
Abstract
Aim
To assess plasma Zn and Cu levels in individuals with depression.
Subjects and Methods
Plasma from 73 clinically depressed individuals, 38 individuals with anxiety and 16 controls were tested for plasma Zn and Cu concentration using inductively-coupled plasma-mass spectrometry.
Results
Depressed individuals, with and without secondary anxiety, had decreased plasma Zn and elevated plasma Cu compared to controls. Zn normalized (increased to the level of normal controls) but Cu increased in individuals with depression (with and without secondary anxiety), after Zn therapy, whereas both plasma Zn increased and Cu levels decreased in anxiety, with and without secondary depression, after Zn therapy. Individuals with depression, with and without secondary anxiety, had significantly higher symptom severity when compared to neurotypical controls. Symptom severity in individuals with anxiety (both with and without secondary depression) significantly decreased after Zn therapy, whereas symptoms remained the same in individuals with primary depression.
Discussion
These data show an association between Zn and Cu plasma levels and clinically depressed individuals, and suggest that high Cu levels are associated with high symptom severity.
Keywords
Introduction
Clinical depression is a considerable public health problem. 1 Approximately 32 to 35 million adults in the United States have experienced depression at some point in their life, and approximately 13 million adults have experienced depression within the pastyear. 2 It is also a considerable medical problem, as those with major depressive disorder (MDD) are at increased risk for serious medical illness, including cardiovascular disease,3–5 diabetes,6–8 cancer,9–11 and stroke. 12
Zn has a unique and extensive role in biological processes. Since the discovery of this element as an essential nutrient forliving organisms,13–15 many diverse biochemical roles for it have been identified. These include roles in enzyme function, 16 nucleic acid metabolism,17,18 cell signaling 19 and apoptosis. 20 Zn is also essential for physiological processes including growth and development, 21 lipid metabolism, 22 brain and immune function.21,23
Dietary factors that reduce the availability of Zn are the most common cause of Zn deficiency. However, inherited defects can also result in reduced Zn. Both nutritional and inherited Zn deficiency produce similar symptoms, such as dermatitis, diarrhea, alopecia and loss of appetite, 24 with more prolonged deficiency, causing growth impairment and neuropsychological changes such as emotional instability, irritability and depression.25–28
Low intracellular Zn has been found to be associated with DNA damage, oxidative stress, antioxidant defenses, and DNA repair,29,30 and decreased Zn has also been found to be a potential marker of treatment resistant depression and of the immune/inflammatory response in depression. 35 There is evidence to suggest Zn may serve as an important anti-oxidant. 31
Abnormal Cu levels have also been associated with depression. 32 As an example, patients with high Cu associated with Wilson's disease often are depressed, 33 and serum Cu has been suggested as a “trait marker” (remains constant regardless of successful treatment) of unipolar depression. 34
Because of the potential association between Zn and Cu and clinical depression, we tested depression patients for plasma concentration of these essential elements and compared these results to perceived symptom severity.
Materials and Methods
Subjects
Experimental and controls
Plasma from individuals with diagnosed clinical depression (n = 73; 36 male; mean age 38 years) and controls (n = 16; 7 male; mean age 42 years) was obtained from patients presenting consecutively at the Health Research Institute/Pfeiffer Treatment Center*, Warrenville, Illinois. Most of these individuals were diagnosed using The Hamilton Rating Scale for Depression before presenting for treatment.
The Pfeiffer Treatment Center is a comprehensive treatment and research center, specializing in the care of with neurological disorders, including Depression.
Patient consent was obtained from all patients involved in this study and this study was approved by the IRB of the Health Research Institute/Pfeiffer Treatment Center.
Severity of disease
Modified Hamilton Scales were used to determine the severity of depression or anxiety. Patients were asked to rate their depressive (or anxiety) behavior such as; irritability and anger, lack of ability to focus/concentrate, racing thoughts, trouble sleeping, light sensitivity, migraines, OCD behavior, intrusive thoughts, overall depression, disorganization, panic, obsessive behavior, and overall anxiety. The patients were rated on a scale of 0-5 (5 being the most severe) for each of these behaviors. We evaluated the overall severity of depression behavior by establishing the mean of all of the scores for each patient.
Zn and Anti-Oxidant Therapy
Individuals in this study who presented to the Pfeiffer Treatment Center with depression (or anxiety) were tested for Zn, Cu and anti-oxidant levels. Based on deficiencies, they were then prescribed the appropriate dose of anti-oxidants. Pre-therapy patients represent those who were tested when they first presented and were not previously taking any Zn or anti-oxidants. Post-Therapy patients received anti-oxidant therapy (Vitamin C, E, B-6 as well as Magnesium, and Manganese if warranted), and Zn supplementation (as Znpicolinate), daily, for a minimum of 8 weeks.
Plasma
All experimental and control plasmas were treated in an identical fashion—refrigerated (4 C) immediately after collection and cell/serum separation, then used within 4 hours for inductively-coupled plasma-mass spectrometry.
Cu and Zn serum concentration
Cu and Zn plasma concentration was performed by LabCorp, Inc. (Naperville, IL 60563) using inductively-coupled plasma-mass spectrometry, as previously described. 51
Statistics
Inferential statistics were derived from t-test with 95% confidence intervals and ANOVA analysis when variance of three or more groups was warranted.
Results
Serum from 73 clinically depressed individuals, 38 individuals with anxiety and 16 neurotypical controls were tested for serum Zn and Cu using inductively-coupled plasma-mass spectrometry.
Depressed individuals with secondary anxiety (N = 48) and without secondary anxiety (N = 25) had significantly lower plasma levels of Zn (P = 0.02; P = 0.02, respectively) (Fig. 1) and depressed individuals with secondary anxiety and without secondary anxiety had elevated Cu compared to controls (P = 0.003; P = 0.03, respectively) (Fig. 2).
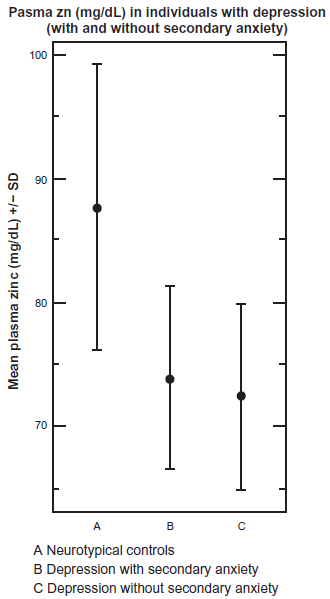
Depressed individuals with secondary anxiety (P = 0.02) and without secondary anxiety (P = 0.02) had significantly lower plasma levels of zinc.

Depressed individuals with secondary anxiety (P = 0.003) and without secondary anxiety (P = 0.03) elevated Cu compared to controls.
Individuals with anxiety and secondary depression (N = 18) and without secondary depression (N = 20) had lower plasma levels of Zn (P = 0.05; P = 0.08, respectively) (Fig. 8), and individuals with anxiety and secondary depression and without secondary depression had elevated Cu compared to controls (P = 0.10; P = 0.02, respectively) (Fig. 7).
Plasma Zn normalized (increased to the level of normal controls) (P = 0.011) but Cu plasma concentration increased (instead of decreased) in individuals with depression (with and without secondary anxiety), after Zn therapy (Fig. 4).

As expected, individuals with depression and secondary anxiety (P = 0.002) and without secondary anxiety (P = 0.003) had significantly higher symptom severity when compared to neurotypical controls.

Plasma zinc normalized (increased to the level of normal controls) (P = 0.011) but copper plasma concentration increased in individuals with depression (with and without secondary anxiety, after zinc therapy.
Whereas both plasma Zn increased (P = 0.001), and Cu levels decreased (although not significantly; P = 0.15) in anxiety, with (N =18) and without (N = 20) secondary depression, after Zn therapy (Fig. 5), it should be noted that controls did not receive the same Zn and anti-oxidant therapy as the patients. Baseline control data is shown on Figures 7 and 8.
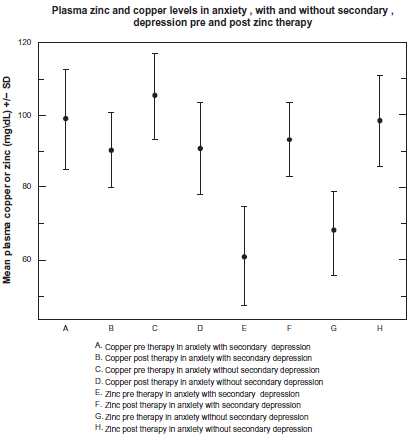
Plasma zinc increased (P = 0.001) and copper levels decreased in anxiety, with and without secondary depression, after zinc therapy.
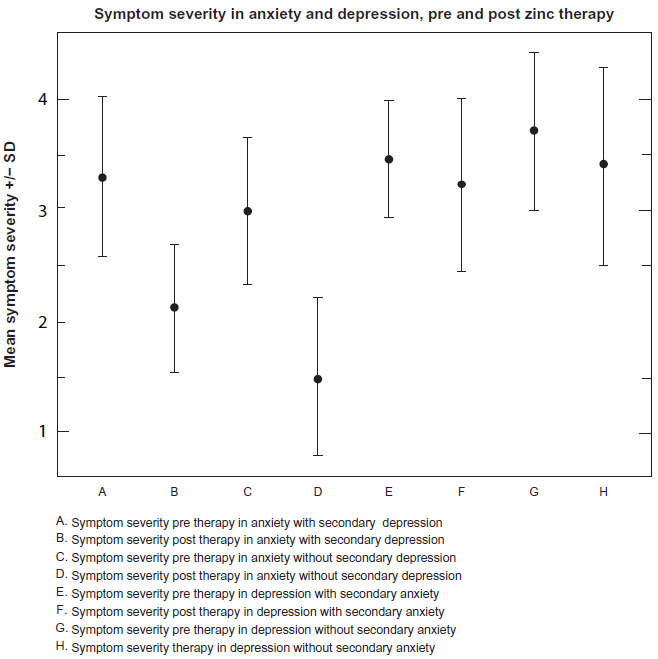
Symptom severity decreases significantly in anxiety groups after zinc therapy, but not in depression groups (P = 0.0002).

Plasma copper is higher than controls in individuals with anxiety (with and without secondary depression).

Plasma zinc is lower than controls in individuals with anxiety (with and without secondary depression).
Individuals with depression and secondary anxiety (P = 0.002) and without secondary anxiety (P = 0.003) had significantly higher symptom severity when compared to neurotypical controls (Fig. 3), whereas symptom severity of anxiety patients, before therapy, was similar to controls (Fig. 9).

Symptom severity in individuals with anxiety is similar to controls.
Symptom severity in individuals with anxiety (both with and without secondary depression) significantly decreased after Zn therapy (P = 0.0002), whereas symptoms remained the same in individuals with depression (Fig. 6).
Discussion
Major depressive disorder has been found to be associated with oxidative stress, 36 which correlates with severity of depression. 37 There is also much support for the role of GABA and glutamate in mood disorders, particularly anxiety and depression.38,39
Zn has been found to be associated with GABA and glutamate regulation, particularly through anxiolytic activity, modulating GABAergic inhibition and seizure susceptibility,40–42 and deficiency of Zn has been found to be associated with GABAergic impairment. 43
Dietary Zn deficiency is associated with a variety of physiological defects, including anorexia, skin lesion, and growth retardation. 44 Mechanistic studies have demonstrated that Zn deficiency affects a large number of hepatic genes involved in multiple cellular functions, including gene expression of metallothionein (MT), insulin-like growth factor I (IGF-I), insulin-like growth factor binding protein 1 (IGFBP1), cyclin D1, and HGF, which are involved in cell proliferation.45–47
Cu has been found to be a potent inhibitor of GABA-evoked responses, particularly in Purkinje cells. Cu toxicity, notably in Wilson's disease, could result, to some extent, from chronic GABAA receptor blockade. 48 Data strongly suggest that Cu and Zn might interact with each other with GABAA receptor complex and participate in modulation of synaptic transmission. 49
We previously reported that depressed individuals have significantly lower oxidative stress after Zn therapy, 50 and individuals with anxiety (both with and without depression) have significantly higher plasma levels of Cu and lower plasma Zn compared to controls. These same patients improved significantly with respect to perceived overall symptoms after Zn and anti-oxidant therapy. 52
In individuals with primary anxiety, data in this report supports our previous findings and demonstrates that Zn and Cu levels normalize (increase or decrease to levels of normal controls) after Zn and anti-oxidant therapy and perceived symptoms significantly improve. However, in individuals with primary depression, after the same therapy, Zn levels normalize, but Cu levels do not, and perceived symptoms do not significantly improve. This suggests that normalization of Cu levels may be important in helping to improve depression symptoms. It is unclear why Cu levels remain high after Zn therapy in depressed individuals, however it is possible that this is due to dysfunctional carriers like metallothionein.
We suggest that the low Zn and high Cu may modulate GABA, ultimately causing a lowering of transmitter concentration. Post Zn therapy, it is possible that increased Zn and decreased Cu cause an increase in GABA, which relieves symptoms. In depressed individuals, when Cu levels remain high after Zn therapy, symptoms also remain high, possibly due to higher GABA levels. To evaluate this relationship, future studies will assess more patients with depression and evaluate GABA concentration along with Cu and Zn levels.
Disclosure
This manuscript has been read and approved by the author. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The author and peer reviewers of this paper report no conflicts of interest. The author confirms that they have permission to reproduce any copyrighted material.