
Abstract
Objective
To investigate the therapeutic effectiveness of percutaneous fascia release to treat chronic recurrent gluteal myofascial pain related to recurrent tendonitis or bursitis at the attachment sites.
Methods
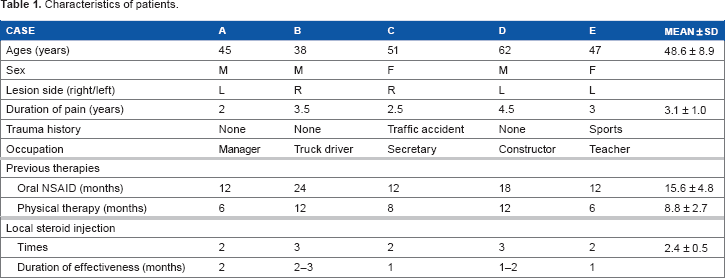
Five patients (three males, two females; aged 48.6 ± 8.9 years) with myofascial trigger points in the gluteus medius muscle were treated. Outcome measures, including pain intensity, pressure pain threshold, and the relative strength of hip abduction, were assessed before, immediately after, and six months after the treatment. The data measured before and after treatment (different times) on visual analog scale, pressure pain threshold, and relative hip abduction strength were analyzed by Wilcoxon signed-rank test and paired t-test, respectively, for the comparisons between time points.
Results
Reduction in pain intensity and increase in the pressure pain threshold and the relative hip abduction strength were found in all five patients after treatment when compared with those of before treatment (P < 0.05). Moreover, all of these improvements existed for at least six months (P > 0.05).
Conclusions
Percutaneous fascia release of gluteal muscle insertion sites can be used to treat chronic gluteal pain related to subtrochanteric bursitis to avoid recurrence, if other treatment cannot control the recurrence, although this was demonstrated only on a small sample size without control and blind assessment in the pilot study.
Keywords
Introduction
Gluteal pain is commonly (10%-25% of the general population with increased prevalence in women) associated with low back pain or as a single complaint related to other lesions such as sacroiliac joint lesion, ischial tuberosities bursitis, or subtrochanteric bursitis. 1 6 Subtrochanteric bursitis is a commonly diagnosed inflammatory condition that presents with pain in the gluteal region, including the greater trochanter, often with radiation down the lateral aspect of the thigh, 1 6 exacerbated by lying on the affected side, with prolonged standing or transitioning to a standing position, sitting with the affected leg crossed and with climbing stairs, running or other high-impact activities. 6 In addition to the localized pain in the greater trochanter region, it can also cause myofascial pain in the gluteal muscles. 4
A myofascial trigger point (MTrP) is classically defined as the most irritable spot in a taut band of skeletal muscle,7,8 and currently considered as the accumulation of sensitized nociceptors.9,10 A latent MTrP, which is only tender but not painful, spontaneously can become an active MTrP with spontaneous pain via peripheral sensitization or central sen-sitization as a consequence of a lesion near or remote to this MTrP. 9 12 An active MTrP can be inactivated after appropriate myofascial pain therapy 7 but recurred frequently if the underlying etiological lesion is not completely removed.9–11,13–15 The diagnosis of trochanteric bursitis is usually based on physical examination, and the criteria include lateral hip pain, discrete tenderness at the greater trochanter, pain on hip abduction against resistance, pain radiating down the lateral aspect of the affected lower limb, and a positive Patrick-FABERE test (flexion, abduction, external rotation, and extension of hip joint).3,6 This condition should initially be managed conservatively with rest, nonsteroidal anti-inflammatory drugs (NSAIDs), and stretching or physical therapy.4,16,17 An injection of corticosteroid into the trochanteric bursa may be given for both diagnostic and therapeutic purposes.
Surgical release of iliotibial band or surgical debridement of the bursa is indicated only if the patient has poor response to conservative therapy. To avoid excessive tissue damage and bleeding, we applied the new technique developed by Lin et al 18 for the percutaneous release of adhesive soft tissues between the tendon sheath and the periosteum. This technique has been used successfully for the relief of recurrent myofascial pain in the forearm and is much less invasive compared to the surgical technique reported previously. In this preliminary pilot study, we report the quantitative effectiveness of percutaneous fascia release for treating recurrent gluteal myofascial pain due to subtrochanteric bursitis. The study was approved by the Institutional Review Board of the China Medical University Hospital. Patients gave their written, informed consent to participate in this study, and the research was conducted in accordance with the principles of the Declaration of Helsinki.
Materials and Methods
Selected Subjects
In our pain clinic, a total of 21 patients with hip pain were screened for eligibility. The flow diagram was shown in Figure 1. This study achieved full enrollment, with five of seven eligible patients enrolled in our study. One patient refused to participate in this study and another one withdrew due to intolerant pain. A total of five participants completed the study and were included in the analysis.
Flow diagram of the pilot study.
The inclusion criteria include the following: (1) had chronic pain in the gluteal region and ipsilateral subtrochanteric bursa region for more than a year, (2) had been diagnosed as subtrochanteric bursitis with active MTrPs in the gluteus medius muscle, (3) received treatments with physical therapy and oral NSAIDs for more than six months, and (4) received local steroid injection to the subtrochanteric bursa with temporary pain relief but pain recurred within three months. Patients with cognitive deficit, history of neurological or orthopedic disorder of the involved lower limb other than the current complaint, any serious medical problem, or pregnancy were excluded from this study.
The diagnostic criteria of subtrochanteric bursitis were: (1) pain and tender over the subtrochanteric bursa, (2) active resistive contraction of hip abductors-induced pain similar to clinical complaints (pain recognition), and (3) pain elicited by flexion, abduction, external rotation, and extension of the ipsilateral hip (positive Patrick-FABERE test).3,6
The diagnostic criteria of myofascial pain of gluteus medius muscle included (1) having active MTrPs in the ipsilateral gluteus medius that were the most tender spots at the prominent muscle belly of gluteus medius muscle as demonstrated in Travell's trigger point manual 4 and (2) having referred pain or referred tenderness to the surrounding area as shown in the same book. 4
Characteristics of patients.
Procedure of Percutaneous Fascia Release
The procedure of percutaneous fascia release is completely similar to that reported previously by Lin et al, 18 which has been ethically approved by the Ethics Committee. A blunt cannula was used for the release of the adhesive tissues in the greater trochanteric bursa region. 18 This cannula was connected to a 10 cc syringe that contained 8-10 mL of 1% lidocaine and 3 mL of sodium hyaluronate (ARTZ Dispo® 25 mg, molecular weight 60-120 million). The addition of local anesthetic could also provide the immediate relief of pain and also to obtain the information about the effectiveness of this procedure after the treatment immediately, and hyaluronic acid was also added for lubrication to avoid re-adhesion.
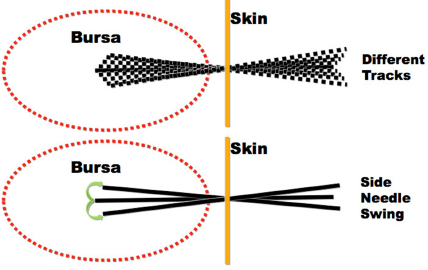
Initially, the skin around the subtrochanteric bursa was cleaned up with butadiene, and the site for needle penetration (about 5 cm away from the tendon insertion site of gluteus muscle) was anesthetized with 1 mL of 1% lidocaine. Then the skin was penetrated with an 18G injection needle to make a hole for the penetration of this blunt cannula. The cannula was inserted into the hole and pushed toward the painful region (usually in the bursa) slowly when the needle tip touches the bone margin, which is the exact depth the needle was advanced (Fig. 2). In addition to the forward needle movement, side movement for about 10° was also provided to release the adhesion of soft tissues in the subtrochanteric bursa region below the tendon of gluteus medius around this track (Fig. 3). During the needle movement, a drop of the solution in the syringe was injected whenever the patient complained of any pain or discomfort from the needle movement. As soon as the resistance of the needle movement subsided, the needle was pulled back to the subcutaneous layer and then turned to another direction (about 10° away from the original track) for a new track of penetration. This procedure was repeated in different directions (new tracks) similar to the multiple insertion technique of MTrP injection,
14
so that the blunt cannula was moved in-and-out to penetrate into different tracks for a comprehensive release of adhesive soft tissue. Finally, this cannula could sweep around the subtrochanteric area freely (for an angle about 30°-40°) with no resistance since all adhesions had been released. Then the needle was pulled out and the open wound was compressed to avoid bleeding, and this procedure was completed.
Needle insertion into trochanteric bursa region. Needle insertion into different tracks (up) and swing movement of needle in a track (low).
Outcome Assessment
As shown in Figure 4, we measured pain intensity, pressure pain threshold, and relative hip abduction strength before, immediately after, and six months after the needle treatment. A well-trained study nurse, who had participated in the outcome measurement work for more than three years in our laboratory, measured and analyzed the outcome assessments and was blind to the aims of the study. Before this study, we have reassessed the reliability and validity of the pressure algometer for pressure pain threshold and dynamometer for hip abduction strength. Both instruments were convenient to apply and comfortable for the patient and have been statistically tested to determine actual validity and reliability.
Schedule for outcome assessment.
Subjective Pain Intensity
The subjective pain intensity over the gluteal region was assessed based on the patient's subjective feeling before, immediately after, and six months after the treatment. It was rated with a “visual analog scale,” which was a horizontal line, 100 mm in length, anchored by the words “No pain” at the left side and “Very severe pain” at the right side. The patient was asked to mark a point on the line that he felt to represent his perception of his current pain state. The score was determined by measuring in millimeters from the left end of the line to the point that he marked. It was also instructed to the patient that the pain with a value at or below 5 of 10 should be considered as a tolerable pain.
Pressure Pain Threshold
The most tender site at the ipsilateral subtrochanteric bursa was assessed with a pressure algometer for pressure pain threshold before, immediately after, and six months after the treatment. 19 The patient was in a comfortable lateral lying position on the contralateral side and encouraged to maintain complete relaxation. Then the most painful spot in the ipsilateral subtrochanteric bursa was marked to confirm the consistent sites for the three consecutive measurements. A pressure algometer 19 was used to measure the pressure pain threshold. This pressure algometer (J-Tech Commander Algometer) was applied on this marked site with the metal rod (standard 1 cm2 in size) perpendicular to the surface of the skin. Then it was compressed to gradually increase the pressure of compression at a speed approximately 1 kg/second. The compression stopped when the subject reported any distinct increase of pain or discomfort. At this point, the reading on the algometer was recorded as the value of pressure pain threshold. The patient was asked to remember this level of pain or discomfort at that point for a consistent standard to apply for the next measurements. Three repetitive measurements at an interval of 60 seconds were performed at each site. The average values of the three readings (kg/cm2) were used for the data analysis. All measurements for all subjects at different times were performed by the same well-trained examiner. This procedure was performed before and shortly after the needle treatment and again at the follow-up time about six months after the treatment.
Relative Hip Abduction Strength
Ipsilateral hip abduction strength was measured with a dynamometer before, immediately after, and six months after the treatment. The dynamometer was placed over the lateral aspect of the ipsilateral knee on the lateral collateral ligament near the knee joint axis to measure the hip abduction strength. Then the patient was requested to forcefully push the dynamometer toward the lateral aspect when the knee was in a full extension position and hip in the neutral position, so that the hip was doing abduction movement. Three maximal efforts were tried for each assessment. The average of these three force values (kg) was used for the data analysis. Then the control side (nonpainful side) was also measured with the same procedure. The force measured from the ipsilateral (painful) side was expressed as the percentage of the nonpainful side for final data, so that the relative hip abduction strength can be expressed as “relative abduction strength = (force in painful side/force in control side) × 100%.”
Statistical Analysis
All data are expressed as mean ± standard deviation. The data measured at different times (before and after the needle treatment) on visual analog scale were analyzed by Wilcoxon signed-rank test. Repeated measures analysis of variance was used to determine the differences on pressure pain threshold and relative hip abduction strength in three time points of before, immediately after, and six months after the treatment. Paired t-test was used to examine post hoc for the comparisons between times. A P-value of < 0.05 was considered statistically significant. All data were analyzed using SPSS version 17.0 for Windows (SPSS Inc.).
Results
Improvement in Subjective Pain Intensity
Subjective pain intensity before and after treatment.

Indicates a significant difference for the data compared with those of before treatment (P < 0.001).
Improvement in Pressure Pain Threshold
Pressure pain threshold (kg/cm2) before and after treatment.

Indicates a significant difference for the data compared with those of before treatment (P < 0.01).
Indicates no significant difference for the data compared with those of immediately after treatment (P > 0.05).
Improvement in Relative Hip Abduction Strength
Relative strength of hip abduction (% of control) before and after treatment.

Indicates a significant difference for the data compared with those of before treatment (P < 0.01).
Indicates no significant difference for the data compared with those of immediately after treatment (P > 0.05).
Discussion
Important Finding in this Study
It has been found in this pilot study that there was improvement in subjective pain intensity, pressure pain threshold at the painful site, and relative hip abduction strength of the involved hip immediately after percutaneous fascia release over the subtrochanteric bursa in treating chronic myofascial pain of the right gluteal region. This effectiveness lasted for at least six months.
Myofascial Pain Related to other Soft Tissue Lesion
In a recent similar study, it was demonstrated that percutaneous soft tissue release of the lateral epicondyle can effectively control the pain of lateral epicondylitis for a significant long period and also control the myofascial pain of the hand extensors. 18 The evidences of the association between active MTrPs and lesions of nonmuscular origins have been documented.10,20–23 In a previous study, 21 the corrections between specific muscles with active trigger points and cervical lesion at specific level (magnetic resonance imaging finding) were analyzed. Therefore, we consider that the MTrP in the upper trapezius muscle is activated by the facet dysfunction in such cases. From this study, we have further demonstrated that the active MTrPs are frequently associated or related to the underlying pathological lesion remote to the MTrP site, and it is important to treat the underlying etiological lesion for long-term relief of myofascial pain due to MTrPs.9–11,15
Mechanism of Percutaneous Fascia Release for Pain Relief
Healing process for the chronic recurrent inflammatory lesion in the subtrochanteric bursa may produce fibrosis and subsequently elicit adhesion of soft tissues in the subtrochanteric bursa region. This chronic inflammation may be directly caused by tendon trauma near the bursa area (either acute pull or chronic repetitive minor trauma). At the same time, the MTrP in the gluteus medius muscle (or even other gluteal muscle) may be activated due to the lesion of its tendon at the greater trochanteric region.10,12 The tendon trauma can be further aggravated by the tension of the MTrP taut band of the gluteus medius. This can elicit a vicious cycle of the gluteal MTrP pain and subtrochanteric trochanteric bursa pain. Another vicious cycle may be established by the possible formation of the attachment trigger point near the tendon that can be caused by the chronic tension produced by the taut band of that MTrP.
24
It is also very likely to cause adhesion in the attachment trigger point region and further activate the MTrP of gluteus medius muscle via central sensitization. This condition can elicit another vicious cycle or enhance the whole vicious cycle (Fig. 5).
18
Therefore, when the adhesive tissue is released, the whole vicious cycle can be interrupted.
Vicious cycle of hip and gluteal pain.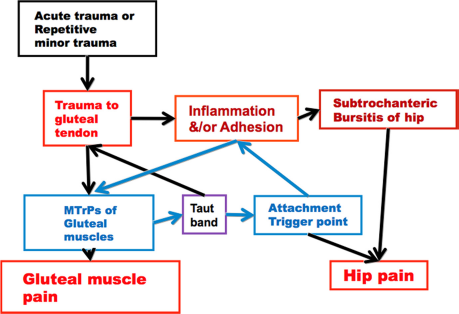
In addition to the release of adhesive tissue, another possible mechanism is the anti-inflammatory effect due to local steroid injection into the adhesion region to inhibit the inflammation to interrupt this vicious cycle.18,25 Since anti-inflammation effect is not an immediate reaction, and we can observe the immediate pain relief after the release of soft tissue, the anti-inflammatory effect from local steroid injection is not an important mechanism for the immediate pain relief. The immediate pain relief may be related to “hyperstimulation analgesia” from the needle stimulation,26,27 mediated via the descending pain inhibitory system, 28 32 similar to MTrP injection or acupuncture.11,15,33 Strong stimuli to nociceptors can elicit strong neural impulses to the spinal cord interneurons, including the hypothetic “MTrP circuit” of an MTrP,11,15 to inhibit the vicious cycle of pain and also activate the descending pain inhibitory system, and thus provide an immediate pain relief. Therefore, this procedure may also provide a hyperstimulation analgesic effect to activate the descending pain inhibitory system, in addition to the adhesion release and anti-inflammatory effect.
In clinical practice, the evidence of inflammation (such as simple tendinitis and bursitis) is usually based on clinical examination of redness, swelling, local heat, and local pain. Sonography or magnetic resonance imaging is usually performed when the document of complication or chronic changes (such as calcification, osteophytes, and fluid accumulation) is necessary. Therefore, we do not have such tests for all of our patients.
Advantage of Noninvasive Procedure
It has been reported that the surgical approach to treat trochanteric bursitis can provide a good pain relief.16,17,34–36 They considered that soft tissue adhesion is a basic lesion to cause recurrent pain. However, although most patients improve using the described therapeutic program, none of this treatment procedures used in trochanteric bursitis have been compared with a placebo in a controlled trial. 1
Similar to the previous study 18 in treating lateral epicondylitis, the percutaneous technique had a lower complication rate than the surgical open approach of invasive tenotomy. 37 40 It can be performed as an office procedure with less cost. The new technique recommended by Lin et al 18 is actually similar to a procedure of percutaneous release of adhesion performed by orthopedic surgeon with a knife or a 18K needle. 41 The only major difference between these two procedures is that a blunt cannula instead a sharp knife or needle is used in this new procedure. Using this new procedure, the recovery period can be much shortened, and the patient has less suffering.
Sonography is usually applied for percutaneous fascia release. However, the resolution power for ultrasound is still limited to identify the minor adhesion clearly and have some metal artifact. In our clinical practice, the adhesion tissue can be perceived during our “blind soft tissue release.” We can feel the resistance of the needle movement, even a minor adhesion. In fact, Lakhey et al 41 performed this procedure blindly and had obtained good results.
Limitation and Requirement of Further Studies
In our pilot study, the sample size was small, so that substantial risk of bias was possible. We had no control group for comparison. The design was not blinded in assessment and not randomized. The difficulty in patient selection is the major reason. Since the statistical analyses showed significant changes in these three outcome assessments, including both subjective and objective assessments, the information still can provide therapeutic effectiveness of this technique. Also, the preferred leg of the subjects and central fatigue processes might be the confounders. In the future study, it is necessary to have a large sample size with a control group and blinded assessments for a longer period of follow-up to further confirm the effectiveness of this technique.
Conclusion
In this pilot study, we have demonstrated the therapeutic effectiveness of percutaneous fascia release in treating chronic myofascial pain of the gluteus medius muscle related to subtrochanteric bursitis. It is much less invasive than the surgical procedure. It can be recommended for the treatment of recurrent subtrochanteric bursitis associated with active myofascial pain of the gluteal muscles when other conservative procedures, such as oral medicine, physical therapy, or local steroid injection, cannot provide long-term effectiveness.
Author Contributions
Conceived and designed the experiments: MTL and CZH. Analyzed the data: YLH. Wrote the first draft of the manuscript: HSC. Contributed to the writing of the manuscript: HSC, CZH, and LWC. Agree with manuscript results and conclusions: HSC, MTL, CZH, YLH, and LWC. Jointly developed the structure and arguments for the paper: HSC, CZH, and LWC. Made critical revisions and approved the final version: CZH and LWC. All authors reviewed and approved the final manuscript.