
Abstract
Assessment of balance control is essential to guide physical rehabilitation poststroke. However, current observational assessment tools available to physiotherapists provide limited information about underlying dyscontrol. This paper describes a force plate-based assessment of quiet standing balance control that we have implemented for individuals attending inpatient stroke rehabilitation. The assessment uses two force plates to measure location of ground reaction forces to maintain stability in quiet standing in five conditions (eyes open, eyes closed, standing symmetrically, and maximal loading on the less-affected and more-affected limbs). Measures of interest are variability of the centers of pressure under each foot and both feet combined, weight-bearing asymmetry, and correlation of center of pressure fluctuations between limbs. We present representative values for the above-mentioned measures and case examples to illustrate how the assessment can reveal patient-specific balance control problems and direct treatment. We identify limitations to our current assessment and recommendations for future research.
Introduction
Function- and impairment-based assessments are an important component of rehabilitation practice. Standardized assessment tools can help to identify patient-specific problems that should be targets for rehabilitation; track patient progress over time; make predictions about recovery (eg, length of stay or discharge destination); and communicate all of the above to the interprofessional care team, patients, and their families. 1 3 The most commonly used outcome measures for assessing balance control within neurorehabilitation practice are performance-based observational rating scales (eg, the Berg Balance Scale). 4 However, the overall score obtained from these types of scales has limited ability to inform patient-specific impairments as patients can use compensatory strategies to achieve a higher score on certain items. For example, one item on the Berg Balance Scale involves standing on one leg for as long as possible. This item is administered by allowing patients to choose which leg to stand on; individuals with unilateral impairments, such as those with stroke-related hemiparesis, can achieve a higher score by standing on their less-affected leg. It is possible that physiotherapists use their observations of patients performing tasks within these scales, rather than the total score, to inform care. 2
When standing still, the central nervous system aims to keep the center of gravity within the base of support. 5 Therefore, the amount of movement of the center of gravity (or postural sway) is considered an indicator of the integrity of the balance control system; less postural sway generally indicates greater stability 6 and, therefore, “better” balance control. Performance-based outcome measures do not directly measure postural sway or how well the center of gravity is contained within the base of support; this is most accurately done with three-dimensional motion analysis. However, current three-dimensional motion analysis systems typically require substantial set-up (eg, to place markers on the patient) and/or postprocessing time, which presents a significant barrier to implementation in clinical practice. Force plates can be used to provide reasonable estimates of postural sway through integration of shear forces recorded during quiet standing. 7 Furthermore, force plates can directly measure the location of the centre of pressure (COP) beneath the feet; it is by changing the location of the COP that individuals control the location of the center of gravity in quiet standing. 8 Thus, force plates can quantify postural sway (ie, center of gravity motion) and provide information about how sway is controlled (ie, COP motion) when standing still.
This paper presents our perspectives on the use of force plates for assessing quiet standing balance control within stroke rehabilitation practice. Our perspectives are influenced by clinical experience and research conducted by our group and other groups. We describe the development of a standard force plate-based quiet standing assessment, how the results of the assessment can be used in clinical practice, limitations of the current assessment, and recommendations for future research to develop both feasible and clinically meaningful assessment tools.
Assessment
The Balance Mobility and Falls Clinic is a partnership between the Research and Brain and Spinal Cord Rehabilitation Programs at the Toronto Rehabilitation Institute, University Health Network. The clinic was established in 2009 to facilitate knowledge exchange and accelerate the application of new technology and findings to patient care. Collaboratively, researchers and clinicians within the Balance Mobility and Falls Clinic developed an assessment to evaluate the aspects of balance and gait, integrating technological measures and commonly used clinical measures.9,10 This paper focuses on our current practices around one aspect of this larger assessment: the assessment of quiet standing balance control. The clinic provides routine assessment to all individuals admitted to the hospital for inpatient rehabilitation following stroke or acquired brain injury; however, the current paper focuses on our assessment practices for individuals with stroke.
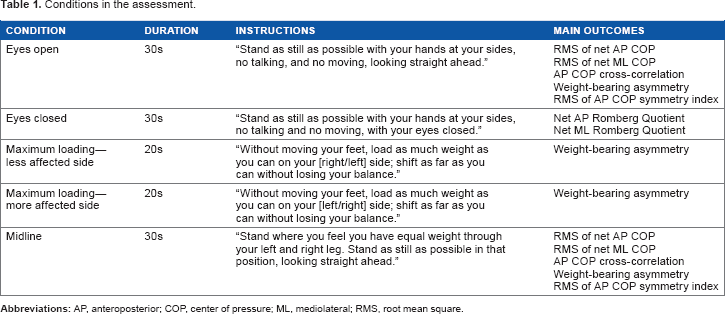
Conditions in the assessment.
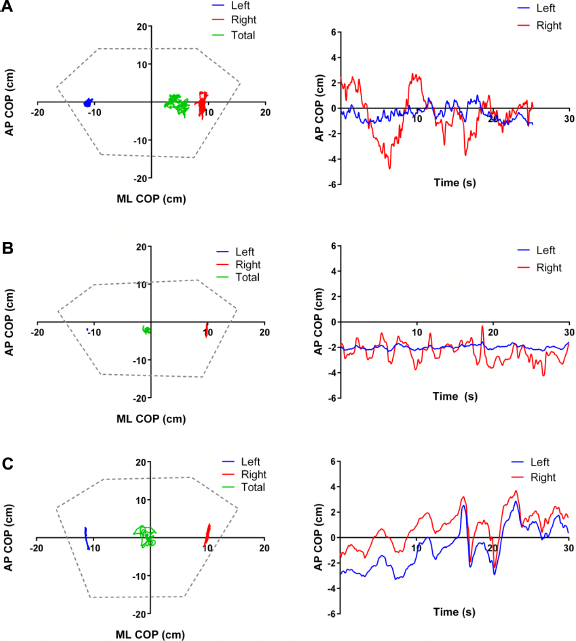
Examples of COP tracings for three patients in the eyes open condition. The figures on the left show the two-dimensional [anteroposterior (AP) and mediolateral (ML)] centers of pressure (COP) recorded by the left and right force plates and the net (total) AP and ML COP for both force plates combined. The figures on the right show the corresponding time series of left and right AP COP for each patient. Note that data were cropped from the end of the trial for patient A such that < 30 seconds are displayed. Also note that the excursion of the COP under the left foot for patient B is so small as to be almost imperceptible on this figure.
Force plate data are collected at 256 Hz on a desktop computer via a BNC terminal block and A/D board (models BNC-2111 and PCI-6229, respectively, National Instruments) and custom-written Labview routine (version 12.0.1f5, National Instruments). Trial meta-data (eg, patient number, trial number, duration, and any notes regarding the trial) are collected with the raw force plate data. Data are stored and processed after the assessment with a custom-written Matlab routine (version 7.4.0.287, The Mathworks, Inc.) using the following steps:
The raw voltages are converted to forces and moments using the calibration coefficients provided by the force plate manufacturers. The forces and moments are filtered using a low-pass zero phase lag fourth-order Butterworth filter at 10 Hz. The anteroposterior (AP) and mediolateral (ML) COP are calculated separately for each force plate, and the net COP is calculated for both force plates. The net vertical force and COP data are presented, and the user has an opportunity to crop data from the start or end of the trial (eg, prior to a sudden increase in vertical force as a result of the physiotherapist stepping on the force plate). Outcome variables of interest are calculated (see the following section).
Outcomes and Interpretation
We recommend outcomes that are easily interpreted and provide quantitative and complementary information about control of quiet standing balance control among individuals with stroke. These measures are weight-bearing asymmetry, Romberg quotient, root mean square (RMS) of the net AP and ML COP, AP cross-correlation, and symmetry index. Detailed definitions and general interpretation of these variables are presented below. It is important to note that assessment results for individual patients should be interpreted together and in light of other clinical assessments (eg, motor recovery, sensation, cognition, etc.).
Weight-bearing asymmetry is the mean vertical force recorded by the force plate under the more-affected limb, expressed as a percentage of total body weight. This is a measure of how evenly body weight is distributed between the limbs. Individuals with stroke may stand asymmetrically because of impaired motor control on the more-affected side13,14 and/or because of a biased egocentric reference frame.
15
Generally, individuals with stroke tend to bear more weight on the nonparetic than the paretic limb,
16
although significant asymmetric stance with more weight on the paretic limb has also been observed.
13
High weight-bearing asymmetry in quiet standing is correlated with decreased walking speed
17
and greater asymmetry of spatiotemporal characteristics of walking among individuals with stroke.17,18 For the maximum loading conditions, the capacity to load the paretic limb is generally less than the nonparetic limb.
19
Increased capacity to load the paretic limb is correlated with increased walking function
20
and reduced stance time asymmetry in walking poststroke.
18
Test-retest reliability is high for weight-bearing asymmetry during quiet standing (ICC = 0.95 for the mean of two 30-second trials) and maximal loading (ICCs = 0.93-0.99 for the mean of five six-second trials) among individuals with chronic stroke.
16
RMS of net AP and ML COP are measures of the variability of the COP displacement under both limbs combined; RMS of COP is calculated separately for the AP and ML directions. RMS of COP is a recommended measure of stability within clinical posturography.
21
As the position of the COP and center of gravity are correlated, high RMS of COP suggests high postural sway.
22
Therefore, high RMS of COP can be generally interpreted as poor overall balance control. There is some evidence that increased RMS of ML COP is related to increased risk for falls after discharge from inpatient stroke rehabilitation.
23
Romberg quotient is the RMS of net AP or ML COP in the eyes closed condition divided by the RMS of net AP or ML COP in the eyes open condition.
24
Values greater than 1 are typical, but values that far exceed 1 suggest that patients rely on visual information to control balance. The upper limit of the 95% confidence interval of the Romberg quotient for older adults who are not at increased risk of falls is 1.1 (ML) or 1.3 (AP);
25
therefore, Romberg quotients that exceed these values may suggest impaired performance. AP cross-correlation is the cross-correlation between the AP COP of the left and right limbs. As control of standing balance in the AP direction is primarily achieved through action of the plantar- and dorsiflexors
8
and both ankles can act independently in quiet stance,
26
the AP cross-correlation provides a measure of how well actions of the two ankles are synchronized in time.27,28 The correlation coefficient at zero lag is reported as there appears to be little value in examining the maximum correlation coefficient and the lag at which this maximum occurs.
28
The cross-correlation value can range from —1 to +1, with values close to +1 indicating that the two limbs are almost perfectly synchronized in time. There is emerging evidence that low cross-correlation values are related to increased risk of falls among individuals with stroke during inpatient rehabilitation
29
and after discharge into the community.
23
Symmetry index is the RMS of AP COP on the less-affected side divided by the sum of the RMS of AP COP on both sides.
30
This provides a measure of the contribution of each limb to AP balance control; a value of 0.5 indicates that both limbs contribute equally to balance control, whereas less than 0.5 indicates that the more-affected side contributes more, and greater than 0.5 indicates that the less-affected side contributes more to balance control. Reduced symmetry index predicts increased risk for falls in daily life after discharge from inpatient stroke rehabilitation.
23
Participant characteristics.

Notes: Values presented are from individuals with stroke assessed in our clinic at admission and/or discharge from inpatient rehabilitation over a three-year period (n = 359 total). Values are means with 95% confidence intervals in brackets for continuous or ordinal variables, or number with percentage in parentheses for categorical variables. Note that percentages are subject to rounding error and might not sum to 100.
Data for measures calculated for each condition.

For the purpose of clinical interpretation, comparison to reference values for healthy young and older individuals, where available,28,31 can help to determine if an individual patient has impaired performance on a measure. The above measures tend to be correlated with each other within the subacute stroke population when performing the task of standing still with “preferred” weight distribution (ie, the “eyes open” condition within our assessment). Thus, individuals with values suggestive of impaired balance control on one measure will likely show impairment on all other measures. 28 However, measures can also be dissociated, and examination of separate measures for one individual can provide information about specific impairments in balance control.
Individual patient data.

Patient B has bilateral impairment, but the physiotherapist noted more sensorimotor impairment on the left than the right side. The values obtained from the force plates correspond to the eyes open trial illustrated in Figure 1.
Likewise, assessment results for other conditions could inform specific treatments; for example, a high Romberg quotient could suggest that practicing balancing tasks with eyes closed or in dim lighting might be beneficial for that patient. Shifts in limb load during eyes closed tasks may provide information to the physiotherapist regarding the individual's use of compensatory strategies to increase sensory information when vision is not available to control balance. Comparing midline to usual stance conditions can provide insights into underlying dyscontrol contributing to postural asymmetries. Maximal loading conditions allow the physiotherapist to differentiate between the capacity to load each limb versus the preferred use of the nonparetic limb as a support function.
Discussion
We have implemented a simple force plate-based assessment of quiet standing balance control into routine care in inpatient stroke rehabilitation. Both patients and physiotherapists feel that the assessment provides specific quantitative information; this information can help patients understand their balance problems and is useful for confirming physiotherapists' clinical reasoning. 10 However, while we have suggested within this paper that the assessment may be useful to reveal underlying dyscontrol that can be targeted, with treatment, to patient-specific balance impairments, physiotherapists have not clearly articulated that such assessments inform care. 10 Clinical interpretation of values from technological measures is cited as an ongoing challenge. 10 Instrumented assessment of balance control is currently not taught within many physiotherapy entry-to-practice degree programs; therefore, additional educational modules for physiotherapists could be developed to help physiotherapists to use the information gained from the assessment to inform practice. The assessment cannot stand alone, and the results must be interpreted in light of other sensorimotor assessments. To aid clinical interpretation, comparison values from healthy age-matched individuals may be useful to identify if a balance control problem exists (if not otherwise apparent) or if the problem can be attributed to stroke rather than age; however, such comparisons provide limited diagnostic information. 32 Additionally, comparison to healthy age-matched reference values may not be appropriate if the systems and methodology used to collect the reference data differ from those used in the clinical setting. 33 Feedback from physiotherapists suggests that providing the visual representations of the COP tracings (Fig. 1) alongside the data aids in interpretation of the values. 10
For assessing quiet standing balance control among individuals with stroke, who often have lateralized impairments, we believe it is essential to use two force plates to provide information about how the two limbs work together and how each limb contributes to whole-body balance control (ie, AP cross-correlation and Symmetry index). Improving weight-bearing symmetry is often a focus of various therapeutic interventions that are designed to “force” use of the paretic limb. 34 37 In the absence of quantitative data, the capacity to weight-bear on the paretic limb can be used as a proxy measure of improved contribution of the paretic limb control to balance. However, improvements in paretic limb load can occur without associated improvement in its contribution to balance control;22,34 this dissociation between weight-bearing and control asymmetry is apparent in patient B. Changes in functional performance (eg, as measured by observational rating scales) can also improve despite little evidence of restoration of the paretic limb's contribution to balance control.22,38 Therefore, we believe it is essential to differentiate between simple loading asymmetry and asymmetries in limb contribution to balance control to unmask dyscontrol underlying observed patient performance. This kind of specific information allows physiotherapists to determine what aspects of balance control change with intervention, and thus inform new intervention approaches.
This paper describes an assessment of “static” balance control when standing still. However, balance control is also required in “dynamic” situations, such as when moving (eg, walking) and in response to external postural perturbations. 39 Instrumented assessment of anticipatory balance control during voluntary movement 40 and reactive balance control following a loss of balance 9 could provide further specific and quantitative information about a wider range of balance skills in stroke rehabilitation practice.
The test-retest reliability of weight-bearing a symmetry has been established within the chronic stroke population.16,41–43 However, to our knowledge, reliability of weight-bearing asymmetry or our other recommended measures have not been established within the subacute stroke population. This is an acknowledged limitation of the current assessment and an important area for future research to enable these measures to be suitable for widespread clinical uptake.
We recommend seven complementary measures to describe quiet standing balance control poststroke that are easy to calculate and are, therefore, easily understood without requiring expertise in signal processing. However, others have used many different measures to quantify the COP in quiet standing 3 (eg, COP area or velocity; for further examples, see Refs. 31, 44). It is possible that inclusion of other measures would provide a more complete picture of quiet standing balance control poststroke. In particular, others have suggested that advanced measures of the dynamical properties of the COP 45 may provide additional insights into balance control problems among individuals with stroke. The potential clinical utility of such measures is promising, but further research is required to provide meaning to these measures and to establish the “best” measures for quantifying quiet standing balance control poststroke.
Our assessment protocol includes some departures from recommendations for clinical posturography made previously.21,33 In the interest of comfort, patients are assessed wearing their usual footwear rather than barefoot. It was previously suggested to position the feet with heels touching; 21 however, if the feet are touching, the forces and moments recorded under one foot are influenced by actions of the other foot, which prevents examination of individual-limb contributions to balance control. Furthermore, there is evidence that weight-bearing asymmetry may be exacerbated when the feet are touching. 46 Thus, we selected a more natural, yet standardized, foot position, 12 with the feet approximately below the hips and the toes slightly angled out. The trial duration used is lower than recommended for optimal reliability of force plate recordings.44,47,48 Likewise, reliability could be improved by averaging values obtained from multiple trials.44,47 However, we feel a longer sampling duration or conducting more trials would be problematic within this stroke population because of potential for fatigue and poor attention, 33 which could adversely affect reliability of the measures obtained. 43
Within our assessment, clinical assistants operate the data collection computer and postprocess the data to generate a clinical report. Our physiotherapists note that they value the support of these assistants and that they would likely not perform the assessment if they had to operate the data collection computer themselves. 10 We recognize that this process might not be feasible in some settings with limited funding for clinical support personnel. Likewise, “research-grade” force plates may be prohibitively expensive for some clinical settings. However, the clinical implementation of instrumented assessment of balance control may become easier in the future as an inexpensive and user-friendly gaming technology is adapted for this purpose. 49
Conclusion
Observation-based balance measures may mask underlying dyscontrol after stroke. COP measures obtained from force plates may augment clinical assessment and provide information that can direct, or inform outcomes of, interventions. COP measures that reveal paretic and nonparetic lower limb contribution to balance control may be particularly promising. Future research is warranted to aid in the development of clinically friendly formats and to advance the standardization and clinical interpretation of these measures.
Author Contributions
Analyzed the data: AM. Wrote the first draft of the manuscript: AM. Contributed to the writing of the manuscript: AM and ELI. Agree with the manuscript results and conclusions: AM and ELI. Jointly developed the structure and arguments for the paper: AM and ELI. Made critical revisions and approved the final paper: AM and ELI. All authors reviewed and approved of the final manuscript.