this is the first study on the association between combined use of marijuana and opioids and MDD among persons with chronic conditions. Substantially greater odds of MDD among those with co-use than the use of either substance alone, suggests a potential synergistic interaction. In a survey of U.S. college students, Lui et al 42 found that polysubstance users, defined as those reporting use of 2 or more psychoactive substances, had significantly higher odds of both depression and anxiety compared with single-substance users. Similarly, MacDonald et al 43 examined clients dependent on alcohol, cocaine, or both, and reported that individuals with concurrent alcohol–cocaine dependence scored significantly higher on validated anxiety and depression symptom scales than those dependent solely on cocaine. Taken together, these studies provide convergent evidence that the combined use of multiple substances confers a greater risk for depression than use of any 1 drug in isolation, a potential interactive effect.
Our study also found that use of marijuana and opioids may differentially affect MDD in adults with chronic conditions. Individuals who reported using marijuana use alone or opioids alone had significantly higher odds of MDD compared to non-users, the adjusted odds of marijuana use with MDD was higher. Although the relationship of marijuana and opioids with MDD are complex, individuals who use marijuana may be more susceptible to MDD because marijuana can impact various brain regions involved in mood, cognition, and pain. 44 This can lead to a complex interplay of effects, including potential for MDD. However, when we compared the odds of MDD among individuals who use marijuana alone (aOR = 1.18, 95% CI = 0.93, 1.49) with opioid use alone, they were not significantly different, a finding that diverges from a study in Israel, 19 which reported a stronger association of opioid use with depression.
Our findings suggest that addressing co-user patterns may require approaches that go beyond traditional models treating substance use or depression in isolation. There is an urgent need to closely monitor, and screen mental health and substance use among US adults with chronic conditions in mental health as well as in primary care settings. Primary care professionals should be trained to assess poly-substance use patterns, particularly in patients with depressive symptoms, and to tailor treatment strategies accordingly. This monitoring is increasingly important given that more states are relaxing regulations on marijuana, leading to increased marijuana access. Similarly, traditional mental health treatment models that address substance use in isolation may be insufficient for co-users. Co-users may benefit more from holistic programs that integrate psychotherapeutic solution-focused approaches and with addiction-focused strategies such as evidence-based recovery, medication-assisted treatment, residential treatment, motivational interviewing, and cognitive behavioral therapy. Research supports integrated treatment models for comorbid substance use and depressive disorders as more effective than parallel or sequential approaches.45,46 Although not the focus of the study, our findings revealed that sociodemographic characteristics, health factors, and COVID-19-related variables can influence both substance-use patterns and the risk of MDD among adults with chronic conditions. For example, differences by age, sex, race and ethnicity may reflect variation in substance use patterns and structural inequities, such as unequal exposure to stress, differences in pain treatment and prescribing, and uneven access to supportive services, that can influence both substance use and mental health.18,47 Likewise, socioeconomic characteristics (eg, education, income, and insurance coverage) can also affect access to nonpharmacologic pain management, specialty mental health services, and continuity of care. These factors may decrease reliance on substances while also reducing untreated depressive symptoms.48,49 Health-related factors, including the number and type of chronic conditions and self-rated health, may further increase vulnerability to both co-use and MDD through greater symptom burden, functional limitation, sleep problems, and stress associated with living with chronic illness. 50
In our study those with multimorbidity had notably higher prevalence of both co-use and opioid-only use compared with those without multimorbidity. This pattern is consistent with prior literature indicating that individuals with multiple chronic conditions often experience more persistent or severe pain, leading to increased reliance on pharmacologic pain management approaches.39,51,52 The elevated rates of co-use and opioid-only use among adults with multimorbidity in our study underscore the possibility that greater chronic disease burden may contribute to more complex substance-use patterns and, consequently, at higher risk of adverse mental health outcomes such as MDD. These findings highlight the importance of integrated care approaches that substance use, multimorbidity, and mental health simultaneously.
Finally, the COVID-19 period added an extra layer of strain. Disruptions in healthcare, increased isolation, financial instability, and pandemic-related distress may have shifted substance-use behaviors and contributed to a higher risk of depressive episodes.53,54 Overall, these findings suggest that co-use and MDD do not occur in isolation and can be affected by patients’ social and health circumstances. Therefore, effective screening and intervention strategies should be implemented.
Strengths and Limitations
This study has several strengths. MDD, opioid use, and marijuana use were available from a large, long-established, U.S. national study with validated questions. The large sample size permitted the inclusion of many covariates that could be influential in the relationship of MDD and opioid and/or marijuana use. Importantly, our models adjusted for the self-perceived mental health impact of COVID-19, which has been identified as a major population-level stressor contributing to depressive symptoms worldwide. Adjusting for this factor minimized potential confounding from pandemic-related distress that might otherwise bias the associations between opioid and marijuana use and MDD. Nevertheless, the data set for this study did place some limitations upon our analyses. We were not able to distinguish between opioid use by prescription and not directed by a doctor. Further, the NSDUH does not capture detailed information on non-prescribed opioid use, such as opioids obtained outside of medical settings (eg, obtaining street drugs). Data were not available concerning marijuana use by prescription, or self-use in states where allowed. Co-use may not represent use of both substances simultaneously. We also did not have data concerning whether the substances were being used for pain relief or for other purposes. Finally, this study identifies a correlation and not a causal relation from co-use to MDD: it is possible that MDD causes co-use or that some factors drive both co-use and MDD simultaneously. Because this study analyzed the full adult sample available in the 2022 National Survey of Drug Use and Health (NSDUH), a large nationally representative dataset, no a priori sample size calculation or power analysis was performed.
Conclusion
One in 12 US adults with chronic conditions (weighted n = 9.28 million) had co-use of marijuana and opioids. Co-use of marijuana and opioids carries a distinct, stronger association with MDD than using either substance alone. There is a need to closely monitor substance use, in particular co-use among US adults with chronic conditions, as early detecting may reduce adverse mental health outcomes.
Footnotes
Appendix
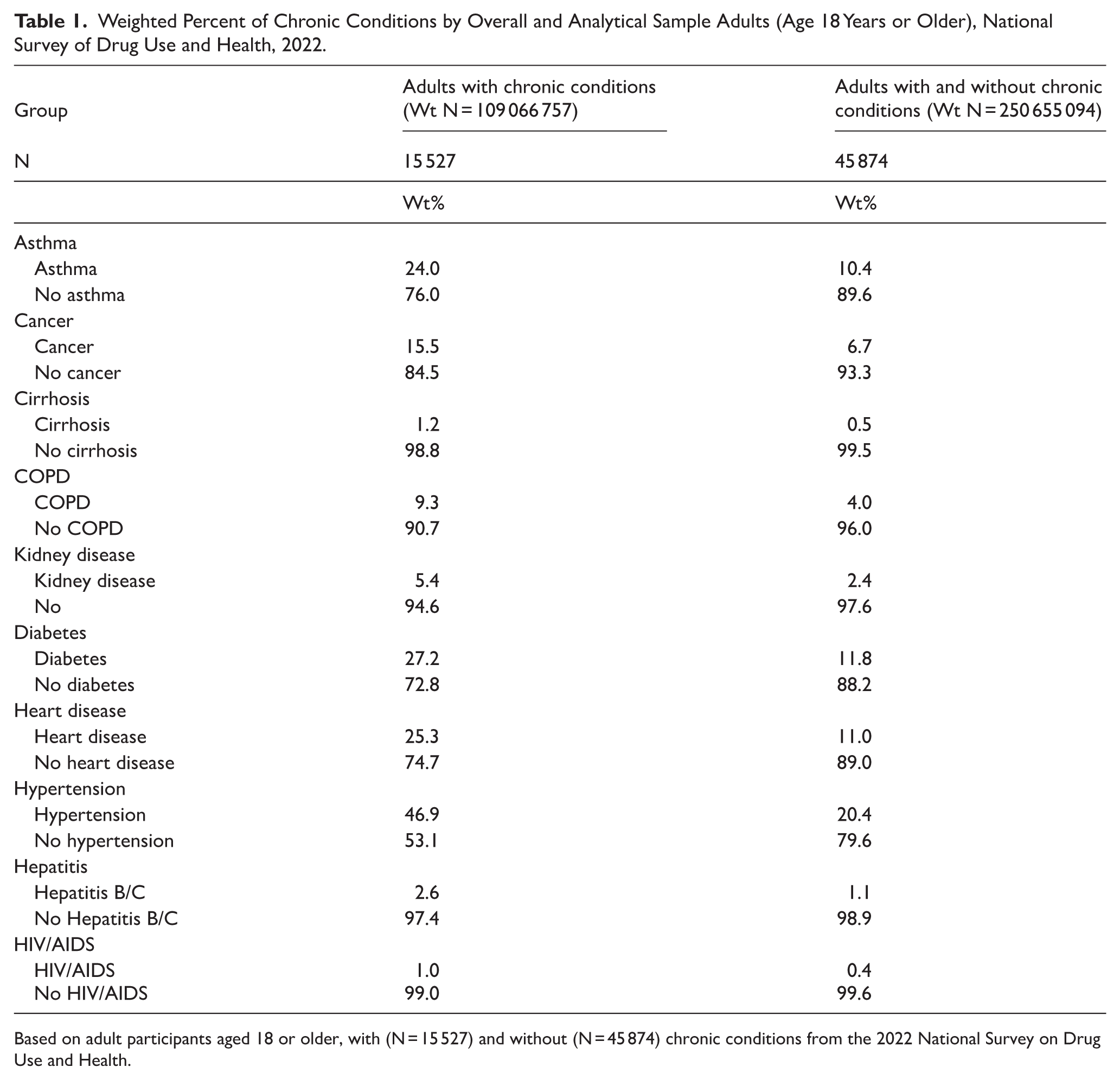
Weighted Percent of Chronic Conditions by Overall and Analytical Sample Adults (Age 18 Years or Older), National Survey of Drug Use and Health, 2022.
| Group | Adults with chronic conditions (Wt N = 109 066 757) | Adults with and without chronic conditions (Wt N = 250 655 094) |
|---|---|---|
| N | 15 527 | 45 874 |
| Wt% | Wt% | |
| Asthma | ||
| Asthma | 24.0 | 10.4 |
| No asthma | 76.0 | 89.6 |
| Cancer | ||
| Cancer | 15.5 | 6.7 |
| No cancer | 84.5 | 93.3 |
| Cirrhosis | ||
| Cirrhosis | 1.2 | 0.5 |
| No cirrhosis | 98.8 | 99.5 |
| COPD | ||
| COPD | 9.3 | 4.0 |
| No COPD | 90.7 | 96.0 |
| Kidney disease | ||
| Kidney disease | 5.4 | 2.4 |
| No | 94.6 | 97.6 |
| Diabetes | ||
| Diabetes | 27.2 | 11.8 |
| No diabetes | 72.8 | 88.2 |
| Heart disease | ||
| Heart disease | 25.3 | 11.0 |
| No heart disease | 74.7 | 89.0 |
| Hypertension | ||
| Hypertension | 46.9 | 20.4 |
| No hypertension | 53.1 | 79.6 |
| Hepatitis | ||
| Hepatitis B/C | 2.6 | 1.1 |
| No Hepatitis B/C | 97.4 | 98.9 |
| HIV/AIDS | ||
| HIV/AIDS | 1.0 | 0.4 |
| No HIV/AIDS | 99.0 | 99.6 |
Based on adult participants aged 18 or older, with (N = 15 527) and without (N = 45 874) chronic conditions from the 2022 National Survey on Drug Use and Health.
Ethical Considerations
This retrospective observational study was exempted by the Institutional Review Board as the data used is a de-identified publicly available database.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Author Contributions
All authors contributed to study design, interpretation of findings, manuscript drafting, and critical revision. Usha Sambamoorthi contributed to study design, data preparation, analysis, interpretation of results, manuscript drafting, critical revision, and supervision of the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was supported by the National Institute of General Medical Sciences, 5U54GM104942-08. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Not applicable.