
Abstract
Substance misuse is frequently encountered in the psychiatric emergency service (PES) and may take many forms, ranging from formal DSM-IV diagnoses to less obvious entities such as hazardous consumption. Detecting such patients using traditional screening instruments has proved problematic. We therefore undertook this study to more fully characterize substance misuse in the PES and to determine whether certain variables might help better screen these patients. We used a prospectively acquired database of over 18,000 visits made to four PESs during a 2-year period in the province of Quebec, Canada. One of the variables acquired was a subjective rating by the nursing staff as to whether substance misuse was a contributing factor to the visit (graded as direct, indirect, or not at all). Substance misuse accounted for 21% of all diagnoses and alcohol was the most frequent substance used. Patients were divided into those with primary (PSM), comorbid (CSM) or no substance misuse (NSM). Depressive disorders were the most frequent primary diagnoses in CSM, whereas personality and substance misuse disorders were frequent secondary diagnoses in PSM. Although many variables significantly differentiated the three groups, few were sufficiently detailed to be used as potential screening tools. Those situations that did have sufficient details included those with a previous history of substance misuse, substance misuse within 48 hours of the visit, and visits graded by the nursing staff as being directly and/or indirectly related to substance misuse. Variables related to substance misuse itself were the primary predictors of PSM and, less significantly, CSM. The nursing staff rating, although promising, was obtained in less than 30% of all visits, rendering its practical use difficult to assess.
Introduction
Patients presenting with primary or comorbid substance misuse are frequently encountered in the medical (ED) and in the psychiatric emergency service (PES).1–8 Discharge diagnoses for these patients typically include DSM-IV-TR-concordant syndromes such as dependence, withdrawal, and abuse. 9 Patients with these diagnostic profiles place a heavy burden on the PES as they have been associated with multiple visits, either to a single2,5,10 or several different services. 1
In addition, more subtle forms of substance misuse have been described. For instance, alcohol use disorders (AUDs) such as hazardous (a pattern that increases the risk of harmful consequences in the absence of an identifiable disorder) or harmful drinking (a pattern causing physical or mental consequences) can occur and have a significant public health impact. 11 In the general population, the majority of alcohol-related problems may be due to a hazardous or harmful type of consumption, rather than to alcohol dependence. 12 In a primary care setting, brief interventions for hazardous and harmful drinking have been shown to be of modest to moderate benefit in reducing alcohol consumption over time.13–15 Less is known about their effectiveness in a general, non-trauma ED or PES population, although several studies suggest that, even when including trauma-based patients, it is modest at best.16–18
Part of the difficulty in assessing the clinical relevance of treatment interventions in an emergency setting may be due the perceived complexity by non-research trained in-house staff of using the screening instruments designed to detect substance misuse in general, as well as the more subtle variants, such as AUD. 19 These include the AUDIT and AUDIT-C (10 and 3 questions, respectively), the CAGE, the Michigan Alcoholism Screening Test, the FAST alcohol-screening test among others.11,17, 20–25 Single question screening instruments have been developed in order to reduce this complexity and have shown some promise in detecting AUD as well as alcohol dependence in an emergency environment. 21 Another difficulty is that the socio demographic profile of the typical PES patient, skewed towards the more economically impoverished, may mimic that usually found in severe substance misuse and hinder its detection.3,26,27
Data was acquired in four PESs in the province of Quebec using a prospective, research-based database in order to answer to the following questions: 1) to better characterize substance misuse in the PES; 2) to determine whether particular sets of variables, some obtained pre triage and other at triage, might be associated with a substance misuse diagnosis; 3) to assess whether the nursing staff's opinion as to a possible relationship between substance misuse and a PES visit possesses sufficient sensitivity and specificity to be used as a triage tool; and 4) to assess whether visits judged by the nursing staff as related to substance misuse, but where the discharge diagnosis was not substance misuse, might fit the profile of at risk behaviors such as AUD.
Methods
This study was approved by the scientific subcommittees of the institutional review boards of three of four PES sites and was exempted from full review. At one of the four sites full institutional review board approval was required and obtained.
Data collection was as described in previous studies.28,29 Briefly, clinical and demographic data were prospectively obtained from patients 18 years of age and older visiting four PESs between September 1st, 2002 and August 31st, 2004. Two services were in the city of Montreal (Quebec, Canada). One was in an inner city university teaching hospital and the other in an urban university affiliated psychiatric institute near the downtown core. This latter PES did not possess prior medical triage and thus functioned similarly to a “walk-in clinic.” Each PES in metropolitan Montreal is assigned a geographic catchment area and citizens within it are obliged to seek acute psychiatric care at that service only. Approximately 4.8% of patients who underwent triage in the ED of the general hospital PES were referred for a psychiatric assessment. Of the two remaining sites, both were in general hospitals. One was in a university-affiliated teaching hospital in Quebec City (300 km east of Montreal, with approximately 500,000 citizens) and the other in a suburban/rural setting (Saint-Jean-sur-Richelieu, 40 km south of Montreal, with approximately 90,000 citizens). This latter site differed from the other three by not having an observation area with short-term beds.
As previously stated,28,29 a maximum of 72 variables per visit could be acquired. The main table contained administrative variables (chart number, name, sex, etc.). Linked tables contained variables pertinent to the consultation process, such as date and time of arrival, reasons for the referral, psychosocial stressors prior to the visit, referral source, ethnicity, employment, residential status, disposition, DSM-IV diagnoses (3 per visit) among others. Variables specific to substance misuse included a present or past history of substance misuse, the type of substance used (alcohol, cocaine…), substance misuse within 48 hours of the visit, and a present or past history of attending a detoxification center. Also included was a subjective rating by the nursing staff as to whether substance misuse was a contributing factor to the visit. This was graded as direct (patients appeared intoxicated and/or reeked of alcohol), indirect (patients were not overtly intoxicated although financial and/or social problems related to substance misuse precipitated the visit) or, not at all. All variables in the database were listed in a paper format, which was used as the primary triage instrument for patients visiting the four services during the 2-year period. The completed forms were forwarded to the principal investigator on a weekly basis for data entry.28,29
As in our earlier reports,28,29 many strategies were used in order to minimize diagnostic uncertainty. First, over 60% of visits have been shown to occur within the daytime hours at these sites, which were covered (during the weekdays) by regular psychiatric staff each with over 5 years’ experience in the PES setting. No site provided midnight to 7 AM assessments. Patients referred during this time period were kept in the PES (or the ED) for assessment in the morning. As such, up to 80% of patients were assessed by the regular PES staff during weekdays. Most staff obtained their medical and specialty training at one the four medical faculties in the province of Quebec and thus shared a common set of methodological/ethical/cultural standards. Second, diagnoses (made using DSM-IV guidelines during non-structured clinical interviews) were obtained either directly from staff after the patient assessment or from the patient's chart prior to it leaving the PES. Third, diagnoses were grouped into broad categories, which included ‘adjustment’, ‘anxiety’, ‘personality’, ‘affective’, ‘schizophrenia/ chronic psychotic disorders’, ‘substance misuse’ and an ‘other’ subcategory (comprised of organic metal, eating and impulse control disorders, and psychosis not otherwise specified). Fourth, between 65% to 80% of frequent users at all sites were at one point in time under multidisciplinary outpatient care and as such any diagnostic uncertainty could be clarified with the treating team.
Primary data analysis
Data was analyzed using Stata (Version 13). The dataset comprised 18,380 visits where a primary diagnosis could be ascertained. The general hospital site in Montreal accounted for 20% of all visits, the second Montreal site and the Quebec City site accounted for 32% each, and the Saint-Jean-sur-Richelieu site provided 15% of the total number of visits.
Of the 72 available variables, 2 were eliminated as being purely administrative in nature (chart number for instance). Of the 70 predictor variables, 10 were eliminated due to lack of pertinence (“date of the last psychiatric hospitalization” for example), 2 because of skewedness (“religion” for example, which was 90% catholic), 2 due to low counts (4th diagnosis/ visit for example), and 4 (3 related to violence, 1 to the pertinence of the consultation process) were the subjects of prior reports.28,29 Of the remaining 52 variables, most were of the nominal type (binary or with multiple subcategories). Variables with a high number of subcategories (such as the 30 reasons for a psychiatric referral) were collapsed into as few logical groupings as possible prior to analysis. The dependent variable (presence of absence of substance misuse) was defined as follows; visits without substance misuse (NSM, n = 13,507 or 73% of all visits), visits where substance misuse was the primary diagnosis, which included patients with a secondary and/or tertiary diagnosis of any type, including substance misuse (PSM, n = 3,034 or 17% of all visits), and visits with a primary psychiatric diagnosis and comorbid substance misuse (CSM, n = 1839 or 10% of all visits).
Analyses consisted of constructing contingency tables where the three substance misuse categories (row variables) were tabulated against a predictor variable (columns). Columns where all cell counts were ≤5% were merged into a generic “other” category and the analysis repeated. Tables where the Pearson's (and likelihood chi-square) ratio
Results
Descriptive variables
A primary substance misuse diagnosis was attributed to 16.5% (3,034 visits) of the total (18,380) number of visits made during the 2-year observation period. A substance misuse diagnosis was also attributed in 31% (2,235 of 7,205) and 33% (589 of 1,788) of visits where a secondary and/or tertiary diagnosis was made, respectively. Overall, substance misuse accounted for 5,858 (21%) of the combined 27,373 diagnoses made during these 18,380 visits.
Three subsets of visits were extracted from the above data for further analyses: NSM, PSM, and CSM. Site differences (as assessed by basic table statistics) were observed regarding the PSM group, ranging from 24% (inner city Montreal site), to 18% (Quebec City site), to 12% at the other sites. The corresponding RRRs, however, were below the index level of 1.5 used to assess clinical significance in this study.
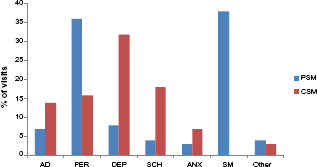
The per substance distribution of the PSM and CSM visits are illustrated in Figure 1. In the majority of cases, alcohol was the substance misused. Combining the alcohol subcategory with “poly-substance misuse” (which typically involved alcohol with another substance), alcohol was responsible for 84% of PSM and 72% of CSM diagnoses. Generally, the greater number of concurrent substance misuse diagnoses, the greater the probability of alcohol being the substance misused. For instance, alcohol was almost twice as likely as all other substances combined (OR 1.7, CI 1.44–2.08,

The relative contributions of the different substances to a primary or comorbid substance misuse diagnosis. 1

Other categories of variables were examined, each appropriate to a given triage phase following a PES referral, to assess whether they might differentiate the three groups.
Variables Available to Staff Prior to Triage
Male gender predominated in both the PSM and CSM groups (65% and 62%, respectively, versus 47% in the NSM group). As illustrated in Table 1, PSM or CSM tagged visits were significantly more likely to be made by men, when compared to NSM tagged visits. No gender difference was found between PSM and CSM groups. Age was examined next and divided into 3 subcategories (18 to 39, 40 to 59, and 60 years of age and above). Both the PSM and CSM groups comprised a significantly younger cohort in comparison to the NSM group. However, this attained clinical significance (RRR ≥ 1.5 or ≤ 0.667) for the CSM group only (Table 1). The age profile for the NSM, PSM, and CSM groups (raw untransformed data for the total sample population) is shown in Figure 4.
Variables available prior to triage and their RRRs 1 (patients without substance misuse were the base outcome).
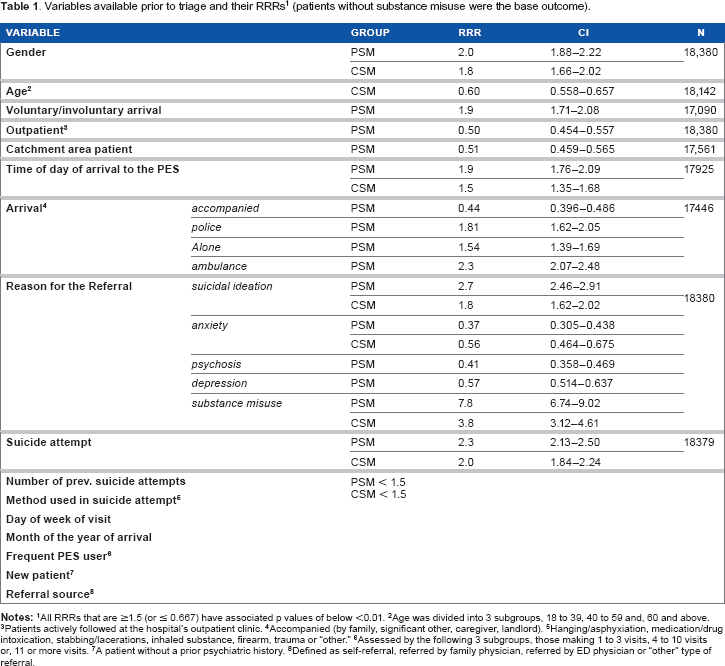
All RRRs that are ≥1.5 (or ≤ 0.667) have associated p values of below <0.01.
Age was divided into 3 subgroups, 18 to 39, 40 to 59 and, 60 and above.
Patients actively followed at the hospital's outpatient clinic.
Accompanied (by family, significant other, caregiver, landlord).
Hanging/asphyxiation, medication/drug intoxication, stabbing/lacerations, inhaled substance, firearm, trauma or “other.”
Assessed by the following 3 subgroups, those making 1 to 3 visits, 4 to 10 visits or, 11 or more visits.
A patient without a prior psychiatric history.
Defined as self-referral, referred by family physician, referred by ED physician or “other” type of referral.
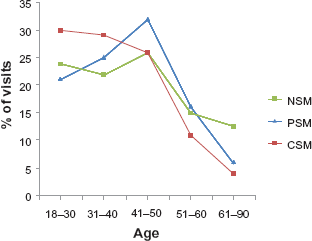
The age distribution of visits tagged as being without, with primary or with comorbid substance misuse.
Time of day, but not day of the week, of arrival to the PES differed between the groups. PSM and CSM patients were more likely than NSM patients to arrive during late evening or night compared to a daytime arrival (18:00 to 7:59 versus 8:00 to 17:59, Table 1). Overall, 36%, 31%, and 23% of PSM, CSM, and NSM patients arrived late evening or night, respectively. Few PES arrivals were on an involuntary basis (26%, 20%, and 15% for PSM, CSM, and NSM, respectively). However, when involuntary arrivals did occur they were more likely to be within the PSM, when compared to the NSM group (Table 1).
Type of arrival to the PES also differed substantially between groups (Table 1). PSM patients in comparison to NSM patients came less frequently to the PES accompanied, and were more frequently brought by ambulance or by police. Clinical variables, such as reasons for a psychiatric referral, were also examined. Referrals for suicidal ideation were significantly more likely than all other reasons combined to be found in the PSM compared to the NSM group. Actual suicide attempts were also more frequently observed in both substance misuse groups compared to the NSM group (Table 1).
Variables Available during Triage
Overall, variables pertinent to drug or alcohol misuse itself possessed the highest degree of significance (Table 2). For example, prior history of substance misuse was found in 95% of PSM visits, 92% of CSM visits, and, surprisingly, 41% of NSM visits. Alcohol and/or drug consumption within 48 hours of the visit was more frequently observed in PSM and CSM patients than in NSM patients (48% and 37% versus 8%, respectively). A present and/or past history of treatment in a detoxification center was found in 61%, 48%, and 28% of PSM, CSM, and NSM patients, respectively.
Variables available at triage and their RRRs 1 (patients without substance misuse were the base outcome).

All RRRs that are ≥1.5 (or ≤ 0.667) have associated p values of below <0.01.
Of any type, both criminal and civil.
None, primary school, high school, college/university.
Apartment, room, supervised apartment, group home, residence for the aged, emergency shelter, temporarily living with relative, home owner, “other.”
Student, welfare, unemployment insurance, retired, insurance, full time job, part-time job, independently wealthy, stay at home spouse, “other.”
Separated, widowed, divorced, common law, married, single.
Separation/divorce, marital difficulties, problematic relationship with “others,” problematic relationship with landlord, illness in self or significant other, death of a significant other, employment difficulties, financial problems, legal problems, trauma, sexual abuse, academic difficulties, “other.”
Being less frequently under active outpatient treatment patients in the PSM group were also less likely to be actively followed by a psychiatrist (Table 2). Otherwise, other than for substance misuse-specific resources, the substance misuse groups did not significantly differ from the NSM group regarding overall psychiatric health care resource utilization (day hospital, hospital-based crisis centers, community-based crisis centers, public medical clinics, private medical clinics, outreach programs, or community resources). PSM patients were also less frequently taking medication, especially antipsychotics. In addition, when taking medication PSM patients were less likely to be compliant (Table 2).
We have previously reported that substance misuse (present or past history) increases the risk of aggressive behaviors upon arrival to the PES. 29 As a corollary, a present or prior history of legal problems was found to be almost three times more likely in PSM when compared to NSM patients (Table 2).
A subjective opinion by the nursing staff of a relationship between substance misuse and the PES visit
The triage nursing staff was asked to provide an opinion as to how directly the PES visit was related to substance misuse. However, only 29% (5,294 of 18,300) of all visits were so assessed (Table 3). Overall, combining visits tagged as having a direct and/or indirect relationship to substance misuse, 92% of PSM and 76% of CSM visits were detected.
Nursing staff opinion as to the relationship between substance misuse and the visit 1

RRR values were 3.2, CI 2.88–3.48,
Interestingly, 34% of NSM visits were tagged with either a direct (17%) or indirect (17%) relationship to substance misuse. In order to determine whether these might represent milder forms of substance misuse, we compared their substance misuse-related variables with those of PSM and CSM tagged visits. As illustrated in Table 4, substance misuse-related variables were all present in NSM visits tagged as directly or indirectly related to substance misuse, albeit with a much reduced frequency.
NSM visits tagged directly or indirectly related to substance misuse compared to similarly tagged CSM and PSM visits.
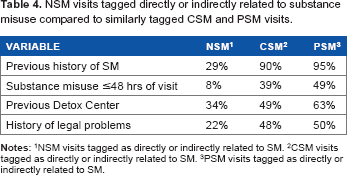
NSM visits tagged as directly or indirectly related to SM.
CSM visits tagged as directly or indirectly related to SM.
PSM visits tagged as directly or indirectly related to SM.
Discussion
This study pooled data acquired in four emergency services, each with a catchment area of between 150,000 and 250,000 citizens. It encompassed a wide socioeconomic spectrum of individuals emanating from rural to inner city areas. As such, our data appears to be a representative sample of the overall population.
The results suggest that patients referred to the PESs for reasons of substance misuse represent a substantial proportion of the overall PES population. They accounted for 21% of all diagnoses attributed, equaling the number of affective or personality disorders diagnoses. This result is fully in line with prior publications showing that substance misuse is an important contributing factor to both psychiatric and medical ED visits.2,5,8,30–32 As for a particular substance misused, alcohol predominated. In fact, most all of the results presented in this paper would have been identical if alcohol alone had been chosen, rather than a combined substance misuse. Our results also support those of previous studies showing that alcohol is primarily responsible for most substance misuse-related PES visits.2,29,33 As in the present study, Curran el al. 2 reported a slight predominance of depressive disorders in their substance misuse comorbid patients. Strict comparisons are difficult, however, as the latter study did not include diagnoses such as personality or adjustment disorders. Indeed, personality disorders predominated, along with substance misuse itself, as secondary or tertiary diagnoses in PSM. That being said, a potential weakness of this study (and of most PES studies where diagnosis is a central issue) is diagnostic stability. In the past few years even the stability of a diagnosis, such as chronic psychosis, which was thought to possess the greatest consistency of a ll psychiatric diagnoses34,35 in the PES, has come into question. 10
Overall, many pre- and during triage non-substance misuse-related variables attained statistical significance in differentiating our three groups. However, none stood out as being intimately related to or even specifically associated with substance misuse. For instance, gender differences were found. Both PSM and CSM tagged visits were more frequently made by men (compared to NSM tagged visits) which appears to be in keeping with the results of several prior publications showing a predominance of men in alcohol and substance misuse disorders.36,37 However, similar gender differences were also found within the schizophrenia/chronic psychosis diagnostic category compared to the combined substance misuse category (64% men each).
Most variables attained modest RRR values between 1.5 and 2.0, with minor exceptions such as suicidal ideation/acts as a reason for a psychiatric referral, which had a 2.7 RRR value in the PSM group. Suicidal ideation or attempts have been shown to be pre sent in a large proportion of alcohol dependent patients.
38
That being said, as was the case for gender, suicidal ideation/attempts were by no means specific to substance misuse and spread rather evenly over adjustment disorders (16%), affective disorders (21%), personality (22%), and substance misuse (27%). Comorbidity with substance misuse has been associated with frequent PES use.2,5,33 In the present study, CSM patients did significantly differ (
Overall, pre-triage and during triage non-substance misuse-related variables appeared to be of questionable usefulness for targeted screening of this disorder. Contrarily, and not unexpectedly, substance misuse-specific variables much more robustly predicted group adherence. For instance, a prior history of substance misuse as well as substance misuse within 48 hours of the visit were, the two most significant variables differentiating the three groups. A history of legal problems (of any type) was observed in 50% of the combined PSM and CSM tagged visits, the highest of all of the broad diagnostic categories.
With few exceptions, variables that predicted PSM visits also predicted CSM tagged visits, albeit less significantly. It might therefore be possible to consider substance misuse as a continuum, ranging from absent up to a primary diagnosis, comorbidity being an intermediary phase. The variables used in this study appeared to scale accordingly. That a younger age was significantly more prevalent in CSM visits suggests that at least some of these patients might, at a later date, be attributed a primary substance misuse diagnosis (rather that a comorbid one).
The subjective impression by the nursing staff of a relationship between substance misuse and a PES visit yielded interesting results. First, less than a third (29%) of visits were so assessed, this despite the fact that all four services were staffed by specialized personnel, each with well over 5 years of experience in the PES setting. Clearly not all nursing staff members felt comfortable in this decision making process. This may in part be due to the fact that we provided only rough guidelines and no formal training so as to better mimic the typical PES setting and maximize the possibility of generalizing our results to less structured PESs. Second, this small (and perhaps less representative) sample size is another major limitation of our study and precludes a definitive assessment of parameters such as sensitivity and specificity. Nevertheless, approximately 92% of PSM and 76% of CSM visits were detected using this simple technique.
Approximately 34% of NSM tagged visits were attributed a direct (17%) or indirect (17%) relationship to substance misuse by the nursing staff. These underwent further analysis in order to determine whether they might approximate what has been frequently called “at risk” behaviors.11,12 Interestingly, those variables intimately associated with substance misuse in the PSM and CSM groups were also present in these patients, albeit at a much lower frequency. Again, it is possible that those variables are most intimately tied to the substance misuse scale from “at risk behaviors” up to and including primary substance misuse.
Conclusion
Clinical services are continually called upon to better define and target their core patient populations in order to maintain (or increase) quality of care. Visits made by substance misuse patients occur at a high frequency and, compared to NSM visits, are significantly less likely to result in a hospitalization. In a previous report, psychiatric staff at these same four PESs were asked to provide a subjective opinion as to the pertinence and urgency of a given PES visit. Almost 50% of substance misuse visits were tagged as neither pertinent nor urgent. 28 As such, the rapid identification and triage of substance misuse visits to, whenever possible, less costly resources such as publicly or privately funded substance misuse treatment centers would appear to be a valid and pertinent endeavor.
Most common variables do not cluster towards substance misuse at the exclusion of the other broad diagnostic categories and, as such, appear to be doubtful candidates for the rapid triage of these patients. The few variables that do cluster do so because of an intimate relationship with substance misuse itself. In the present study, the subjective opinion by the nursing staff as to the relationship between a visit and substance misuse had a very limited scope. Nevertheless, this opinion appears promising and warrants further investigation to determine whether a more formal integration into the triage process, along with minimal training, might substantially increase its usefulness.
Author Contributions
As primary author for this article, YC takes full responsibility for the design of the trial, for data acquisition, data analysis and data interpretation and the writing of the manuscript.
M-JL, the chief coordinator of the trail, had significant input as to the design of the database and had full responsibility for the actual implementation of the study at all sites. She also had significant input as to the interpretation of the results and the conceptualization (not the writing) of the manuscript.
MP, LB and EL were site principal investigators. They had significant input as to the design of the database and had full responsibility for the actual implementation of the study at each individual site.
All authors reviewed and approved of the final manuscript.
Disclosure and ETHICS
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
Acknowledgements
The authors would like to thank the following site-specific principal investigators as well as their supporting clinical and administrative staff: Edith Labontέ, MD, Lucie Beaulieu, MD, and Michel Paradis, MD.
This data has in part been presented at the 62nd Annual conference of the Canadian Psychiatric Association, Montreal, Quebec, Canada, September 28th, 2012.