
Abstract
Deep sternal wound complications represent a significant problem in current open heart surgery and still pose a tremendous challenge to surgeons. Over the years, many treatment modalities have been proposed, but only few found their way into daily clinical practice of cardiothoracic surgeons. A gold standard has not been defined yet. This review was designed to give an overview of the preferred surgical strategies.
Introduction
The median sternotomy was reintroduced by Julian in 1957 after its initial description by Milton in 1897 and is now the standard approach for open heart surgical procedures. 1 In contrast to the standardized division of the sternum with an oscillating saw, the closure of a sternotomy can be accomplished in many different ways. According to a survey in 2006 in Germany, surgical wires are used in the majority of cases (87%), mainly passed trans/peristernally (64%). 2 The preferred osteosynthetic procedure for patients with an increased risk for sternal instability is the method of Robicsek.2,3
Despite several technical variations and improvements over the years, a small percentage of patients suffers sternal wound complications, of which deep infections involving sternal bone and mediastinum are most relevant. The incidence of the former has been reported as 0.6% to 5%, with a mortality rate being twice that of patients without medistinitis.4–6 In many cardiosurgical centers, these patients pose a considerable challenge with regard to the optimal treatment procedure. Financial implications have to be discussed as well, since many of the treatment options are not only clinically cumbersome but also time demanding and therefore costly. Before 1980, sternal debridement, mediastinal irrigation, and rewiring was the preferred approach, which was followed by a hype for coverage with autologous (omental or muscle) flaps.7–10 A decade ago, plate fixation came into play but remained poorly accepted.11,12 Recently, negative pressure wound therapy, also termed vacuum therapy, was introduced as another treatment modality, especially in the case of deep sternal wound infection, and has gained widespread acceptance within a short period of time for its simplicity.13–15
Nowadays, in most institutions, the surgical approach follows the surgeon's preference as there is no robust clinical evidence.16,17 To alleviate decision making, we summarized the therapeutical options and treatment strategies for deep sternal wound complications. The concomitant antibiotic treatment, which is an integral part in case of severe soft tissue and bone infection, has not been included and analyzed in detail because it's not the focus of the review, and several recommendations already exist.
Spectrum of Sternal Complications
Deep sternal complications involve not only skin and subcutaneous tissue but may also affect the bone. Infection of the sternal wires can also be present. With regard to the specific surgical treatment, we discriminate the following pathologies: noninfected sternal instability, deep sternal wound infection without sternal instability, and deep sternal wound infection with sternal instability.
Noninfected Sternal instability
An inadequate mobilization of the patient with high traction forces to the sternal edges as may also develop with severe coughing can tear the wires through the sternal bone. A rapid process destroys osseous integrity and leads to immediate sternal instability. A more gradual course creates a gliding trauma that leads to a cartilaginous metaplasia with less movement of the fragments, but usually ensues chronic pain syndromes.
Deep Sternal Wound Infection without Sternal Instability
Obese patients with a good sternal bone structure or women with extraordinarily large breasts can develop considerable distension of the skin layer that results in an avulsion of the skin suture line. Impaired wound healing, especially in diabetic patients, and ongoing tension then aggravates the problem, ultimately resulting in a secondary deep wound infection.
Deep Sternal Wound Infection with Sternal Instability
Deep sternal wound infection with sternal instability is the most deleterious situation. A maintained structure of the sternal halfs is less frequent and mostly related to a loosening or rupture of sternal wires. The ongoing movement of the sternal edges promotes inflammation, effusion, and secondary infection. More often, deep sternal wound infection and sternal instability are associated with extensive bone loss. Not infrequently, a total destruction of the sternum is present when the wires cut the bone into small pieces. Most of these patients suffer not only from extensive sternal infection, but also from severe respiratory problems, often associated with pneumonia.
This discrimination of pathologies is in accordance with the most commonly applied classification for sternal complications as has been proposed by El Oakley and Wright. 18 They distinguished between uninfected dehiscence (class 1), superficial wound infections without sternal instability (class 2A), and deep sternal wound infections with or without dehiscence (class 2B). 18 There have been other classifications, but these do not indicate the type of reconstruction necessary. Pairolero and Arnold have based their classification of sternal wounds on the timing of presentation of the infection. 19 In their classification, Type I wounds occur in the first few days post-operatively, contain early wound separation with or without sternal instability, and are characterized by serosanguineous drainage without cellulitis, osteomyelitis, or costochondritis. Type II wounds occur within the first few weeks and are characterized by drainage, cellulitis, mediastinal suppuration, and positive cultures (fulminant mediastinitis). Type III wounds occur months to years after surgery and are characterized by the presence of chronic draining sinus tracts, localized cellulites, osteomyelitis, or retained foreign bodies. Mediastinitis is a rare finding.
Risk Factors
Various risk factors have been related to the development of deep sternal wound complications. Risk factors were either patient- or comorbidity-related and included chronic obstructive pulmonary disease, diabetes, obesity, chronic cough, osteoporosis, reoperation, irradiation, previous myocardial infarction, and age or were procedure-related, such as the use of bilateral mammary arteries for coronary bypass surgery or the duration of surgery, prolonged mechanical ventilation, and the need for reexploration.20–23 Interestingly, it is still unclear whether there is an advantage for the sternal microcirculation when harvesting the internal thoracic artery in a skeletonized fashion as compared with the pedicled technique.24–26 Moreover, Medalion et al found acute postoperative sternal ischemia caused by harvesting of a pedicled left internal thoracic artery to be temporary and resolving with time. 27 Strong coughing also considerably jeopardizes sternal stability as the intrathoracic pressure may rise up to 300 mmHg, which induces strong shearing forces in the anterior-posterior and lateral directions, and which may also easily untwist the wires28,29 (Table 1).
Risk factors. a
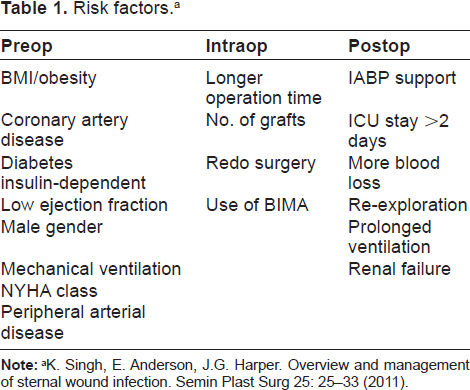
K. Singh, E. Anderson, J.G. Harper. Overview and management of sternal wound infection. Semin Plast Surg 25: 25–33 (2011).
Diagnostic Procedures
A major clinical issue is that many of the sternal problems become clinically evident rather late; in about half of the patients, this is only after discharge. 30 As a consequence, suppuration and formation of granulation tissue may alter a standardized treatment protocol. Most important is to evaluate the patient clinically first. If the sternal wound is inconspicuous and without redness and hyperthermia, bimanual palpation follows to assess sternal stability. However, the degree of instability cannot be always judged correctly by palpation. It may well happen that a sternal dehiscence can be missed. Due to this high probability of error and the fact that the extent of an assumed sternal dehiscence may have an impact on the surgical treatment to be employed, a computed tomography (CT) scan is strongly recommended to clearly visualize the integrity of the sternum.
Severely compromised bedridden patients with a septic status usually demonstrate extensive findings including large skin defects with considerable suppuration, sometimes with a visible and usually dehiscent sternum and infected (and loosened) wires. In these cases, no further diagnostic procedures are necessary; the patient requires immediate treatment. The proper diagnosis can be established during surgical revision. Nevertheless, sometimes a preoperative CT scan is advocated to identify deep mediastinal collections, abcesses, as well as pleural effusions and empyema. A transesophageal echocardiography (TEE) may rule out associated prosthetic valve endocarditis.
However, between these two scenarios, there are many wound situations which can be assessed and responded to in both ways.
Treatment Options
Currently, the European and American cardiothoracic societies provide no guidelines for the treatment of deep sternal wound complications. Patients are treated in many different ways according to general surgery rules of infection and institutional experience. General recommendations for clear-cut and extreme conditions are simpler to suggest, whereas borderline or complex wound situations mandate a more individualized decision making (Fig. 1).
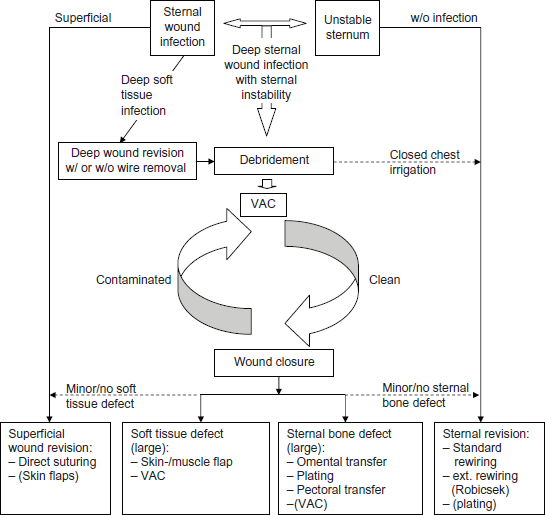
Treatment algorithm.
Noninfected Sternal instability
The aim of surgery is to reestablish sternal stability. Regardless whether the whole sternum or only a part of it is involved, the optimal surgical technique depends on the integrity of the sternal wound edges and the bone quality. If the sternal wires are only loosened, they can be simply strengthened. In inadvertent paramedian sternotomy, plating works well and can be recommended. If the wires are torn off the bone but the sternal edges still seem sufficiently intact, rewiring may suffice. Whether simple loops, figure-of-eight, or the Robicsek technique is better is probably less important and up to the surgeon's discretion and experience.31,32 There have been many more suggestions in the literature, including the addition of absorbable pins, but none has been proven to be superior to all others.33–38 As more wires provide more stability, obese patients are frequently treated with a higher number of wires or with sternal bands if the bone is sufficiently robust.39,40 In patients with extraordinary osteoporosis, wires easily tear through the fragile bone. Nonabsorbable braided sutures for these patients can be well anchored in or around the bone. 41 Overall, there is no common agreement with regard to the optimal surgical technique in frail and obese patients, and failure rates are significantly. 41
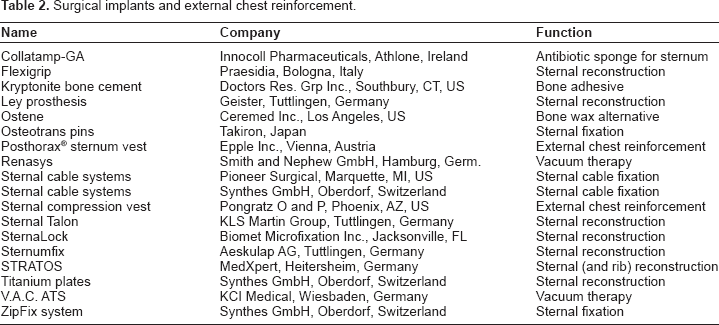
Recently, specifically designed plate fixation became available. A few plates including horizontal titanium plates (Synthes GmbH, Oberdorf, Switzerland), the SternaLock (Biomet Microfixation Inc., Jacksonville, FL), and the Sternal Talon (KLS Martin Group, Tuttlingen, Germany) have been devised, some of which can be unlocked in case of emergency situations.42–44 The Strasbourg Thoracic Osteosyntheses System (STRATOS) consists of rib clips with different angulations and connecting bars with adjustable length (MedXpert, Heitersheim, Germany). 45 All these systems serve the purpose well but are not absolutely necessary, as standard trauma plates can be used as well in most instances. 46 As in the case of the ZipFix system (Synthes GmbH, Oberdorf, Switzerland) consisting of poly-ether-ether-ketone implants similar to cable ties and thermo-reactive nitinol clips (Flexigrip, Praesidia, Bologna, Italy), a place in the clinical routine for all of the above systems has not been established yet47,48 (Table 2).
Surgical implants and external chest reinforcement.
Deep Sternal Wound Infection without Sternal instability
The most important goal in the surgical treatment of deep sternal wound infection is the elimination of the infectious focus. Therefore, an extensive debridement and antibiotic treatment is compulsory under all circumstances. The first task is to clean the wound from pus and necrosis. Depended on the extent of involvement, if there is an abscess and the skin is still closed, the wound may have to be reopened. In this regard, more is better than less. The area should be extensively rinsed to clear the wound from debris and to reduce the bacterial load. All necrotic tissues must be removed until adequately perfused tissue is visible. If the sternum is sufficiently stable, infected sternal wires should be removed to get rid of the bacterial biofilm as microorganisms have a considerable affiliation towards foreign bodies, especially coagulase-negative staphylococcus (CONS). The entry sides of the wires into the sternal bone should be inspected and locally debrided with a small sharp spoon as well if infection is present. Early after cardiac surgery, when the sternal edges are not sufficiently fused, extraction of the wires is awkward as it results in sternal dehiscence and instability. An individual decision has to be made as to whether the wires can be left in place or not. If the wires have to be removed, pericardial closure and pleural flap advancement are recommended to prevent right ventricular rupture and to facilitate vacuum assisted closure (VAC) therapy (see below). Under fortunate conditions, the sternal bone can heal despite infected wires, leaving only a small fistula to the skin. At a later stage, the wires are then removed and the fistula excised. Otherwise, when wire removal cannot be avoided, and removal results in sternal dehiscence, an open therapy is indispensable.
While these initial steps of wound debridement are commonplace and well accepted, the consecutive management is more debated. The main question is whether to primary close the wound or not. If there is no large wound defect, and infection has been presumably eradicated for the most part, primary wound closure with one or more drainage catheters is certainly a good option. Minor wound defects can be covered by mobilizing the pectoral muscles. If a larger wound defect is remaining mandating consecutive plastic surgery, it is advisable not to primarily close the wound as recurrent infection would be disastrous. It has been hypothesized that a delayed primary closure is superior to a late secondary closure. 49 An open treatment with packed gauzes or towels, or even better with VAC therapy until the wound is definitely clean and granulation tissue is forming is an attractive alternative, especially in extensive infection, which cannot be fully controlled by a surgical debridement.50,51 VAC therapy has been shown to increase peristernal blood flow, even in the face of internal mammary artery harvest, and to reduce bacterial loads leading to enhanced granulation tissue formation. 52 Secondary closure of the wound can be achieved (with or without plastic surgery) after an appropriate open treatment period. 53 The optimal time for closure is still under debate. 49
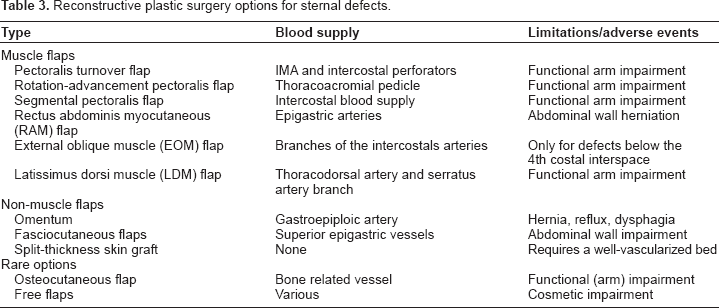
In case of ongoing subclinical infection, especially post transplant, after implantation of Dacron grafts, and following infection of a ventricular assist device as well as following total sternectomy, an omental transposition is a traditional option. 7 The median sternotomy is extended caudally and the peritoneal cavity is entered. The omentum is mobilized and is brought up to the chest through a diaphragmatic incision. It is placed above the sternum and below the soft tissue coverage. Remaining soft tissue defects can be dealt with by a variety of plastic surgery options; however, in most cases, a simple mobilization of the pectoralis major muscle suffices. 16 In odd situations were infection cannot be controlled despite all efforts, repetitive wound cleaning and granulation without secondary closure remains the only successful therapy (Table 3).
Reconstructive plastic surgery options for sternal defects.
Deep Sternal Wound Infection with Sternal Instability
The most frequent sternal complication after cardiac surgery is complete or partial dehiscence and fragmentation of the sternal structure with a secondary wound infection. On exceptional occasions, infection starts superficially and affects an a priori stable sternum which has to be unjoined due to extensive involvement of the sternal wires. Regardless of the cause and underlying pathophysiology, infection and instability both have to be treated. As infection always has priority, the surgical debridement has to be achieved first. In a localized infection, the non-infected part of the sternum can be left untouched. If the sternal instability involves the whole sternum or is associated with an ongoing mobility of the sternal edges, a complete wound revision is necessary. After reopening the sternum, the mediastinum has to be inspected for and cleaned from infection including excision of necrotic tissue and extensive rinsing. The sternal edges have to be cleared from syndesmotic coverage. Postoperatively, repeat C-reactive protein (CRP) measurements, bacterial swabs, and blood cultures are necessary to prove successful eradication of infection. Otherwise further mediastinal revisions are indispensable. An optimization of the nutritional status and the nitrogen balance can be considered as well. When obtaining a “clean” mediastinum, there is usually a large defect involving soft tissue and bone.
Again, a key question for success is whether to immediately close the wound. It has to be assumed that infection behind the sternum may not be completely eradicated. The more convenient treatment for patient and physician is continuous antibiotic tube irrigation with stabilization of the sternum and closure of the wound, which was devised in 1963.10,54 The patient can be immediately extubated and also mobilized if the sternum is salvageable. A notable risk for an infectious relapse remains, since mediastinal rinsing is limited in its efficacy. 2 Far better results have been obtained when an additional omental flap has been transposed to cover the entire mediastinum. 55 Leaving the mediastinum open is another alternative. No matter whether the mediastinum is packed with towels or provided with a VAC system, repetitive changes of wound dressings in a 2 to 5 day interval have a high potential to effectively control infection. The skin can be temporarily closed to prevent wound retraction. When the mediastinum becomes clean, secondary wound closure is anticipated. Due to the fragmentation of the sternum, rewiring is usually difficult and placement of titanium plates much safer. Soft tissue reconstruction is predominantly achieved with pectoral flaps. Very large defects require more sophisticated plastic surgical options 17 (Table 3).
Most problematic are the cases with a fulminant mediastinitis and fragmented necrotic sternal bone early after surgery when the heart is not yet covered with granulation tissue and “exposed to the air.” Repetitive extensive debridement and rinsing is without alternative. However, an open sternum exposes the patient to several risks in the long run, mainly respirator-associated pneumonia, decubitus, systemic inflammatory response syndrome (SIRS), and sepsis. Nowadays, VAC therapy is the solution for long-term treatment, but the foam dressings on which suction is applied cannot be placed directly onto the heart. In these situations, transfer of the omentum is an option, which can be covered by a thin soft silicone faced polyurethane foam sheet (Mepilex, Mölnlycke Health Care, Gothenburg, Sweden) on top of which a VAC is installed. Secondary wound closure follows when clean wound conditions are achieved. 56
Outcome
Hospital stay is rather long for patients with deep sternal wound infection, usually 4 to 8 weeks. 16 A multiple site infection is not uncommon, especially with staphylococcus aureus and methicillin-resistant staphylococcus aureus (MRSA) infection. 57 The overall mortality in these patients ranges from 9% to 29%, and is highest with a true mediastinitis and close to zero without it.16,49,58 Complications, seen in about 20% of patients, include hematoma, partial flap loss, and recurrent wound dehiscence.16,58 The most devastating complication is a laceration of the right ventricle when the sternum has not been primarily closed. Multiple further problems may arise from longer-term immobilization.
The hospitalization for extended VAC therapy has been reported to average 25 ± 20 days, whereas the mortality has been noted to be about 15% in recent literature. 59 Complications with VAC use include a possible increased risk of bleeding and potential damage to the underlying tissue. The duration of VAC therapy is still an issue of debate as recent reports suggest that prolonged VAC use for more than 3 weeks can be detrimental by causing recurrent sternal breakdown, infection, and osteomyelitis.60–62
Omental transfer has success rates exceeding 95% and low mortality rates. 63 A 5-year survival rate of 82% was reported as early as 1995. 64 However, the exercise capacity after omental flap transposition has been shown to be considerably reduced, as expressed by a lower percent vital capacity and lower oxygen consumption (VO2) and a longer 200 m walking time. 65 Due to the immunologic properties and the ability to conform to the deepest recesses, the omental flap is frequently considered superior to muscle flaps. 63 Moreover, the emergence of laparoscopic omental harvest has placed more attention on its use, which might reduce the incidence of abdominal hernia. 66 Likewise, comparing omental transfer with muscle flaps a recent review paper suggests a slightly higher mortality rate with a relative risk of 1.29 for the use of muscle flaps. 67
Complications of muscle flaps include reexploration for flap necrosis in 3% to 19% of cases, hematomas and seromas in 6% to 10%, as well as a high rate of arm or shoulder weakness (31%) and chest wall pain (43%–51%). 67 Hernia formation and protrusion are a further concern of abdominal flaps.58,68
Prevention
Check lists of standardized procedures to prevent infection in cardiac surgery have been devised by several institutions. These recommendations include screening for MRSA and MRSA decolonization, optimal blood glucose level adjustment, and other hygienic measures as well as timely application of antibiotics adapted to preexisting infection and adequate surgical hand disinfection. After surgery, decolonization and blood glucose level adjustments should continue, whereas a perioperative antibiotic prophylaxis should be terminated at day 1. However, there are also more basic principles to be followed such as opening the sternum strictly midline and tension free wound adaption, which are hardly ever mentioned in the literature.
Several ideas have been devised to specifically reduce sternal instability and consecutive infection. (1) In extreme sternal stabilization, there has been well-understood evidence that more wires are better than fewer. However, this concept does not work in a soft bone structure or severe osteoporosis. In the latter, nonabsorbable braided sutures can be added to conventional wiring. Newer ideas included rigid brackets like the single or double legged Sternal Talon (KLS Martin Group, Tuttlingen, Germany) and Sternumfix (Aeskulap AG, Tuttlingen, Germany) devices as well as various sternal cable systems (Synthes GmbH, Oberdorf, Switzerland; Pioneer Surgical, Marquette, MI, USA). 69 (2) Reduction of sternal bleeding with hemostyptic agents such as fibrin glue, avoiding the use of bone wax, has been suggested. Ostene (Ceremed Inc., Los Angeles, CA, USA) is a water soluble bone wax alternative that showed excellent results in animal experiments but did not enter the clinical arena as other polymers have.70–72 (3) The application of local collagen-gentamicin sponges (Collatamp-GA, Innocoll Pharmaceuticals, Athlone, Ireland) between the sternum halves just before closure significantly was shown to reduce the infection rate but to increase the risk of bleeding and dehiscence. 73 (4) The use of osteoconductive bone adhesive to augment conventional wire cerclage has been introduced recently. All patients treated with Kryptonite bone adhesive (Doctors Research Group Inc., Southbury, CT, USA) recovered well with no adverse side effects or adhesive-associated complications. 74 (5) Various external chest reinforcements with vests have been devised. The Posthorax sternum vest (Epple Inc., Vienna, Austria) was designed for anteroposterior stabilization of the chest. Two pads are placed on each side of the sternum to prevent intrinsic movement of the 2 sternum halves, whereas lateral flaps are designed for optimum fit. 20 In a prospective randomized multicenter trial, it was shown that the need for reoperation could be reduced from 3.9% to 0.6%. 75 The Sternal Compression Vest (www.sternalvest.com) is indicated for stabilization of poststernectomy wound sites and thoracic surgical sites secondary to postcardiac surgery or plastic surgery procedures. An individual custom-made complete thoracic compression garment vest has been reported as well. 76 It is important that these vests allow normal breathing, and over-extension is banned (Table 4).
Check list prevention of infection in cardiac surgery. a
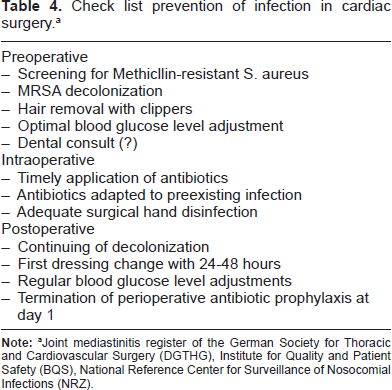
Joint mediastinitis register of the German Society for Thoracic and Cardiovascular Surgery (DGTHG), Institute for Quality and Patient Safety (BQS), National Reference Center for Surveillance of Nosocomial Infections (NRZ).
Conclusion
Deep sternal wound complications are infrequent but significant complications in open heart surgery. The spectrum of clinical findings is broad; the diagnostic pathway is restricted to clinical judgement, microbiological swabs, and CT scan. Risk factors, prevention, and treatment are heavily debated and not standardized. Interestingly, the available literature is sparse, and large clinical trials are lacking. Considering the financial implications of these complications for the public health care system, development of guidelines would be helpful.
Author Contributions
Wrote the first draft of the manuscript: LR. Contributed to the writing of the manuscript: CS. Agree with manuscript results and conclusions: LR, CS. Jointly developed the structure and arguments for the paper: LR, CS. Made critical revisions and approved final version: LR, CS. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.