
Abstract
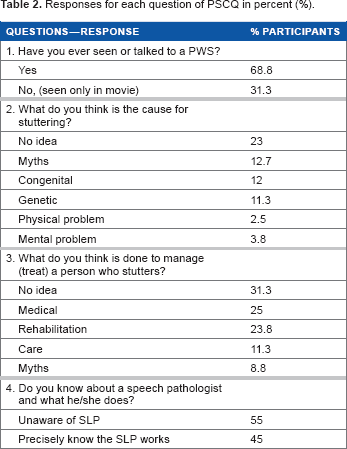
The conceptions about stuttering vary amongst cultures. Culturally specific findings regarding stuttering help in understanding the peoples' views and conceptions about stuttering and devising awareness and counselling strategies. A total of 132 passengers on the Coromandal Express from Chennai to Howrah participated in this study. All of them belonged to the upper middle socio-economic class. Preliminary Stuttering Conception Questionnaire (PSCQ) was used to understand their conceptions of stuttering. 23% had no idea and 12% had myths about the etiology of stuttering. 11% assumed it was a genetic problem and 5—6% a physical-mental problem. 31% had no idea of treatment options. 25% preferred medicine, 23% rehabilitation for treatment of stuttering. For rehabilitation, only 45% precisely knew about the speech language pathologist; the remaining 55% were unaware of this profession. Steps need to be taken towards educating the common man about stuttering.
Introduction
Stuttering is a speech disorder where the flow of speech is disrupted by involuntary repetitions and prolongations of sounds, syllables, words, or phrases as well as involuntary silent pauses or blocks during which the person who stutters (PWS) is unable to produce sounds. 1 A typical characteristic of the disorder is dysfluencies under certain speaking situations, and unexpected fluency in others. The speech organs of the PWS do not have any deformities or diseases attributable to the dys-fluency. Unpredicted variation in fluency along with no abnormalities in the oral peripheral mechanism makes stuttering mysterious, and in turn, prone to evoke speculations about its cause and treatment modalities. Moreover, older civilizations have higher variations in perceptions about the etiologies and treatment paradigms.
In India, stuttering has been documented and treated since Vedic times (5000 BC-200 BC). The texts of Ayurveda, which is the ancient system of Indian medicine contain references to medicines along with yogic practices that help PWS. 2 Even today, mothers or grandmothers recommend chewing holy basil (Tulsi), Glycyrrhiza glabra (Mulethi), black pepper (Kalimirch), and adrak (Ginger) with rock salt etc., and practicing ujjai pranayama (a type of breathing exercise) for clear and fluent speech. In addition, it is as very common for a PWS to be advised to speak with a betel nut placed under his tongue to get clear speech. In India, astrologers recommend “Panna,” a green colored stone for clear speech. 3 Thus, the underlying causes of this shadow of prejudice surrounding stuttering may include ignorance. 4 Moreover, the lack of understanding about stuttering, which could be eliminated through counseling during a speech therapy session, needs to be exposed. 4
The perceptions of society often get reflected in the unique life experiences of PWS, which is seldom integrated into the assessment and treatment of stuttering owing to relatively limited physiological research. Clinical practice does not provide a rationale or procedures for dealing with personal perspectives on meaning and meaning making.5–7 The current focus of stuttering research includes etiology, the physical process of speech, and physiology, which often reduces the PWS to more of a research subject than an individual. Further, much of our existing data reflect the experiences of PWS from the racial, ethnic, and social class of mainstream America and not the experiences of those from other backgrounds. 8 The prevalence of stuttering in India is 10% as compared to countries like Great Britain, Australia, and America, which have prevalences of 0.75-1%.9–13
The high prevalence of stuttering and the need for speech therapists in India can be felt when one comes across advertisements in local and express train compartments and toilets stating, “guaranteed cure of stuttering in 30 days.” The demand for speech treatment is on the rise as a result of the country's media revolution. Articles and programs related to stuttering appear frequently in the media. The hero of the mainstream big budget Indian film Dhoom-3 and the villain of the movie Agneepath had a stutter. Moreover, depiction of PWS to add humor, as in the movie Golmaal, indicates pervasive misperceptions about the disorder as well. Thus, stuttering has received its share of attention and perceptions about it have shaped up influenced by the media.
India is a multilingual and multicultural country. Perceptions about stuttering may vary across different linguistic and cultural backgrounds. 14 Perceptions of the Indian society are mostly directed by the literate and financially well to do upper-middle socioeconomic class (SEC). Getting the attention and time of this group is difficult as they are quite busy. However, the undivided attention of this strata of the population can possibly be accessed during their long distance train travel. The upper-middle SEC passengers usually prefer air travel or travel in an air conditioned (AC) train compartment owing to the greater travel comfort. The idea for this study arose from the observation that the majority of long distance travelers in AC compartments have ample unoccupied time as they are restricted to a place during long distance travel. Their travelling time can be used to interact with them and clarify their misperceptions about stuttering. The present study investigates the views of the upper-middle socioeconomic class about the cause and strategy needed for the management of stuttering by a speech therapist.
The present study was aimed at understanding the perceptions of people on stuttering and PWS. However, during the course of the study, 6 out of the first 10 participants suggested developing short and simple reading materials elaborating the issues pertaining to stuttering. Keeping the need for reading materials in mind, the rest of the participants were asked about the content and language in which the material should be in.
Methods
Participants
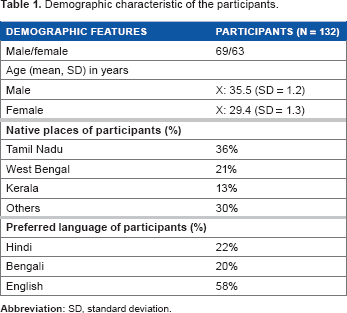
A total of 132 passengers boarding in second and third class AC compartments of the Coromandel Express train participated in this study. The train connects Chennai to Howrah and takes 27 hours for the completion of its journey. The majority of participants (122) were travelling from Chennai to Kolkata. All of them belonged to the upper-middle socioeconomic strata.
Instruments
Kuppuswamy's Socioeconomic Status Scale (KSSS)
This scale measures the socioeconomic status of families in urban communities and classifies them into upper (UP), upper-middle (UM), lower-middle (LM), upper-lower (UL), and lower (LO) socioeconomic classes. 15 Classification is based upon a composite score of education, occupation, and income per month. For instance, a person who is a post graduate (score = 7), working as a lecturer (score = 10), and with a monthly income of 38,000 rupees (score = 12) would be categorized into upper class (UP), as the composite score 29 (7 + 10 + 12) lies within the range of 26-29.
Preliminary Stuttering Perception Questionnaire (PSCQ)
PSPQ was developed by the authors for this study in Hindi, Bengali, and English. It consisted of four open-ended questions along with demographic information. The questions were:
Have you ever seen or talked to a PWS?
What do you think is the cause for stuttering?
What do you think is done to manage (treat) a PWS?
Do you know about speech pathologists and what he/she does?
The PSCQ was validated for its test-retest reliability and content validity prior to usage. Five speech-language pathologists (SLPs) well versed in English, Hindi, and Bengali were approached and the purpose of the study was briefed. They rated the questionnaire (in three languages) on a three point scale (0: unsuitable question, 1: needs modification, 2: can be included). All four questions received a rating of 2 and were included in the final checklist. After a time gap of 20 days, the questionnaire was given to 15 adults belonging to the upper-middle socioeconomic strata. The results were judged on a visual analog scale that was 5 cm long. The left end of the scale was marked as no similarity at all and right end as the most similar. Test of co-relation was done to observe the test-retest reliability. The Cronbach's alpha coefficients value for all four questions (Q1 = 0.93; Q2 = 0.82; Q3 = 0.93; Q4 = 0.82) indicated high test-retest reliability.
Procedure
Purposive sampling technique was used, which suited the purpose of study. The choice of this technique was based on a few previous travel observations and experiences from interaction with AC coach co-passengers. It was consistently observed that passengers travelling in the AC compartments were mostly literate, economically well to do, and held socially influential positions. They have ample amounts of free time during travel and are mostly ready to have conversations on varied topics. Hence, it was felt that the travel time could be used to explore their perceptions and experiences about stuttering.
The interviews were carried out by the first two authors. Both had clinical experience of more than 10 years in the field of speech-language pathology. The passengers were approached one at a time and an oral consent was obtained after briefing them about the purpose of study. The passengers, who agreed to participate and gave their consent, were interviewed in the language (Hindi, Bengali, or English) they were most comfortable with. After completing the questionnaire, a few participants shared experiences pertaining to stuttering and PWS, which was encouraged and recorded. Interviews were audio recorded using a digital voice recorder (Olympus WS-550M). At the end of each interview, opinion was taken about the need and effectiveness of using pamphlets that could highlight issues pertaining to stuttering and other disabilities on the rail.
The results were tabulated and descriptive statistics were carried out using Statistical Package for the Social Sciences (SPSS) version 16.0 software. The statistician opined that the study was qualitative and basic descriptive statistics along with percentage analysis would justify the research. In addition, multivariate analysis of variance (MANOVA) was utilized to evaluate the significance of differences in the perception of stuttering across gender and place.
Results
The results indicate that all participants had met a PWS in real life. The demographic characteristics of participants are shown in Table 1. The responses to all the four questions and their percentage values are depicted in Table 2.
Demographic characteristic of the participants.
Responses for each question of PSCQ in percent (%).
Significant effect of the native place of the questionnaire participant {F (18, 292) = 29.1, p ≤ 0.05} was found in the PSCQ responses. F and p-values of gender, native place, and their interaction on the four questions are shown in Table 3. Further, the significant effect of native place {F (18, 564) = 5.15, p = 0.02} on the awareness of a SLP's work (Q4) was observed. On comparison, native Kerala participants were found to be more aware of SLPs (p = 0.01). Since a significant interaction was found between gender and native place for Q4, each native place was analyzed separately. Male participants had significantly higher awareness than female participants among the participants from Tamil Nadu (p ≤ 0.01) and West Bengal (p = 0.02). However, among participants from Kerala, significantly equal (p > 0.05) awareness was found in both genders.
F and p-value of gender and native place of participants and their interaction on the four questions of PSCQ.

P ≤ 0.05 = significant difference.
All the participants suggested using a magazine or pamphlets on the rail to highlight issues pertaining to stuttering and other disability, as these issues are not known to the common people. However, opinions about how the matter should be presented varied on the choice of language, text, and pictograms. Table 4 shows the opinions on magazine or pamphlet content by the participants.
Opinions on language, texts, and pictograms for magazine or pamphlets.

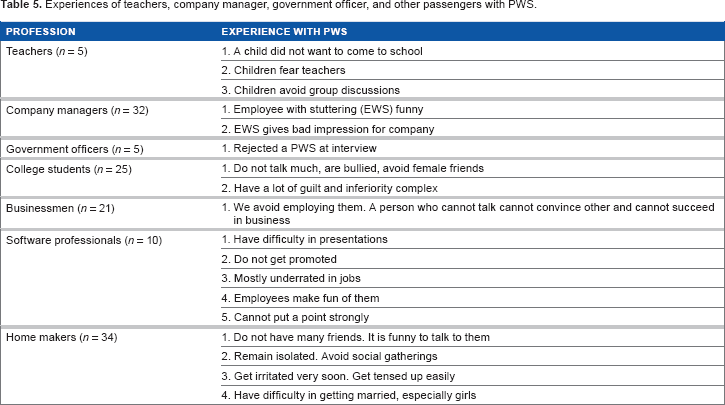
A total of 42 participants shared their life experience related to PWS. Table 5 depicts the experiences of teachers, company managers, and government officers with PWS.
Experiences of teachers, company manager, government officer, and other passengers with PWS.
Discussions
The result indicates that all participants had met a PWS in real life. Hence, stuttering is a common problem and expected to have a higher prevalence than the estimated prevalence of 10% in India. 9 Surveying data, systematic study, research, and treatment of stuttering in India began with the establishment of the All India Institute of Speech and Hearing (AIISH) in 1965. However, till date, no study has documented the incidence and prevalence of stuttering in India. 2
All participants knew about stuttering, but their perceptions about the cause and management were mostly fallacious. A few participants perceived stuttering as a problem with the speech organs, such as the tongue not rotating properly, the soft palate being short, or the tongue getting stuck to the roof of the mouth and unable to be moved properly. However, others believed forcing left handed children to use their right hand might cause stuttering in childhood. Concerning the management of stuttering, many participants suggested that weakness in speech muscles causing the stuttering could be cured by blowing a conch. However, physiological studies concerning to the involvement of the orofacial musculature has not reported any abnormal or elevated orofacial muscle activity during speech disruptions. 16 Moreover, the perception that forcing a left-hander into right-handedness can cause stuttering is certainly an over simplification of the truth. Most of the studies published since 1940 have failed to detect evidence of the switching hypotheses or increased prevalence of stuttering among left-handers.11,17,18 A few passengers felt that the recent trend of working mothers in India contributes to poor emotional development of the child leading to stuttering in early childhood. Servants and crèches are common substitutes for working mothers and this leads to the emotional needs of children being poorly addressed to. This view was reported by a working mother whose mother was also a working woman. The emotional factor contributing to stuttering has been a matter of debate. 19 However, some psychophysiological studies have found significant effects of anxiety and stress on speech dysfluencies.20–22
Other myths or fallacious perceptions on stuttering included a common belief in Odisha that, “if you kill a frog you will lose your hearing and if you make faces to tease other children or imitate a stutterer your face becomes distorted and you cannot speak.” These types of myths about the causes of stuttering were also reported in many other countries. African population believes that stuttering occurs if a baby is left out in the rain, on failure to inform the ancestors of imminent childbirth, from emotional trauma, and tickling a baby too much. 23 A few of the etiological myths prevalent among African Americans are that stuttering can be caused by a mother having an improper food while breast feeding an infant, allowing an infant to look in the mirror, cutting a child's hair before he/she says his/her first word, a mother looking at a snake during pregnancy, a mother dropping a baby, a child being bitten by a dog, and the work of the devil. 24 Some participants also believed that disabilities are the results of past life deeds (karma) of the child or its parents.
About 8.8% of the participants quoted myths attributed to effective stuttering treatment. For example, reading aloud to a mirror, wearing a shank (a type of sea shell) as a ring, placing a pebble under the tongue when the child is asleep so as to cut the attachment of the tongue to the lower jaw and free it, and placing a betel nut in the mouth while speaking. One participant attributed the clear and confident speech of a child to its mother. If the mother does not spend time to teach the child speech, then it will have erroneous speech. It was reported that, in speech therapy, a client's belief systems are related to the condition being treated. 25 Hence, speech-therapists working with PWS should be culturally sensitive. 26 If a family views stuttering as a curse or a God given condition, the treatment will need to account for such beliefs. Otherwise, clinicians inadvertently could challenge clients to decide between clinician's advice and personal beliefs.
Six passengers classified stuttering into two types. The first type is children who stutter right from birth or the day they start speaking, while the other group comprises those who become stutterers after a mental or emotional shock. They quoted two instances from their family and neighborhood to elaborate the second cause. A couple narrated an incidence of twin children who were very attached to each other. Until the age of nine years, both had unmarked development in physical, emotional, and language domains. Then, one of the brothers fell ill and expired. The incident changed the personality of the other brother; he started to stammer and became an introvert. Another passenger narrated about a nine year old normally developing girl, who went to the hospital with her parents to visit her severely ailing grandmother. There was a sudden, brief power failure, which resumed in five minutes. As the power resumed, the doctors who were on rounds declared the old woman to be dead. The girl reportedly developed stuttering after the instance. Although, the role of the environment in the onset and evolution of stuttering symptoms continues to generate debate, 27 a study reported that a stressful situation like the birth of a sibling or death of loved one might trigger stuttering. 28 A study focusing on college students conducted by the University of Minnesota Duluth, found that a large majority viewed the cause of stuttering as either nervousness or low self-confidence, and many recommended “slowing down” as the best course of action for recovery. 29 Studies also emphasized the possible role of parental attitudes and behavior in shaping stuttering tendencies in childhood.30–33
Genetics and neurophysiology were reported as the cause for stuttering by 11.3% of participants. There is strong evidence for a genetic basis of stuttering. 28 Three genes have been found to be correlated with stuttering including GNPTAB, GNPTG, and NAGPA. Alterations in these three genes were present in 9% of the PWS with a family history of stuttering. 34
The majority of the passengers (31%) had no idea about treatment. However, 25% were of the view that medicines could be a treatment option. Comprehensive reviews of all the drug trials for adults and children in 2006 indicated that only a few drug trials were methodologically sound. 35 Only one was found to be reliable in decreasing stuttering down to less than 5% along with potential side effects such as weight gain and increase in blood pressure. A passenger who had completed his doctorate in medicine and was a practitioner in a tertiary health care center felt sorry for PWS. He opined that stutterers have an “unclassified” problem. They can neither be cured by medicines nor are they considered ill/disabled. Stuttering emerges in the situations where communication skills ought to have been at their best (interviews, serious discussions, and communications under time pressures). Poor communication and lack of awareness leads a PWS to be underrated, personally, socially, and vocationally. The entire crowd in a cinema theater breaks into loud laughter as a stutterer struggles to speak. It is sad that the plight of a stutterer (which is never honestly depicted) is used to add humor in movies, which is carried forward to the real word. People working for PWS should file a public interest litigation against filmmakers to avoid such misleading on screen depictions. At least a caution notice as those shown while depicting a smoker or using animals on screen, “Smoking Kills,” “No animals have been treated inhumanly or have been harmed,” should be displayed while depicting a stutterer on screen in any form.
As many as 24% of the participants recognized the need for rehabilitative treatment for PWS. However, they were unaware of the professionals to be approached for stuttering. Only eight passengers reported that stuttering is treated by a SLP. The lack of awareness is in part because of the limited number of colleges offering speech therapy courses. Approximately 25 speech and hearing colleges offer diploma, bachelor, and master level courses in India. 36 More than 5000-6000 professionals have graduated from these colleges since 1966. However, in the recent years, increasing global demand for SLPs resulted in a major drain of skilled SLPs from India to other countries. Therefore, there seems to be a shortage of qualified and skilled SLPs in India. A study reported that only 700 registered SLPs are available in India. 37 Hence, on an average, there would be one speech therapist per every 1,522,089 Indians, putting forth a need for more graduate colleges to be established. The majority (as many as 70%) of the post graduates migrate to USA, Canada, Australia, or Middle Eastern countries, creating a void and adding an economic burden on the country. The total number of seats for the post graduate colleges can be restricted so as to ensure quality control and warrant the availability of speech therapist in India.
Amongst the three states from which participants were included in the study, participants from Kerala were significantly more aware of SLPs. This might be because of the maximum number of speech and hearing colleges in Kerala (seven colleges) as compared to the other two states (Tamil Nadu, five; West Bengal, one). 38 This is partly a result of the highest literacy level in Kerala (93.91%) as compared to Tamil Nadu (80.3%) and West Bengal (77.1%). 39
About 11.3% of the passengers who had met children with stuttering had asked the child to slow down his rate of speech and advised him not to worry about stuttering while speaking. The study suggested that if a child is interrupted every time he speaks, it will lead to dysfluencies. 40 It is always advisable to consult a SLP for stuttering therapy rather than trying out different techniques, which might deteriorate stuttering. Presently, behavioral oriented approaches (BOA) are preferred for the treatment of stuttering. They have been proved to be effective in controlled studies as well. 41 Two major schools of thoughts among BOA include the Van Riper school of thought and the school of thought followed by Perkins and Hedge, who proposed stuttering modification therapy (STM) and fluency shaping techniques (FST), respectively.41,42 SMT not only eliminates stuttering but also modifies it, so that stuttering is easier and less effortful. 33 A PWS should be permitted to stutter fluently without fear, anxiety, or avoidance. SMT focuses on the removal of negative emotion that actually reinforces stuttering. However, FST targets the stuttering behavior. The focus is on reducing stuttering through different techniques like airflow modification, gentle phonatory onset, and rate reduction by syllable-to-syllable prolongation techniques to reduce the dysfluencies and improve fluent speech. These techniques have been found to be effective in reducing dysfluencies. 41
The above discussed findings are mostly from the upper-middle socioeconomic strata, mostly belonging to 3 out of 35 states of India. However, an estimated 22% of Indians are living below the national poverty line, 63% are in the middle socioeconomic strata and the remaining approximately 15% belong to the upper socioeconomic strata. 43 In addition to 23 official languages and 1661 mother tongues, the 2800 religions followed in the country show huge linguistic and cultural diversity.44,45 Hence for representative data, cohorts keeping in view the variables need to be made.
Conclusion
Stuttering is a common problem that seems to be on the rise as every passenger who was approached had met a PWS. However the awareness about etiology and management of stuttering is poor even amongst the upper-middle socioeconomic class of India, which is of concern. Travel time may be an effective medium to create awareness and educate people about stuttering and PWSs using pamphlets.
Author Contributions
Conceived and designed the experiments: NR, SK, NK. Analyzed the data: NK. Wrote the first draft of the manuscript: NK. Contributed to the writing of the manuscript: NR, SK. Agree with manuscript results and conclusions: NR, SK, NK. Jointly developed the structure and arguments for the paper: NR, SK, NK. Made critical revisions and approved final version: NR, SK, NK. All authors reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.