
Abstract
Objective
The effects of TENS before exercise (TBE) and TENS after exercise (TAE) in the management of knee osteoarthritis (OA) were compared.
Methods
Fifteen participants with knee OA were alternatively assigned to either TBE or TAE groups. Participants' pain, active knee flexibility, thigh girth, disability, and activity levels were assessed at baseline and at the end of eight-week study. Mixed design two-way analysis of variance (ANOVA) at P < 0.05 was used to compare the two groups.
Results
The mean age of the participants was 58.1 ± 10.9 years. Post-intervention comparison showed that TAE had significantly lower scores (1.9 ± 0.9) than TBE (4.3 ± 1.5) on Disability Index Questionnaire (DIQ) (F-ratio = 10.5; P = 0.006), and significantly lower scores (0.8 ± 0.3) than TBE (1.4 ± 0.6) on Patient Assessment Scale (PAS) (F-ratio = 8.3; P = 0.013). However, both groups did not significantly differ on the selected impairment measures.
Conclusion
TAE was found to be more effective on the primary outcome measures in patients with knee OA.
Keywords
Introduction
Osteoarthritis (OA) is a heterogeneous group of conditions that leads to joint symptoms and signs associated with defective integrity of the underlying bone and joint margins. 1 It is characterized by joint pain, mobility impairment, and gradual wearing of joint cartilage. A previous study showed that OA is a common condition attended to in physiotherapy facilities in southwestern Nigeria, accounting for about 9% of new patients and with knee joint being the most frequently affected. 2 A study in Ghana also showed that over 60% of the adult population were affected by OA of the knee joint. 3 Joint pain and mobility impairment in OA are amenable to many non-pharmacological treatment approaches. Treatment is primarily aimed at relieving symptoms, improving joint mobility and function, and optimizing patients' quality of life. 4 Pain is the leading symptom of OA; therefore, alleviation of pain by raising its threshold in patients with knee OA is one of the main purposes of therapy.
Exercises and TENS are complementary physical means of treatment commonly prescribed by physiotherapists in the conservative management of OA. 5 Indeed, regular supervised exercise has been found to improve pain control, proprioception, strength, stability, and endurance in patients with OA.6–8 Previous studies have also shown that application of TENS thrice weekly for six consecutive weeks caused significant reduction in pain thus enabling patients to appreciably increase their active knee range of motion (ROM).9–11 Although the effects of TENS and exercise have been established in literature, the duration of post-stimulation analgesia of TENS is still a matter of debate in literature.
Through personal observations, TENS is commonly chosen by physiotherapists ahead of exercise in most clinical settings in Ghana without recourse to any scientific rationale. However, TENS effect has been described as short-lived; lasting approximately 15 minutes after its application. 12 This raises a question concerning the application of TENS before exercise (TBE) in the management of knee OA with regard to the treatment outcome. The present study was therefore aimed at comparing the effects of pre-and post-exercise TENS application on pain, active range of motion (AROM), thigh girth, and levels of activity and disability in patients with knee OA.
Participants and Methods
Design
The study used a quasi-experimental design. Fifteen patients with unilateral knee OA were alternately assigned to either TBE (n = 7) or TENS after exercise (TAE; n = 8) groups.
Participants
Seventeen participants with unilateral OA of the knee attending the out-patient units of two referral hospitals were invited to this study. Only 15 of this number were able to complete the study, while 2 dropped out because of personal reasons. Participants were eligible for enrollment if they were diagnosed with chronic knee OA (≥ 3 months) by resident physicians, had no additional joint inflammatory disease eg rheumatoid arthritis, had pain intensity of at least 4/10 on the numerical rating scale, and had no neurological condition eg stroke. Patients with defective skin sensation and open wounds around the knee, those females who were pregnant, those with cardiac pacemaker or other metallic implants, and those with bilateral presentation of knee OA were excluded from the study. Patients were instructed to adhere strictly to the study's intervention modalities while the study lasted. Advice was also given on diet and adherence to their prescribed medications.
Apparatus and Instrumentation
The TENS machine used in the study was an Enraf-Nonius Endomed 581 ID. The 11-point numerical rating scale was used to rate participant's worst pain during any activity. 13 A high score indicates more severe pain ie 0 represents no pain and the upper number 10 represents worst pain imaginable. The scale has been shown to be reliable in measuring pain perception. 14 A universal goniometer was used to measure participants' active knee ROM before and after each treatment. Muscle girth was determined with the use of tape measure. Disability Index Questionnaire (DIQ) for patients with knee OA was used to assess the level of disability of the participants. 15 It is a self-administered tool comprising five items, and each item consists of 4-point responses ranging from 0 to 3. The maximum score possible is 15 whereby high score indicates more disability. The level of activity was measured using Patient Assessment Scale (PAS). 16 The scale consists of 10 items with each item comprising 4-point response. The maximum score is 30, and a high score is indicative of more difficulty in engaging in daily activities. The total score obtained on the items are converted to a standard value provided in the questionnaire.
Procedure
Before the commencement of this study, approval was sought and obtained from the Ethics Committee of the School of Allied Health Sciences, University of Ghana. Participants gave their written, informed consent to take part in the study. On the treatment days, each patient was physically examined in supine lying position. The affected knee was palpated to localize the painful area. To rule out referred pain, participants were subjected to lower quarter screening comprising joint mobility and neurological tests. The maneuver was also meant to identify possible dysfunctions of the hip or spine that are capable of contributing to or perpetuating the symptoms at the knee.
Measurements
The patients were asked to rate their pain as normally perceived during any activity using the numerical rating scale. The active knee ROM was measured with patients in side lying and fully supported positions to ensure relaxation. The axis of the goniometer was placed at the lateral femoral epicondyle, while the stationary and mobile arms were positioned parallel to the thigh and the shank, respectively. The thigh girth of the affected lower limb was measured with participants in supine lying position and the affected lower limb positioned such that the patella faced the ceiling. The reference point for measurement was 15 cm above the base of patella. The participants also rated their activity and disability levels with respect to the knee functions on PAS and the DIQ respectively.
TENS Treatment
Patients were requested to assume the supine lying position on the plinth. Skin overlying the affected knee was cleaned with methylated spirit, and the patients were briefed about the sensation they would feel. Two electrodes were placed lateromedially on the either side of the knee and were secured in place with a Velcro strap covering the electrode to ensure even distribution of pressure, and hence the current. Conventional TENS application (low intensity and high frequency) was adopted in this study with treatment duration lasting 30 minutes per session. Each participant was treated thrice weekly for eight weeks.
Exercise Therapy
Exercises were performed in the gymnasium of the physiotherapy departments of the two selected hospitals. The exercise modes included open and close kinetic chain training. Open kinetic chain exercises were performed in both lying and standing positions, and these included AROM exercises, quadricep drills (using quadriceps chair), cycling in air, alternate leg raise with knees at 90°, and straight leg raising, whereas close kinetic chain exercises included heel lifting, leg press exercises, wall-slide, cycling, calf stretching, and gait training. Exercises were individually prescribed, and the principles of progression and overload were observed.
Both groups had 30 minutes of active exercises thrice weekly for eight weeks. At the end of the eight-week intervention, a physiotherapist who was neither part of the treatment procedure nor participants' allocation to groups performed the post-treatment outcome on the selected parameters.
Data Analysis
Data were analyzed using the SPSS package version 16.0. They were summarized using mean and standard deviation and further analyzed with paired and unpaired t-tests. Between-groups comparison was performed using mixed design two-way analysis of variance (ANOVA). The level of significance was set at α = 0.05.
Results
The study sample comprised 11 females and 4 males with age range of 40-71 years and a mean age of 58.1 ± 10.8 years. The respective baseline scores for TBE and TAE groups were 0°-88.3 ± 19.4° and 0°-78.1 ± 11.6° (ROM), 7.0 ± 1.5 and 7.6 ± 1.1 (Numerical Rating Scale), 42.0 ± 6.9 cm and 43.2 ± 5.9 cm (muscle girth), 7.8 ± 3.6 and 4.9 ± 2.3 (DIQ), and 2.4 ± 0.66 and 2.1 ± 0.9 (PAS). The groups did not differ significantly (P > 0.05) in any of the dependent variables at baseline (Table 1). The participants' scores on the outcomes at baseline and following the eight-week intervention are compared in Table 2. Both groups improved significantly on pain, level of disability, AROM, and participation level over the baseline values. The participants' muscle girths in both groups were not significantly different from the baseline values. Between-group comparisons on the outcome measures are presented in Table 3. Mixed design two-way ANOVA showed that the participants in TAE group scored significantly lower than those in TBE group after eight weeks on DIQ (1.9 ± 0.9 vs. 4.3 ± 1.5;. F-ratio = 10.5; P = 0.006) and PAS (0.8 ± 0.3 vs. 1.4 ± 0.6; F-ratio = 8.3; P = 0.013). However, both groups did not significantly differ on thigh girth, pain, and ROM.
Baseline parameters of the participants.

Paired t-test comparison, between TBEG and TAEG parameters within each group.
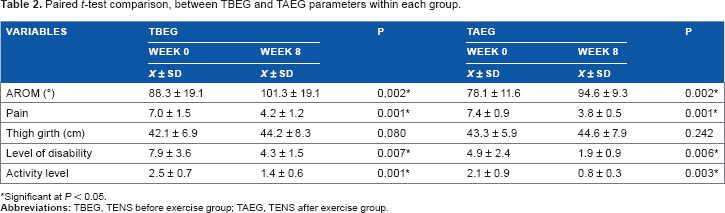
Significant at P < 0.05.
Two-way ANQVA comparison of baseline and week 8 parameters of TBE and TAE groups.
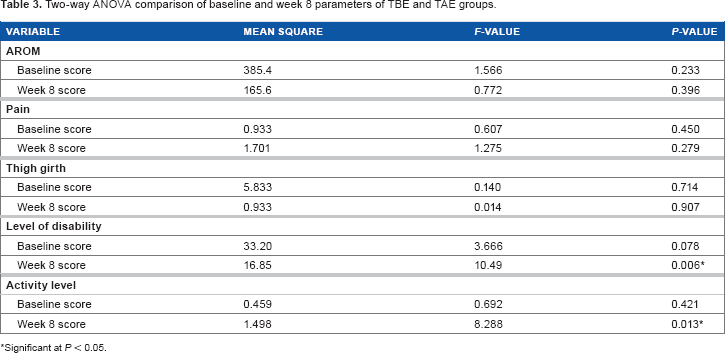
Significant at P < 0.05.
Discussion
The primary objective of this study was to compare the effects of TENS application before and after exercise on pain, active knee ROM, thigh girth, level of disability, and activity level in patients with unilateral OA of the knee joint. Our findings indicated that TAE group was significantly better than TBE group in improving self-perceived level of activity and disability level. This result implies that TAE could produce better results on functional outcome measures in the management of OA.
The results of this study also revealed that both groups experienced significant improvements over the baseline scores in their participants' pain, active knee ROM, level of disability, and activity level over the baseline scores. These findings are in agreement with those from previous studies. A significantly better improvement in gait parameters, augmented exercise performance, AROM, and pain perception had been observed among patients with OA who received TENS and exercises than those who received either modality or placebo.17–19 Exercises include any activity that enhances or maintains muscle strength, physical fitness, and overall health. The mechanism for pain reduction through exercise is diverse, and several physiological pathways have been suggested. For instance, reduction of the shock-absorbing function of muscles as well as reduction of swelling through venous and lymphatic return have been linked to higher pain threshold, although no sufficient data are available to substantiate this submission. 20 In addition, pain modulation because of exercise may be as a result of suppression of the 13-endorphin system in response to a high-intensity strengthening stimulus. 21
On the other hand, modulation of pain through the use of TENS has been reported to occur in two major ways. 22 Conventional TENS (high-frequency TENS) application could modulate pain by selectively stimulating large diameter fibers without concurrently activating small diameter fibers, thereby closing a metaphorical “pain gait” by inhibiting onward transmission of noxious information to the brain. Also, low-frequency TENS application could influence the pain-inhibitory pathway from the brain by exciting small diameter peripheral fibers, thus stimulating the release of endogenous opiates. 23 The findings from this study must have been influenced by the interplay of the physiological events from exercise and TENS applications.
In spite of the discernible physiological effects of TENS, its efficacy has been reported to vary largely by the outcome under study. 24 Previous studies that have reported the lack of effect of TENS on the knee OA pain were performed on pain at rest as the main outcome, whereas substantial evidence has revealed that TENS has a greater effect on movement-evoked pain and could subsequently result in improved function.25,26 This submission has lent support to the findings of the present study with the logical notion that TENS application is better following exercise therapy. Although therapeutic exercises have been reported to be very effective in the management of knee OA with regard to pain management, pain remains a feared effect of exercise. Indeed, even non-weight-bearing and isometric exercises could provoke pain, which might necessitate changing or redesigning the exercise programs. It is thus important that the therapeutic exercise program should not cause long-lasting pain or deterioration of functions, justifying the incorporation of other pain-relieving measures such as TENS application following the exercise program.
The major limitations of this study are the small sample size and its pilot status. The findings from this study hence need to be considered with caution. Indeed, we suspect that significant differences between the groups would have been found in other dependent variables if the sample size had been larger. Increasing the sample size and taking the study beyond the pilot stage will probably substantiate findings on the comparative effects of pre- and post-exercise TENS applications in the management of knee OA.
Conclusion
Within the limitations of this study and given the better reported effectiveness of TENS on movement-evoked pain rather than pain at rest, we concluded that post-exercise TENS application could lead to better and significant improvement in activity participation and reduction in self-perceived disability in patients with knee OA. It thus follows that clinicians should consider TAE engagement for better treatment outcome.
Author Contributions
Conceived and designed the experiments: AIB. Analyzed the data: AIB. Wrote the first draft of the manuscript: AIB. Contributed to the writing of the manuscript: BOAA, SC. Agree with manuscript results and conclusions: BOAA, SC. Jointly developed the structure and arguments for the paper: AIB, SC. Made critical revisions and approved final version: AIB, BOAA. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.