
Abstract
Aims
Response of single agent chemotherapy in improving quality of life in patients with recurrent head and neck cancers.
Methods and material
This is a study of the 18 patients with advanced cancers of head and neck, who had failed earlier attempts of radical treatment with Surgery, Radiotherapy ± chemotherapy and have residual or recurrent tumours, were treated with single agent Injection Methotrexate 50 mg/m2 weekly. Follow up visit complaints and clinical examination details were recorded. History regarding pain, speech and diet was collected for every visit. Severity of pain was divided with the National Cancer Institute's Common Terminology Criteria for Adverse Events (CTCAE) version 3.0 pain scales. Symptom control was done with analgesics, antiemetic and infection control.
Results
Weekly single agent chemotherapy with injection Methotrexate has significantly improved the quality of life of patients. 38.8% of patients have shown good response with decrease in the tumour bulk by more than 50% and other 39% of patients have stable disease on Injection Methotrexate. 22.2% patients have shown disease progression on single agent chemotherapy. Overall 83.3% patients have shown improvement in Quality of life in terms of symptomatic control. After 6 weekly treatments with injection methotrexate 63% patients were pain free with 16% patients reported decrease in pain. 87.5% of patients have shown improvement in speech and diet. Improvement in symptoms has shown decrease in depression in cancer patients. Grade 3 toxicity observed was Neutropenia (11.1%), anaemia (11.1%) and Mucositis (16.6%) which was managed adequately. Median survival with good quality of life is 5.4 months.
Conclusions
Single agent methotrexate chemotherapy on an out-patient basis can provide good quality of life. Decrease in pain along with improvement in speech and diet has shown decrease in incidence of depression and overall positive impact on psychosocial status. Few cases have shown sustained regression of gross disease adding to maintained quality of life with better socio-economic compliance.
Introduction
Head and neck cancers are a select group of uncommon and diverse malignancies that can be characterized by their pattern of spread and recurrence. Cancer of the oral cavity, pharynx and larynx comprise 5% of all malignancies worldwide. The most common primary site is the oral cavity. In 2002, there were estimated to be more than 500,000 new cases of head and neck cancers worldwide and 300,000 deaths. Approximately 95% of these tumours are squamous cell carcinomas arising primarily from the lip/oral cavity, Oropharynx, hypopharynx, and larynx. Other less common cancers include mucoepidermoid carcinomas, adenoid cystic carcinomas, and adenocarcinomas, originating from the salivary glands. The main causes of treatment failure are locoregional recurrences and metastatic disease. 1
Despite intensification of single or combined modality treatment aimed at achieving higher locoregional control in head and neck cancers, more than half of the patients with locally advanced tumours developed loco regional recurrence.2–4 For those who did not develop loco-regional or distant recurrence there is still a risk of 25% at 5 years to develop a second primary head and neck cancers. 5
Although these response rates are clinically significant, it is also important to remember that systemic therapy has not been adequately demonstrated to improve OS, and its role in therapy continues to be a palliative one with the goal of controlling symptoms and improving quality of life.6,7 This distinction is important to recognize in the selection of patients for treatment, with consideration given to treatment toxicity and tolerability. 6
Subjects and Methods
This is a study of the 18 patients who have residual or recurrent disease of Head and Neck, after failed earlier attempts of radical treatment with Surgery, Radiotherapy ± chemotherapy. Complete history and physical examination of patients was done. Complete local examination of head and neck areas was done to see the local extent of the disease. Direct laryngoscopy was done for the local extension and characteristics of disease as required. Complete history and treatment details were collected and recorded for each patient. Symptoms of pain, change in voice, speech and difficulty in swallowing were recorded. Pain was rated with the National Cancer Institute's Common Terminology Criteria for Adverse Events (CTCAE) version 3.0 pain scale: 0) no pain; 1) mild pain not interfering with function; 2) pain or analgesics interfering with function but not with activities of daily life; 3) severe pain, pain or analgesics severely interfering with activities of daily life; or 4) disabling pain. 8 Chest X-ray and ultrasonography of abdomen were done to assess the presence of metastasis to lung and liver respectively. Accordingly patients were classified as local recurrence or metastatic disease. Consent of patients was taken for the treatment with single agent palliative chemotherapy with injection Methotrexate. All the effects and adverse effects of the drug were discussed with the patients before starting the chemotherapy. Patients having residual disease or local recurrence were planned for the palliative chemotherapy with single agent injection Methotrexate 50 mg weekly. Before giving every infusion of single agent chemotherapy complete physical examination and complete blood counts were done. Two patients were started on upfront injectable Methotrexate due to economic reasons. Follow up visit complaints and clinical examination details were collected and recorded. History regarding pain, speech and diet was collected for every visit. Management given in the form of analgesics, antiemetic and infection control was also recorded.
Results
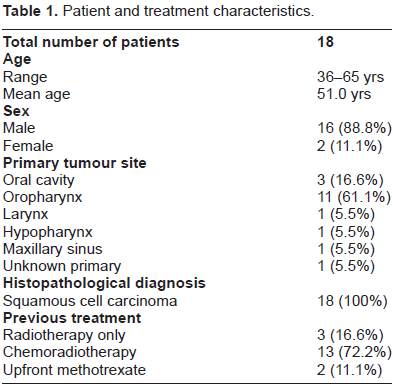
Majority of patients (88.8%) were in 5th to 7th decade of life. Present study has 88.8% males and 11.1% females. 83% were smokers. Oropharynx was the primary in 61.1% patients followed by oral cavity (16.6%). One case each of Maxillary sinus, larynx and hypopharynx were in the study. One (5.5%) was diagnosed as unknown primary. All patients have squamous cell carcinoma, with 50% patients having poorly differentiated grading (Table 1). Average Radiation dose received is 60Gy. Out of 18 patients, eleven presented with recurrent disease, five were having residual disease after primary treatment. Two patients were started on upfront chemotherapy with methotrexate because of economic reasons. Two (11.1%) patients experienced anaemia and only two (11.1%) patients developed Neutropenia which was managed adequately with supportive care and management. Mucositis was seen in three (16.6%) patients only (Graph 1).
Patient and treatment characteristics.
Partial response with more than 50% reduction in tumour mass was recorded in eight (44.4%) patients. Six (33.3%) patients have stable disease and Progressive disease was seen in four (22.2%) patients (Graph 2). Median survival of 5.4 months was seen in patients started on methotrexate as salvage therapy. Symptomatic improvement in concern to pain, speech and diet was seen in 72.3% of patients.
Discussion
The management of recurrent and second primary head and neck cancers in the previously irradiated has been limited to salvage surgery in selected patients resulting in a 2-year disease free survival of 36% (range 23%–55%). 9 Up to 55% of the patients developed second recurrences after salvage surgery. 10

Treatment adverse effects.

Treatment response.
Salvage surgery as well as brachytherapy or stereotactic radiosurgery is limited by tumour size, location and/or co-morbidity. In the inoperable patients and non-resectable tumours, chemotherapy alone is considered a standard treatment 11 despite the poor response rates of 10%–40% and median survival rates not exceeding six months. 12 The role of external re-irradiation was rarely investigated mainly due to fear of severe toxicity from high doses to large, previously irradiated target volumes. 13
Since many patients with these tumours are heavily pre-treated, their physical condition is poor and their tolerance of standard doses of chemotherapeutic agents is reduced. 14 Patients with head and neck cancers face difficulties in eating, chewing, drinking, breathing, speaking, as well as changes in appearance. Simultaneously, the burden of head and neck cancers is often manifested in psychosocial dysfunction, which can have a negative impact on quality of life. Although a phenomenon well recognized, little is known about many factors that influence or impact psychosocial dysfunction in individuals with head and neck cancers. Even less is known about the effective management of psychosocial dysfunction. 15 Palliative therapy with systemic therapy includes conventional chemotherapy and novel targeted therapy. Response rates with these therapies are variable, with several phase II-III clinical trials showing overall response rates to combination chemotherapy in the order of 20%–40% and single agent therapy, including non-cytotoxic, in the order of 5%–15%.6,7
Patients with advanced head and neck cancers resistant to platinum-based chemotherapy have a very poor prognosis, with a low response rate and short survival. 16 The purpose of chemotherapy in these patients is to control potential symptoms, prevent serious complications, increase survival, and improve quality of life. It is very important to provide a treatment that can be well tolerated, affordable and has few toxic effects. Combination chemotherapy has demonstrated the highest response rates in systemic therapy for recurrent and metastatic squamous cell carcinoma of head and neck, and is currently the standard of care. Several phase II–III studies comparing combination chemotherapy versus single-agent therapy have shown statistically significant improvement in tumour response with combination chemotherapy over single-agent therapy.6,17 Single agent chemotherapy is currently recommended in cases in which prior combination chemotherapy has failed and toxicity is of concern.6,18
Although combination chemotherapy has been shown to have higher response rates than single-agent therapy, the incidence of high-grade toxicity is significantly higher. A phase II trial of a Paclitaxel-Carboplatin combination in recurrent squamous cell carcinoma of Head and Neck Cancer has shown grade 3–4 toxicities with Neutropenia (62.9%), anaemia (11.1%) and 7.4% Mucositis. 19 The incidence of toxicities with single agent palliative methotrexate chemotherapy in present study is Neutropenia (11.1%), anaemia (11.1%) and Mucositis (16.6%). This study has seen higher incidence in toxicity with Mucositis which was managed adequately.
Other agents currently used in the treatment of squamous cell carcinoma of head and neck include the platinum agents (cisplatin and carboplatin), the taxanes (paclitaxel and docetaxel), 5-FU, capecitabine, gemcitabine, pemetrexed, as well as bleomycin which were both the most widely used cytotoxic agents before the advent of the platinum agents.6,18
In cases of localised recurrence, for most patients palliative chemotherapy is the standard option. Although combination chemotherapy (Cisplatinum, 5-Flourouracil or taxanes) produces higher response rates and may show a better progression-free survival than single agent methotrexate, no overall survival benefit has been demonstrated [II,B]. 20 Weekly methotrexate may be considered as the accepted treatment [I,B]. Weekly methotrexate therapy is well tolerable, affordable and given on Outpatient basis.
The standard dose and schedule for palliation are 40 mg/m2/wk intravenously or intramuscularly, with dose escalations to 60 mg/m2/wk until mild toxicity or any tumour response is achieved. This methotrexate dose and schedule are relatively nontoxic, inexpensive, and convenient, features that are critical to palliative therapy.
Conclusions
Single agent methotrexate chemotherapy in recurrent head and neck carcinoma can provide good quality of life on an out-patient basis. Decrease in pain along with improvement in speech and diet has shown decrease in incidence of depression. Symptom control has shown an overall positive impact on psychosocial status. Sustained regression of gross disease adding to maintained quality of life with better socio-economic compliance can be achieved with single agent methotrexate chemotherapy, which is relatively less toxic, inexpensive and convenient to administer.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.