
Abstract
Background
Hypertensive crisis (HC) is a common medical emergency associated with acute rise in arterial blood pressure that leads to end-organ damage (EOD). Therefore, it is imperative to find markers that may help in the prediction of EOD in acute hypertensive crisis.
Aim
To assess the clinical presentations on admission; echocardiographic changes of pulsed and tissue Doppler changes in EOD patients compared with no EOD; and the risk of developing end organ damage for clinical and biochemical variables in hypertension crisis.
Material and Methods
The data of 241 patients with hypertensive crisis with systolic blood pressure (SBP) of >180 mmHg or diastolic blood pressure (DBP) >120 mmHg were extracted from patients files. Patients divided into hypertensive emergency (HE) with EOD, n = 62 and hypertensive urgency (HU) without EOD, n = 179. LV hypertrophy on ECG, echo parameters for wall thickness, left Ventricular mass index (LVMI), Body mass index (BMI), pulse Doppler ratio of early filling velocity E wave to late A wave (E/A) and ratio of E wave velocity to tissue Doppler Em to E wave (E/Em) were evaluated. Serum creatinine, hemoglobin, age, gender, body mass Index (BMI), history of diabetes mellitus, smoking, hypertension, stroke and hyperlipidemia were recorded. Multiple logistic regression analysis was applied for risk prediction of end organ damage of clinical variables.
Results
Patients with HE compared with HU were significantly older, with a significantly higher SBP on admission, high BMI and LVMI. Further there were significantly higher E/A ratio on Doppler echo and higher E/Em ratio on tissue Doppler echocardiogram. Multiple regression analysis with adjustment for age and sex shows positive predictive value with odds ratio of SBP on admission >220 mmHg of 1.98, serum creatinine > 120 µg/L of 1.43, older age > 60 year of 1.304, obesity (BMI ≥ 30) of 1.9, male gender of 2.26 and left ventricle hypertrophy on ECG of 1.92. The hemoglobin level, history of smoking, hyperlipidemia and DM were with no significant predictive value. The pulsed Doppler E/A ratio was ≥1.6, E/Em > 15, LVMI > 125 gm/m2 in patients with EOD compared with those without.
Conclusion
In patients presented with hypertensive crisis, the echo indices of E/A ratio and E/Em ratio of tissue Doppler are significantly higher in patients with hypertensive emergency compared to hypertensive urgency. The left ventricle hypertrophy on ECG, high LV mass index of >125 gm/m2, BMI > 30, old age > 60 year, male gender and history of hypertension and stroke were positive predictors of poor outcome and end organ damage.
Keywords
Introduction
Systolic blood pressure (SBP) continues to increase with age while diastolic blood pressure (DBP) declines leading to an increase in pulse pressure after the age of 55 years. This increment of pulse pressure leads to structural and functional damage to large vessels and other organs. 1
The sudden increment of blood pressure above optimal range results in end-organ damage (EOD) for myocardium, blood vessels, eyes, kidneys and brain. The signs of EOD herald a poor prognosis, late comorbidities and death.2,3
Hypertensive crisis is defined as SBP > 180 mmHg or DBP > 120 mmHg, with or without EOD. 4 It is further characterized as hypertensive urgency (HU) or hypertensive emergency (HE). Patients that presented with EOD are called HE and those without are called HU. 5 Patient with hypertensive emergencies may lead to pulmonary edema, acute myocardial infarction (MI), hypertensive encephalopathy, intracranial hemorrhage, dissecting aortic aneurysm and acute renal failure. 6
The pathophysiology of hypertensive emergency is not well understood, but the failure of normal auto-regulation and abrupt rise in systemic vascular resistance (SVR) may be the initial steps in the disease process followed by mechanical injury of endothelial, and activation of renin–angiotensin system.7,8
The rule of echocardiogram in the assessment of hypertensive heart disease has been well established. The pattern of pulsed Doppler LV diastolic filling had been classified into abnormal relaxation, pseudo normal and restrictive based on the ratio of early filling E velocity wave to the late filling atrial A velocity wave and duration of deceleration time (DT). 9 The restrictive pattern is characterized by high early (E) wave and decreased late (A) wave velocity, shortened (DT) of E wave, while the abnormal relaxation pattern had low E/A ratio of <1 and prolonged DT. 10
Furthermore, tissue Doppler velocity at the basal septum of mitral annulus has been recognized as a marker of myocardial stiffness in hypertensive patients. 11 It was shown earlier that the ratio of early diastolic filling wave (E) on pulsed Doppler to tissue Doppler of septal mitral annulus velocity (Em) correlate positively with the LV end-diastolic pressure (LVEDP). 12 Further, tissue Doppler velocities of the early diastolic wave (Em) and systolic wave (Sm) were both reduced in stiff hypertensive myocardium. 13
At present, the tissue Doppler echocardiographic changes in hypertensive emergency is unclear.
Aim
The study aims to assess the clinical manifestations and development of clinical events on admission for patients presented with hypertensive crisis (BP ≥ 180/120 mmHg); changes of pulsed and tissue Doppler indices in HE patients; and the predictive value of variables of clinical history, ECG voltage and biochemical markers for the risk of developing clinical events in hypertensive crisis.
Material and Methods
The clinical data of each patient admitted with hypertensive crisis were extracted from the files over the period of one year (January to December 2010). There were 7245 total medical admissions with 1449 (20%) patients presented as medical emergency and 241 (17%) of them presented as hypertensive crisis. An institutional medical approval was obtained before conducting the study.
Inclusion criteria: Every patient admitted to Salmaniya Medical Complex with SBP > 180 mmHg or DBP > 120 mmHg during the study period was included (n = 241).
Exclusion criteria: Patients were excluded from the study if they had advanced liver disease, end stage heart failure with LVEF% of <15% or patient's age less than 20 or above 90 years.
End-organ damage (EOD) was established from history, clinical examination and laboratory investigations of patients. Data of clinical history of each patient, symptoms on presentation to emergency room (ER) such as headache, malaise, palpitation, lightheadedness and epistaxes were recorded.
Likewise symptoms of end organ damage such as dyspnea due to pulmonary edema, acute chest pain of acute coronary syndrome, sensory or motor weakness of stroke, signs of left ventricular dysfunction (pulmonary edema) such as bi-basilar crackles and S3 gallop were recorded.
The level of SBP and DSP on admission, heart rate, acute myocardial infarction, arrhythmia, pulmonary edema and dissection of aorta were recorded. The development of stroke, transient ischemic attacks, and hypertensive encephalopathy or death were recorded.
The height and weight, body mass index (BMI), blood levels of creatinine and hemoglobin were recorded. Twelve leads ECG findings of voltage criteria of left ventricle hypertrophy (LVH) were recorded. Conduction abnormalities, atrial fibrillation, ST segment elevation or depression were also recorded. 14 Echocardiographic findings of M mode dimensions of LV septal and posterior wall thickness, left ventricle ejection fraction percentage (LVEF%) 15 were recorded. Derived LV mass index where LV mass > 136 gm/m2 for male and 125 g/m2 for female were defined as echo criteria of LVH, The left ventricle mass was calculated according to Devereux et al. 16
Pulsed Doppler data of E wave velocity, A wave velocity and E/A ratio, tissue Doppler velocity of E wave at basal septal area of mitral annulus for E wave (Em) and the ratio of E/Em were recorded.
The number of antihypertensive drugs for treatment of hypertension that used prior to admission was recorded. The intravenous medications administered for lowering the blood pressure in the ER were recorded.
Patients were divided into two groups: HE group (n = 62 with end organ damage) and HU group (n = 179 without).
Statistical analysis
The statistical analysis was performed using SPSS, version 17. Student's t-test was applied for continuous variables and Chi-square analysis for non-continuous variables data. Sensitivity and specificity of LVH on ECG was assessed against LVMI > 125 g/m2 as a gold standard.
The predictive risk of different clinical variables, ECG voltage of LVH for the development of clinical events was assessed using multiple linear Logistic regression analysis. All reported P-values are two tailed. P value was regarded as significant at level of <0.05.
Results
The total number of patients presented with hypertensive crisis was 241. Sixty two (26%) patients had clinical events suggestive of end organ damage (HE) and 179 (74%) had no end organ damage (HU).
Table 1 shows the characteristics of the patients in both groups. In the whole study, the mean age was 52.9 years (range 20–90), the percentage of male gender was 74%, those with history of diabetes mellitus prior to admission were 34%, 77% had history of hypertension, those with history of stroke of 7%, ischemic heart disease of 15% and smoking of 31%.
Previous history and clinical characteristics of patients presented with hypertensive crisis.
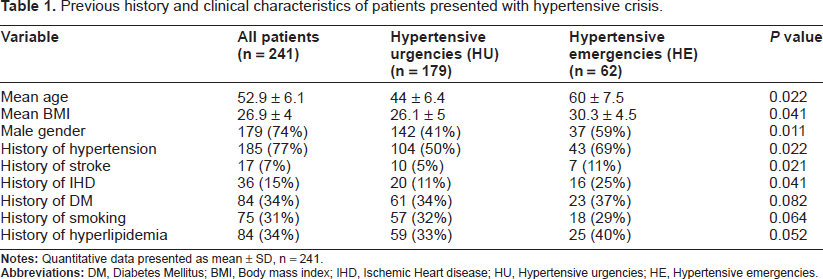
Patients with hypertensive emergency (HE) compared with HU, were significantly older, had higher male to female ration of, higher body mass index, higher history hypertension, ischemic heart disease and previous stroke.
Table 2 shows the biochemical and clinical data for both groups. Patients with HE had significantly higher mean SBP on admission (221.50 ± 13.38 vs. 195.13 ± 18.45 mmHg, P = 0.02), higher heart rate (96.87 ± 14.23 vs. 70.45 ± 7.34, P = 0.037), higher body mass index and higher serum creatinine. The difference of hemoglobin level in both groups was not statistically significant.
Biometric and biochemical data in patients with hypertensive crisis. hypertensive emergencies (he) are patients with end-organ damage (EOD). Hypertensive urgencies (HU) are those without EOD.
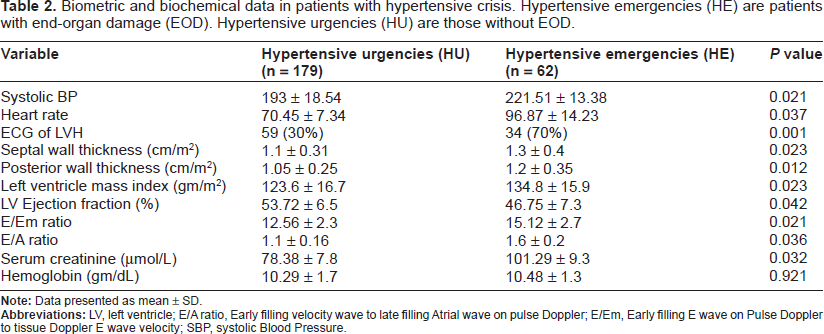
On echocardiogram, the mean index of left ventricle septal wall and posterior wall thickness in HE group compared with the HU group were significant of 1.3 ± 0.4 cm/m2 vs. 1.1 ± 0.3 cm/m2, P < 0.01. Likewise, the mean of LV mass index was 134 gm/m2 vs. 123 gm/m2, P < 0.001, with 148 (61%) patients in the whole study having LVMI > 125 gm/m2. The E/A ratio on pulsed Doppler echocardiogram was significantly higher 1.6 vs. 1.1, the ratio of E/Em was significantly higher of 15.12 vs. 12.56 and LVEF% was significantly lower of 47% vs. 54%.
Voltage Criteria on ECG
In all patients in the study, 12 leads ECG showed voltage criteria of LVH in 96 (40%) patients, 32 (13%) of them had strain pattern. LVH was shown in 59/179 (33%) in patients with HU, 34/62 (54%) in HE with sensitivity of 65% and specificity of 81%. Fourteen patients (6%) had atrial fibrillation while the rest of patients were in sinus rhythm and four had left bundle branch block.
Figure 1, shows the frequencies of clinical manifestations in all patients presented with hypertensive crisis (n = 241). Those presented with headache were of 25%, 23% had generalized malaise, 18% had light headedness, 20% had palpitation and 14% had epistaxis.
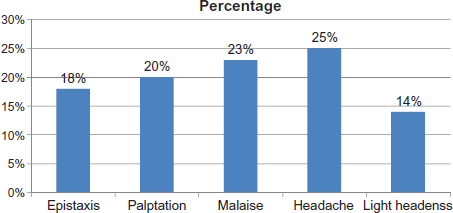
Percentage of clinical manifestations in patients admitted with hypertensive crisis, n = 241.
Figure 2 disclosed patient's percentage of those presented with end organ damage in the HE group, 16% had pulmonary odema, 6% had stroke, 5% had acute myocardial infarction and 4% had unstable angina.
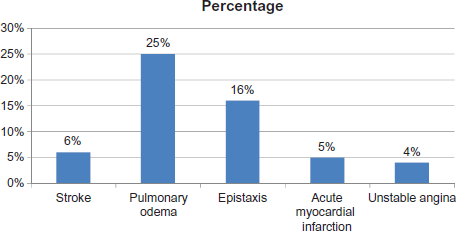
Percentage of end organ damage in patients admitted with hypertensive emergency, n = 62.
In patients with acute coronary syndrome, 14 had acute myocardial infarction and ten had unstable angina. In the HE group, 5 patients died, four had intra-cerebral bleeding and one went into severe pulmonary congestion and cardiac arrest. No death occurred in the HU group.
Table 3 shows the predictive risk of clinical events of different biochemical and clinical variables in the whole study group after adjustment for age and sex. The voltage criteria on ECG, LV mass index 125 gm/m2, body mass index > 30, further the odds of male gender, history of hypertension, history of DM, age > 60 years, and the high serum creatinine were positive predictors. The odds of smoking and hyperlipidemia were of no significant predictive value.
The odds ratio and confidence interval of different clinical and biometric variables in the risk prediction of clinical events in patients presented with hypertension crisis.

Antihypertensive medication
In the whole study 185 (77%) patients were on antihypertensive drugs prior to admission. The number of antihypertensive medication was as follows: 12% were on single drug, 32% were on two drugs, 50% were on three drugs, and 6% were on 4 drugs. The most frequent combinations of antihypertensive medication were diuretics and angiotensin I receptor antagonists (ACE) of 46% or on diuretic, angiotensin II receptor antagonist (ARB) with calcium blocker of 20% and diuretic, ARB and beta blocker in 12%.
There were 56 (23%) patients on no medication for hypertension prior to hospital admission and the high blood pressure was observed without being aware of the problem.
All patients were presented as hypertensive emergency, (n = 63 and 55(22%) patients with hypertensive urgency were give an intravenous medication to lower the BP. There were 55 patients that were commenced on IV nitroglycerine with IN furosemide, 15 patients given on nitroglycerine alone and 47 patients given labetalol IV.
Concomitant oral combination of diuretics and angiotensin I converting enzyme inhibitor (ACE) were commenced in 20% of patients, diuretic and angiotensin II receptor antagonist (ARB) in 25% and diuretics, ACE and beta-blocker in 30% and diuretic, ARB with calcium blocker in 25%.
Discussion
In this study, 26% of patients had hypertensive emergency with end organ damage in the form of pulmonary edema, acute coronary syndrome or stoke and 74% had hypertensive urgency with end organ damage. These finding are in agreement with previous report where HU of 76% and 24% of hypertensive emergency, 17 and differ from another with prevalence of HE of 39% and HU of 60%. 18
Voltage criteria of Left ventricular hypertrophy on ECG were higher in HE patients of 55% compared with HU of 32%. The low sensitivity and high specificity of voltage criteria on ECG is in agreement with a previous study, however, in that study the population were not in hypertensive crisis. 19
The LV mass index of >125 gm/m2 on echo was significantly higher in HE patients and was an independent predictor of clinical events, this was in agreement with previous report where LVM index was the highest independent predictor for risk of future events. 20
Patients with HE compared with HU had higher wall thickness and higher LV mass index on M mode. Furthermore, there was higher E/A ratio on pulsed Doppler echocardiogram that was suggestive of restrictive pattern with higher tissue Doppler ratio of E/Em of >15. In a previous report, the tissue Doppler velocity for the basal septum did correlate positively with the LV end diastolic pressure and restrictive pattern on echo Doppler. 21
The clinical presentation on admission showed an incidence of stroke of 6% and pulmonary edema of 16%, which was lower than two previous reports, where in the first report, stroke rate was 24% and 23% had pulmonary odema 22 and of 24.5% for stroke and 22.5% for pulmonary edema in the second report. 23 Patients with HE who sustained end organ damage were significantly older compared with HU patient. The significant number of old age in HE was in agreement with a previous report where 50% of patients with HE were old (60–70 years). 24 The lack of awareness of hypertension on admission of 23% was similar to previous report where 22% of adults were unaware of hypertension on admission. 25
Further, prevalence of diabetes mellitus in the study patients was of 34%. The prevalence of DM was previously reported in Bahraini population of 38% and the history of hypertension was 21%. 26
Patients who were already on antihypertensive combinations on admission were of 55% using three drugs, 32% using two drugs, while 6% were on four and 7% were on one drug. The rate of using combination of drugs were higher than early report in Bahrain where 37% were using two drugs and 63% were using single therapy. 27 This highlights the fact that there is a trend for using more combination therapy in hypertensive population.
The finding of high prevalence of DM in this study is different from other previous two reports of normal population, with prevalence of 14% and 35% respectively.28,29
The predictive risk for clinical events was positive for male gender, history of hypertension, DM, high serum creatinine, and high body mass index. These findings were in agreement with previous report regarding the predictive value of these variables in patients with uncontrolled hypertension. 30
Further, the predictive risk was positive for pulsed Doppler E/A ratio of >1.6 and E/Em ratio of >15 on tissue Doppler. Such high positive independent predictive risk is in keeping with previous reports where patients with hypertensive heart failure had severe diastolic dysfunction with restrictive pattern on pulsed Doppler with high tissue Doppler ratio of E/Em > 15 suggestive of high left ventricle diastolic pressure. 31
Patients presented with acute coronary syndrome with or without acute infarction in the study population mostly had the onset of ischemia secondary to the sudden failure of auto regulation and the abrupt rise in systemic vascular resistance in hypertensive crisis leading to the release of more vasoconstrictors and further vascular injury of myocardium. 32 Further the subsequent increase in blood pressure generates endothelial injury leading to increased permeability, the release of additional vaso-active mediators generating a vicious cycle of ongoing injury, causing organ dysfunction and development of Pulmonary edema. 33 The development of dyspnea and pulmonary odema in HC is associated with the rapid accumulation of fluid within the lung's interstitial and alveolar spaces due to acute elevated cardiac filling pressures. 33
In hypertensive crisis the diastolic myocardial dysfunction with increase in ventricular stiffness and impaired relaxation impedes ventricular filling during diastole due to left ventricular hypertrophy, restrictive cardiomyopathy and increase after load. 34
Tissue Doppler velocity of the mitral annulus was observed to be suppressed in hypertensive patients, further it was observed that the E/Em ratio of >10 has is a recognized noninvasive index for the assess left ventricular filling pressures was predictive of a mean pulmonary capillary wedge pressure above 15 mmHg with a sensitivity and specificity of 92 and 80 percent, respectively.12,35
Limitations of the study
This retrospective study had a few limitations as the data were incomplete for some patients particularly the fundus examination and the presence of protein in urine on admission. Also the number of patients who had the pulsed Doppler and tissue Doppler echo in the same day of admission was limited to 30% in the study, 45% on the second day and 25% on third and fourth day where the BP was mostly controlled. This difference of echo performance may influence the pulsed and tissue Doppler velocities which may vary among individual patients.
Conclusion
In patients presented with hypertensive crisis, the echo indices of E/A ratio and E/Em ratio of tissue Doppler are significantly higher in patients with hypertensive emergency compared to hypertensive urgency. The left ventricle hypertrophy on ECG, high LV mass index of >125 gm/m2, BMI > 30, old age > 60 year, male gender and history of hypertension and stroke were positive predictors of poor outcome and end organ damage.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.