
Abstract
Background
Fetal surgery is selectively offered for severe or life-threatening fetal malformations. These infants are often born prematurely and are thus at risk for retinopathy of prematurity (ROP). It is not known whether fetal surgery confers an increased risk of developing severe ROP relative to published rates in standard premature populations ≤37 weeks of age grouped by birth weight (<1500 grams or ≥1500 grams).
Design
This is a retrospective chart review.
Methods
We reviewed the charts of 137 patients who underwent open fetal/fetoscopic surgery from 1996–2004. Surgical indications included twin-twin transfusion syndrome (TTTS), myelomeningocele (MMC), congenital diaphragmatic hernia (CDH), sacrococcygeal teratoma (SCT), cystic adenomatoid malformation of the lung (CCAM), and twin reversed arterial perfusion sequence (TRAP). Of these, 17 patients had local ROP examination data. Binomial tests were performed to assess whether rates of ROP in our fetal/fetoscopic surgery cohort were significantly different from published rates.
Results
There were 5 patients each with an underlying diagnosis of TTTS and MMC, 2 patients each with CDH and TRAP, and 1 patient each with SCT, CCAM, and mediastinal teratoma. The mean gestational age at surgery was 23 4 /7 ± 2 3 /7 weeks, mean gestational age at birth was 30 ± 2 5 /7 weeks, and mean birth weight was 1449 ± 510 grams (610–2485). Compared to published rates of ROP and threshold ROP, our fetal surgery patients had significantly higher rates of ROP and threshold ROP in both the <1500 grams and the ≥1500 grams group (all p-values <0.05).
Conclusions
Fetal/fetoscopic surgery appears to significantly increase the rate of ROP and threshold ROP development. Greater numbers are needed to confirm these observations.
Introduction
Fetal surgery is selectively performed for severe or life-threatening fetal malformations. The first successful fetal surgery was performed in 1981 at the University of California, San Francisco and involved the placement of a catheter to relieve urinary tract obstruction in a twin with prune belly syndrome. 1 Since then, thousands of fetal surgical procedures have been performed with varied outcomes. There are three main approaches to fetal intervention: open fetal surgery, fetoscopic surgery, and fetal image guided surgery. In open fetal surgery, the mother is anesthetized, an incision is made in the lower abdomen to expose the uterus, the uterus is opened using a special stapling device to prevent bleeding, surgical repair of the fetus is performed, the uterine and maternal abdominal walls are closed, and the mother is awakened. Open fetal surgery is performed for congenital cystic adenomatoid malformation (CCAM), sacrococcygeal teratoma (SCT), myelomeningocele (MMC) (see Fig. 1), and congenital diaphragmatic hernia (CDH). Fetoscopic surgery is less invasive and can be done percutaneously or in some cases with a mini-laparotomy, with the use of small endoscopic instruments to visualize the fetus while operating. Fetoscopic surgery is performed for laser ablation of vessels in the twin-twin transfusion syndrome (TTTS) (see Fig. 2), cord ligation/division, cystoscopic ablation of posterior urethral valves, division of amniotic bands, and balloon occlusion of the trachea in CDH. Fetal image guided surgery (FIGS) is the least invasive technique, and involves manipulation of the fetus entirely under real-time cross-sectional view provided sonographically for percutaneous needle or catheter placement. FIGS is used for amnioreduction/infusion, fetal blood sampling, radiofrequency ablation for anomalous twins, vesico/pleuro amniotic shunts, cord monopolar cautery, and balloon dilation for aortic stenosis.
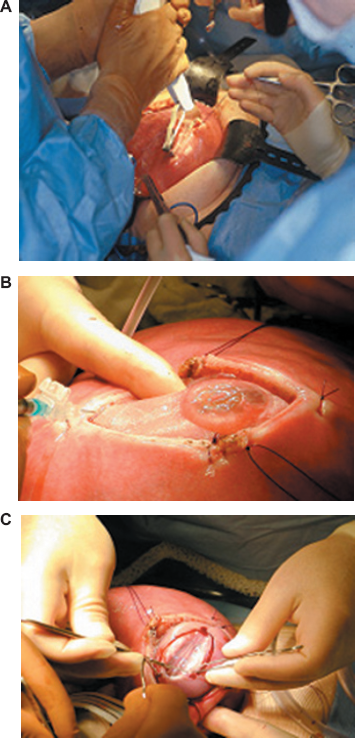
Open Fetal Surgical Repair of Myelomeningocele.

Fetoscopic Laser Ablation of Vascular Communications in Twin-Twin Transfusion Syndrome.
The vast majority of fetal surgery patients are born prematurely (birth at <37 weeks gestational age) in comparison to about 12% of the general population (2001 data from the National Center for Health Statistics). This is thought to be due to the underlying disorders of fetal surgery patients as well as the premature rupture of membranes (PROM) and preterm labor that results from post-operative uterine irritability.2–3 A study in sheep showed that in open hysterotomy, uterine blood flow and uteroplacental oxygen delivery reduced to 73% of its initial value, while remaining unchanged in the endoscopic approach. 4 Compared to open fetal surgery, human fetoscopic surgery has a lower frequency of preterm labor with less use of tocolytics, decreased maternal hospital stay, and decreased maternal complications due to tocolysis.5,6 However, fetoscopic surgery has not yet been shown to significantly prolong time in utero or reduce the incidence of PROM. PROM is less common in single port procedures, such as laser coagulation for TTTS, occurring in 6%-10% of cases, 7 while it occurs in up to 40%-60% in multiple port procedures with longer operating times. 5
Retinopathy of prematurity (ROP) is a retinal disorder of low birth weight premature infants that potentially leads to blindness and confers an increased risk for myopia, strabismus, amblyopia, and glaucoma. 8 13 In 2006, the American Academy of Pediatrics, American Association for Pediatric Ophthalmology and Strabismus, and the American Academy of Ophthalmology issued a joint statement recommending the screening of infants with a birth weight of <1500 grams (g) or with a gestational age of ≤32 weeks, as well as selected infants between 1500 and 2000 g with an unstable clinical course believed to be at high risk by their attending pediatrician or neonatologist. 12 This is a revision of the 2001 recommendation of an age threshold of ≤28 weeks. 13 At our institution, all infants <1500 g or with a gestational age ≥32 weeks were screened for ROP throughout the period of this study. The timing of fetal surgery prior to the 24th week of gestation coincides with early retinal vascular development. Increased physiologic stress, hypoxia, and early light exposure that could occur at the time of surgery (especially in open fetal surgery) may adversely affect normal retinal vascular development. It is also unknown whether fetal surgery causes upregulation in angiogenic factors such as VEGF that might play a role in ROP development. Of the conditions treated by fetal surgery in this study (CCAM, SCT, MMC, CDH, TTTS), only TTTS has been shown to cause an increase in serum VEGF (for both donors and recipients). 14 The purpose of this study was to determine whether fetal surgery confers an increased risk of ROP and threshold ROP.
Subjects and Methods
Institutional Review Board approval was obtained to perform a retrospective study of patients who were enrolled in fetal surgery studies at our institution. We reviewed the medical records of 137 patients who underwent open fetal surgery (71 patients) or fetoscopic surgery (66 patients) from 1996 to 2004 at our institution. Surgical indications included MMC, CDH, SCT, CCAM, TTTS, and twin reversed arterial perfusion (TRAP). Of these 137 patients, 17 patients had ROP examination data at our institution (see Table 1). ROP was staged according to the International Classification of Retinopathy of Prematurity.15,16
Fetal surgery patients with local retinopathy of prematurity examination data.

Rates of ROP in our cohort of fetal/fetoscopic surgery patients with ROP examination data were compared with published rates in the two largest cohorts of patients with similar demographics in the same time period as our study.17,18 Binomial tests were performed to determine p-values and evaluate whether the rate differences were significant.
Results
The 71 patients who underwent open fetal surgery at our institution had a mean gestational age at surgery of 23 6 /7 ± 2 5 /7 weeks (range = 20 6 /7–35 3 /7 weeks) and an mean gestational age at birth of 34 3 /7 ± 3 1 /7 weeks (range = 24 3 /7–40 weeks). Of the open fetal surgery patients, 87% were born prematurely (<37 weeks gestational age), compared to 12% of the general population, and 19% were born at gestational ages ≤32 weeks, compared to 1.9% of the general population (200 1 data from the National Center for Health Statistics). The 66 patients who underwent fetoscopic surgery at our institution had a mean gestational age at surgery of 21 4 /7 ± 2 3 /7 weeks (range = 16 1 /7-26 5 /7 weeks) and an mean gestational age at birth of 34 ± 4 2 /7 weeks (range = 26–42 3 /7 weeks). Of the fetoscopic surgery patients, 73% were born prematurely, and 31% were born at gestational ages ≤32 weeks.
Of the 17 patients with ROP examination data at our institution, the mean gestational age at surgery was 23 4 /7 ± 2 3 /7 weeks (range = 18 4 /7-27 weeks), mean gestational age at birth was 30 ± 2 5 /7 weeks (24 3 /7–36 1 /7 weeks), and mean birth weight was 1449 ± 510 g (610–2485 g). The average ROP at initial screening was Immature, Zone 2 (Table 1). Follow-up data to retinal maturity was only available in 12 of the 17 patients. The incidence of ROP was 40% (6/15)–-two patients were transferred prior to development of ROP or retinal maturity. Of those with complete examination data, the incidence of threshold ROP was 8.3% (1/12) overall, and 33% (1/3) of those with ROP had threshold ROP.
Lad, et al evaluated the largest known cohort of newborns in the United States for incidence of ROP using The National Inpatient Sample, a representative sample of all U.S. hospital discharges from 1997 to 2002. 17 In this study, newborns with a length of stay >14 days were looked at for incidence of ROP. Of those infants <1500 g, 10.45% (24,198/231,527) had ROP, compared to 0.22% (3000/1,384,641) of those weighing ≥1500 g. Of all the infants with ROP, 7.7% (2112/27,43 5) underwent laser photocoagulation and 0.13% (35/27,435) had scleral buckle or pars plana vitrectomy. 17 In New York state, between the years 1996 and 2000, the incidence of ROP in a large cohort of newborns with a length of stay >28 days and <1500 g was found to be 20.3% (2152/10,596), and for those 1500–2500 g was 3.6% (131/3645). 18 Of all newborns with ROP, incidence of threshold ROP was 10.1% (230/2284): 9.5% (218/2284) requiring laser and 0.5% (12/2284) requiring sclera buckle or vitrectomy. 18 To our knowledge, this was the second largest cohort of newborns evaluated for incidence of ROP in the United States in recent years. Both of these studies included a demographic population similar to ours, evaluated over a similar time period. The overall incidence of ROP in our cohort was high, at 40%. Among those <1500 g, 57% had ROP (4/7; one patient was transferred prior to development of ROP or retinal maturity), a significantly higher rate than the rates of 10.5% (p = 2.2 × 10–4) and 20.3% (p = 0.005) in the above studies. The incidence of ROP among infants ≥1500 g was 28.6% (2/7). This is significantly higher than the 0.22% (p = 3.5 × 1 from the National Inpatient Sample study 16 or the 3.6% (p = 1.5 × 10–3) incidence of ROP in babies 1500–2500 g from the New York study. 17 Among those patients with ROP for whom we have complete follow-up data, the incidence of threshold disease was 33% (1 of 3 patients), which is significantly higher than the roughly 7.8% (p = 0.017) incidence of threshold ROP among all infants with ROP in the National Inpatient Sample study 17 or the 10.1% in the New York study (p = 0.028). 18
Eight of 17 patients would have been examined using a screening criterion of <1500 g. Two patients with birth weights ≥1500 g developed ROP but did not reach threshold (patients 11 and 15). One of these, patient 15, is actually large for gestational age (LGA), with a weight >90th percentile for gestational age, according to the Fenton Fetal-Infant Growth Chart for Preterm Infants. 19 Fifteen of 17 patients would have been examined with a screening criterion of gestational age at birth ≤32 weeks. One patient with gestational age at birth >32 weeks and birth weight >1500 g was examined and did not develop any stage of ROP (patient 16).
The five TTTS patients had an average gestational age at surgery of 25 5 /7 weeks, an average gestational age at birth of 29 3 /7 weeks, and average birth weight of 1153g. Four of the five were donor twins with an average birth weight of 1050 g. One donor twin reached Stage 3 (patient 2) and another donor reached threshold ROP and was treated by laser (patient 1). The average gestational age at birth for these two infants was 28 weeks and the average birth weight was 680 g. Both of these infants were small for gestational age (SGA), with weights <10th percentile for gestational age according to the Fenton Fetal-Infant Growth Chart for Preterm Infants. 19
Discussion
Based on our small series, fetal surgery patients appear to be at significantly increased risk for ROP and at significantly increased risk for threshold ROP compared to large published cohorts of populations with similar demographics over a similar time period.17,18 This may be due to any number of factors that the fetus may encounter during surgery, such as reduced oxygen delivery, light exposure, physiologic stress, and/or other environmental changes that might upregulate angiogenic factors such as VEGF or cause other biologic changes that result in ROP. It is important to note, however, that the published cohorts that were used for comparison of ROP and threshold ROP rates might underestimate the background risk of ROP. The National Inpatient Sample study and the New York study both calculated rates of ROP among newborns of any age, not necessarily premature infants, and used the length of stay of >14 days or >28 days to help ensure that primarily premature infants were included.17,18
While our sample size was small and only represented 12% of the fetal surgery patients at our institution, we observed that the two patients with the worst ROP, TTTS donor twins, also had the smallest birth weights and were small for gestational age. The severity of ROP witnessed in these infants is consistent with existing evidence that the lower the birth weight, the greater the risk for ROP 20 Additionally, SGA infants have significantly increased risk for severe ROP 21 It is interesting to note, however, that one patient in our cohort (patient 15) was LGA and still developed ROP, though it regressed. Perhaps undergoing open fetal surgery caused undise stress that encouraged the development of ROP, but the large size of the baby was protective, promoting regression.
Our data demonstrate that the current screening guidelines at our institution for ROP examination of babies with birth weights <1500 g and gestational age ≤32 weeks would adequately cover the at-risk patients who undergo fetal surgery. A greater percentage of fetoscopic patients compared to open fetal surgical patients were born at ≤32 weeks gestational age and would have been screened for ROP. In addition, the average time in utero was slightly longer in open fetal surgical patients as compared to fetoscopic patients (34 3 /7 weeks compared to 34 weeks). From our sample of patients with ROP data, 4/7 (57%) of the fetoscopic patients developed some level of ROP, whereas 2/10 (20%) of the open fetal surgery patients developed some level of ROP. All of these data suggest that the invasiveness of the surgery may not affect the likelihood of ROP development.
This study's small numbers were due to transfers to other centers prior to initial ROP screening. Larger studies need to be done in order to confirm our findings that fetal surgery confers a significantly increased risk for ROP and threshold ROP. ROP examiners should be aware that these at-risk fetal/fetoscopic surgery patients may present in their screening population.
Disclosure
The authors report no conflicts of interest.
Footnotes
Acknowledgement
Presented in part as a scientific poster at the 2005 American Association of Pediatric Ophthalmology and Strabismus Annual Meeting in Orlando, Florida.