
Abstract
Background
Data from the core data set of the Hospice and Palliative Care Evaluation (HOPE) from 1999 to 2001 demonstrated considerable variance in the incidence of patients’ symptoms and problems between participating services. This paper aims to investigate these differences more closely.
Methods
During the evaluation period of HOPE in 2002 a telephone survey with a representative of each participating unit was performed. Telephone interviews assessed the professionals’ definitions of selected symptoms and estimates of problem and symptom incidences. Content analysis was used to evaluate qualitative answers.
Results
Staff members rated pain, weakness, nausea/emesis as the most frequent physical symptoms; anxiety, depression and amentia as most frequent psychological symptoms; wound treatment, mobilisation and weakness as nursing problems and organisation of care settings, loneliness, demands of relatives the most common social needs. Staff members used a wide range of definitions for cachexia, weakness and depression.
Discussion
Standard definitions of symptoms and problems were lacking in the articulation of subjective staff members’ perspectives. Meaningful evaluation of multicentre surveys would require training in symptom assessment and classification in order to produce a common basis for documentation. Even though definitions differed widely, underlying concepts seemed to be compatible.
Introduction
Although key concepts are described in definitions of palliative care (PC), there is still a lack of widely accepted and suitable indicators and outcome parameters of the quality of PC treatment.1,2 There is general agreement that the continuous documentation of symptom incidence and intensity is necessary for monitoring and evaluation of the effectiveness of the care provided. Therefore standardised assessment tools like the Edmonton Symptom Assessment System (ESAS) or the Karnofsky Performance Status (KPS) were developed and implemented. Hence, caregivers are challenged to estimate patients’ symptoms precisely for maximising the accordance to the self-estimation of patients.3,4 In addition caregivers have to use assessment batteries with a comparable understanding of underlying PC concepts. In consequence, standard documentation systems have to be validated to demonstrate whether they are useful for the evaluation of effectiveness eg, for quality assurances. However, the selection of quality indicators and best practice for benchmarking is still under discussion. 5
In 1996, following a remit from the German Ministry of Health, a work group of experts developed a standard core data set for the use in the palliative care units (PCU). The resulting Hospice- and Palliative Care Evaluation (HOPE) was tested in yearly census surveys in 1999 and 2000. HOPE assesses personal data on patients, social situation, state of disease, individual symptom burden, current medication and other therapeutic interventions, as well as information on outcome such as place of death. The instrument was revised following each evaluation period.6,7 The census surveys managed to include more than half of the existing PCUs in Germany, producing representative results for inpatient PC in the country. Comparable standard assessment tools on symptoms8,9 or quality of life10,11 were implemented nationally or internationally to standardize terminology for better clinical care and to assist in clinical trails data collection.
An evaluation of multi centre or nationwide surveys assumes a homogenous understanding and unique use of the documentation system. However, there has been no systematic evaluation of staff members’ definition of the underlying concepts and definitions used for this documentation system. The results of the evaluations in 1999–2001 showed major differences in the incidences of symptoms and problems of PC patients. For example PCUs affiliated to anaesthesiology report that 38.7% of their patients suffer from cachexia, but this is reported in significantly less patients (30.8%) in PCUs affiliated to internal medicine. 12 Similar significant differences were found for nursing and social problems, oedema and sleeping disorders 12 and might be related to either different catchment areas and populations or related to differences in staff members’ attitudes and perceptions. While the incidence of pain was 39.1% for patients from oncological units, the incidence of this symptom ranged from 49% in some units to 78.5% in others. Similarly, the incidence of weakness for patients from geriatric units was 81.6%, but ranged from 52.7% to 96.6% in the individual palliative care units. For anxiety the incidence ranged from 20% to 69.4%. 13 In consequence, it became necessary to investigate the understanding of the underlying concepts and definitions of common symptoms and problems assessed in PC.
This paper presents results on a) staff members’ main issues working with PC patients, b) their estimates of the incidence of problems and symptoms of PC patients and c) their subjective definitions of selected symptoms (cachexia, weakness, depression) to explain differences in documented incidences with conceptual differences in the understanding of these items. These symptoms had been selected because feedback from the participants in previous HOPE evaluations had demonstrated low levels of consensus for the definition and epidemiology of these symptoms.
Methods
Telephone survey
For the yearly nationwide survey with HOPE from October to December 2002 hospice and PC service registered in the German hospice directory were invited to participate in the evaluation. Each participating service identified one representative who performed a telephone interview that was done two to six months after the initiation of the evaluation period. The interview guide was mailed to the representatives prior to the call to allow for written responses for those participants who preferred that option. The structured interviews were performed and documented by one of the authors (CH), who had received interview training before the survey. Written responses were collected and analysed in the same manner as telephone answers.
The questionnaire asked for the five most frequent and important problems and therapies in PC, as well as for participants’ definitions of the symptoms weakness, cachexia and depression and estimated incidences in PC in general and the interviewees unit specifically.
Setting
The core documentation for HOPE and the telephone interviews did not lead to additional work for the health care professionals or changes in the PC provided to patients. Documentation for HOPE in the survey did not exceed what would be required for good clinical practice. All data were analysed anonymously. Informed consent of patients was not obtained, but the HOPE survey provided an information brochure on the background and outline of the project for patients and relatives.
The project was not submitted to an ethics committee as the HOPE census survey was performed as a quality assurance project. The telephone survey did not involve patient data. Thus ethics committee approval was not required following usual standards in Germany. Ethical implications of the data documentation and evaluation as well as from the telephone survey were discussed in detail among authors and in the HOPE Steering Group.
The study was funded by the Department of Palliative Medicine, RWTH Aachen University.
Data analysis
Statistical analysis (descriptive data) of quantitative answers was carried out with SPSS 16.0 for Windows. Free text answers to open interview questions and subjective definitions were analysed qualitatively using content analysis. 14 Respondents’ definitions of weakness, cachexia and depression were collected and summarised in sub and major categories based on similar content independent from gold standard definitions.
Results
Study population and demographic data
Representatives from 71 of the 74 participating units (57 PCUs, 4 oncology units, 2 geriatric units, 8 hospices) responded to the telephone interview. The majority (61 units) answered the questionnaire by phone, the others by mail.
Most interviewees were physicians (N = 58) except for 9 nurses, 3 psychologists and one social worker. Almost half of them worked in PC for 3–6 years (44%) and had been in the current place of care for the same time (47%). The attitude of hospital staff towards the PCU (N = 57) was rated very good (19%), good (41%), satisfactory (21%) and unsatisfactory (19%). Explanations provided for low levels of acceptance were: “stigma as terminal ward”, “accepted only as existing” and “some kind of hospice”.
Ranking of symptoms and problems
The professionals’ ranked the most frequent physical problems of patients receiving PC as reduced energy and performance status, gastrointestinal suffering, respiratory symptoms and pain, followed by psychological problems (emotions, changes of personality, coping with the disease, psychosomatic symptoms), nursing issues (symptom control, nursing activities, organisational problems) and social problems (experiences of the patient, surrounding, organisational problems, interaction).
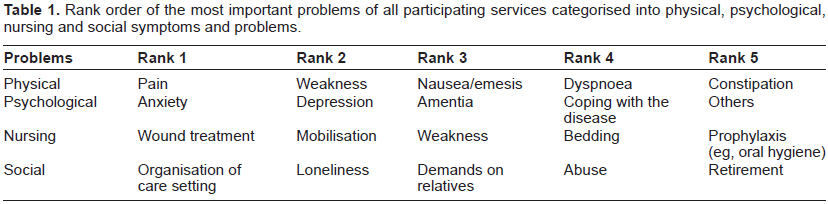
In contrast, the most important physical problems of patients receiving PC are pain, weakness, nausea/emesis and constipation; psychological problems: anxiety, depression, amentia, coping with disease; nursing issues: wound treatment, mobilisation, weakness, bedding and prophylaxis and social: organisation of care planning, loneliness, demands of relatives, abuse and retirement (see Table 1).
Rank order of the most important problems of all participating services categorised into physical, psychological, nursing and social symptoms and problems.
Definitions
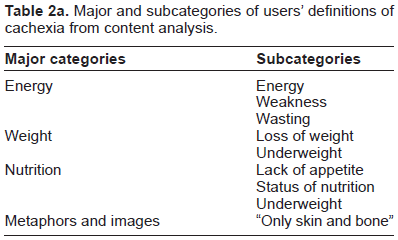
More than 80% of the representatives of PCUs estimated the percentage of patients with cachexia higher than 50% and found cachexia an important and frequent problem in PC. The wide range of definitions of cachexia provided by the interviewees was related to energy status, weight and nutrition. Other definitions were characterised by the use of metaphors and images. Only some participants used quantitative data such as percentages of weight loss per time for the definition of cachexia (see Table 2a).
Major and subcategories of users’ definitions of cachexia from content analysis.
Similarly, a range of definitions were documented for depression, covering concepts of introversion, listlessness, negative emotions, somatic disorders as well as official definitions or test scores (see Table 2b). Except for one hospice, all units estimated the percentage of PC patients with depression at less than 50%. In contrast the percentage of patients with depressive moods in their own unit was estimated to be higher than 50% by half of the PCUs, as well as in one oncology and one geriatric unit and two hospices.
Major and subcategories of users’ definitions of depression from content analysis.

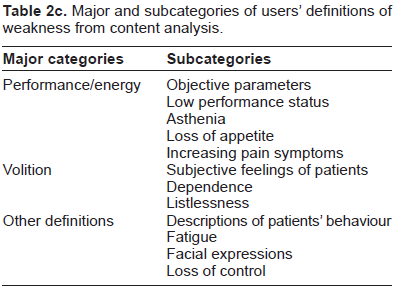
The majority of all PCUs (90%) estimated that 50% of patients suffer from weakness, whereas all other units except for one oncology unit estimated a percentage of more than 70% of their patients to be affected by weakness. Definitions of weakness involved: performance/energy, volition and other definitions. Subcategories of all definitions are listed in Table 2c.
Major and subcategories of users’ definitions of weakness from content analysis.
Discussion
From previous evaluations of HOPE we had presumed that differences in individual attitudes, definitions and perceptions of staff members might influence the assessment and documentation of problems and symptoms, ranking, incidence and intensity. Results of this study confirmed this hypothesis, but also offered new insights into the value of different articulations of symptoms provided that these are based on compatible understandings of underlying concepts.
Differences in assessment can be explained by different care settings, needs and diseases of patient groups to some degree. For example, the dominant problem of PCUs, geriatrics and oncology units was the organisation of home care for patients about to get discharged. In comparison, hospices did not report this as a problem at all, because in Germany patients usually are transferred to hospice if home care is not possible, and are cared for in the hospice until the time of death. Oncology units prioritized curative treatment (radiotherapy, chemo therapy, surgical neoplasm excision) and PCUs primarily aimed for symptom relief. There was only little overlap in the ranking between settings, and none of the interventions preferred by oncology units was included in the top five interventions of PCUs, although PC does not exclude these treatment options on principle. 15 Whereas oncology units (92%), PCUs (94%) and hospices cared for cancer patients, only a minority of geriatric patients suffered from cancer (8%). The large percentage of patients with non-cancer diseases in geriatrics implies different problems and therapies, 13 such as the use of logopaedia and occupational therapy which were ranked as important only in geriatrics.
In order to explore differences in symptom epidemiology between services that had been described in earlier evaluations of HOPE, concepts and definitions of selected key symptoms were evaluated in telephone interviews. The range of definitions provided by the interviewees was wide, including vastly different examples. Only rarely regular definitions as predetermined by diagnostic codes or guidelines were produced.
On the one hand, a common understanding of the selected symptoms was hard to find in this survey because some respondents presented formal definitions while other respondents used metaphors to explain the same phenomenon. 16 It remains unclear which of these ways of understanding patient symptoms is more efficient in clinical practice. Metaphors and clinical classifications and definitions may even relate to the same underlying concepts, and a pluralistic approach to symptom assessment may be more suitable for the patient to communicate his/her symptoms to the PC care team.
A lot of uncertainty was reported for the definition of depression in PC patients. Differentiation between depressive mood in reaction to the malignant disease and pathological major depression as a comorbidity seemed difficult. 17 A standard definition of depression has been provided by the World Health Organisation: “… a common mental disorder that presents with depressed mood, loss of interest or pleasure, feelings of guilt or low self-worth, disturbed sleep or appetite, low energy, and poor concentration”. 18 Depressive mood in PC patients is often associated with other cancer-related symptoms such as fatigue, low energy, loss of appetite and loss of interest. Breitbart (1993) recommended a flexible approach, excluding physical symptoms in the diagnosis of depression if they are probably due to physical disease or its treatment but including them if they are more likely to be part of the depressive symptomatology. 19 This dilemma of definition and diagnosis burdens the assessment and evaluation of depression as different concepts will lead to differences in the epidemiology. Under-assessment and undertreatment of depressive moods have been reported as a major problem in PC. 17
The biggest variability of definitions was found for the symptom weakness. Whereas the category performance/energy described parameters that can be evaluated and measured objectively by the observer, the category volition summarises subjective aspects of the individual feeling and perception of patients.
Cachexia was often defined by metaphoric associations and other symptomatic descriptions which underlined that cachexia raises feelings of helplessness in staff members and leads to a feeling of poor prognosis and low quality of life in patients.20,21 Only rarely definitions close to the literature such as “an involuntary weight loss of more than 10 per cent from premorbid weight, associated with loss of muscle and visceral protein and lipolysis” 22 were provided by the interviewees. The higher frequency of cachexia in patients from PCUs and hospices than in oncology and geriatric units corresponds with clinical data, as cachexia is found in 24% of cancer patients in early stages of the disease and in 80% of patients in advanced stages of disease who are more often treated in PCUs or hospices.23,24
All the descriptive and explanatory words such as energy status, weight and nutrition appear plausible as content for the concept “cachexia” and these words are in line with the respondents’ descriptions with the metaphor “only skin and bone” so that the understanding of the phenomenon might be compatible although the articulation is widely different and does not correspond to the terminology in guidelines or standard definitions.
The study is limited by the evaluation of only one representative of each institution which might rather mirror an individual perspective but not team attitudes. Only few nurses were interviewed and this might not accurately represent the group of professionals that care for PC patients.
Differences in definition, assessment and documentation might be less relevant if documentation were a team effort rather than a task delegated to one team member. In clinical practice assessment usually is performed by one person only, but multiple perspectives and subjective definitions could rather support a more holistic estimate of professionals in PC. In an ideal setting, the whole team would be involved in the documentation process, but this does not seem feasible in many services due to high workload.
However, performing routine assessment with a standardized documentation system facilitates communication of staff members on care planning. Finally it can be used to evaluate differences in patient's symptom load, no matter what the underlying concepts of staff members are.
Conclusion
Standard definitions of symptoms and problems were lacking in the articulation of subjective staff members’ perspectives in this survey. Nevertheless a common understanding of major concepts has to be secured for a consistent use of documentation systems for quality assurance in PC.
Therefore specific training in symptom assessment and classification might be an option to further strengthen demands of the documentation systems and lead to a comparable use of the documentation system of participating institutions. This standardisation could provide symptom assessment independent from subjective definitions and preferences in articulation of symptoms; however, even though the description of symptoms differed widely, the underlying concepts might be similar. If caregivers in clinic practice accept and perform pluralism as an approach to assess the patient's symptoms, this could provide new insight into the patient's way of communicating symptoms.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.