
Abstract
Purpose
To assess the safety and efficacy of gadoxetate disodium-enhanced liver MR imaging in pediatric patients.
Material and Methods
Retrospective, multicenter study including pediatric patients aged >2 months to <18 years who underwent contrast-enhanced liver MRI due to focal liver lesions. A single intravenous bolus injection of 0.025 to 0.05 mmol/kg body weight of gadoxetate disodium was administered. Adverse events (AEs) up to 24 hours after injection were recorded and a one-year follow-up was conducted for all serious and unexpected AEs. Efficacy was defined based on the additional diagnostic information obtained from the combined (pre- and postcontrast) image sets as compared with the precontrast image sets by blinded reading.
Results
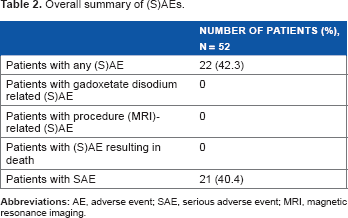
A total of 52 patients for safety and 51 patients for efficacy analyses were evaluated. Twenty-two patients (42.3%) reported a total of 51 serious AEs (SAEs) and one AE after one year. No SAE or AE was related to gadoxetate disodium injection. Gadoxetate disodium-related effects on vital signs were not seen. Additional diagnostic information was obtained for 86.3% of patients. The three most improved efficacy variables were lesion-to-background contrast, lesion characterization, and improved border delineation in 78.4%, 76.5%, and 70.6% of patients, respectively.
Conclusion
Gadoxetate disodium in pediatric patients did not raise any clinically significant safety concern. Contrast enhancement provided additional clinically relevant information.
Introduction
Gadoxetate disodium (Gadoxetic acid [Gd-EOB-DTPA]) is a gadolinium-based contrast agent (GBCA) used in MRI that combines features of both an extracellular contrast agent and a hepatocyte-specific agent. It has been specifically developed for the detection, localization, and characterization of liver lesions (lesion type diagnosis), for example, metastases, hepatocellular carcinomas, focal nodular hyperplasia, and hemangiomas. Its particular strength was shown for small hepatic lesions with a diameter <1 cm. 1 Therefore, gadoxetate disodium has the potential to improve diagnosis and assist surgical planning.2–4 Gadoxetate disodium belongs to the class of linear ionic GBCAs and features a high T1 relaxivity of 6.9 L mmol -1 s-1 (at 1.5 T in plasma). 5 After intravenous administration, gadoxetate disodium is first distributed in the extracellular space and then quickly taken up by the hepatocytes, thus enabling both dynamic and hepatocyte-specific imaging. In healthy subjects, about 50% of the injected dose is excreted via the kidneys and 50% via the hepato-biliary system. Contrast enhancement of the liver parenchyma and liver-to-lesion contrast is highest at about 20 minutes after administration, with a plateau lasting for at least up to 45 minutes postinjection. 6
The excellent safety profile of gadoxetate disodium in adults (>18 years)1,7,8 has been demonstrated in several (controlled) clinical studies and in post-marketing experience. 9 So far, since approval in March 2004, more than 2.7 million patients have been exposed to gadoxetate disodium worldwide (according to Bayer internal sales reporting).
In pediatric patients, liver diseases are generally diffuse rather than focal. These liver diseases/disorders include biliary atresia, different forms of viral hepatitis, metabolic liver diseases, intrahepatic cholestasis, autoimmune liver disease, and tumors. 10 Tumors (either benign or malignant) and metastases can occur in the liver in pediatric subjects; however, they constitute a rare disease entity.10–12 In the United States, there are approximately 150 new pediatric cases of hepatoblastomas per year. 13 Malignant tumors such as hepatoblastoma account for approximately two-thirds of the liver tumors in children. 13 Generally, liver tumors are highly heterogeneous and distinct from adult liver pathology, as are surgical approaches. Better definition of liver pathology and anatomy with novel imaging modalities can help clinicians to manage such pediatric patients optimally by improving diagnostics and resolution of tumor/normal tissue anatomical relationships.
Thus far, gadoxetate disodium has been systematically investigated only in adults. The aim of this study was to assess the safety and efficacy of gadoxetate disodium–enhanced MRI in a pediatric population, prompted by a request in the FDA's approval letter in July 2008. 14
Material and Methods
Study design
We performed a retrospective, multicenter study in seven centers in four countries (United States [three centers], Italy [two centers], Japan, and Taiwan [one center each]). The enrollment period lasted from December 2009 to April 2013. The aim of this study was to assess the safety and efficacy of gadoxetate disodium–enhanced liver imaging in pediatric patients.
Study population
Our study population consisted of 52 pediatric subjects (>2 months and <18 years of age), who underwent a contrast-enhanced liver MRI with gadoxetate disodium because of suspected or known focal liver lesions. Diffuse liver disease was not an indication. Patients eligible for our study had to have well-documented safety and efficacy data, precontrast, and postcontrast MRI. We attempted to include an equal distribution of patients in the following three age groups: infants (>2 months to ≤2 years), children (>2 to ≤12 years), and adolescents (>12 years to <18 years).
We conducted the study in accordance with all guidelines set forth by the sites’ approving institutional review boards. The ethical principles laid out in the Declaration of Helsinki and the International Conference on Harmonization guideline E6: Good Clinical Practice were respected. Informed consent was obtained from the patients or their legally authorized representatives prior to data retrieval.
Treatment
All patients received a single intravenous bolus injection of 0.025 to 0.05 mmol/kg (0.1–0.2 mL/kg) body weight (BW) gadoxetate disodium (Primovist®/Eovist®; Bayer HealthCare AG, D-51368 Leverkusen, Germany) followed by a saline flush. All procedures were done in the framework of the clinically routine diagnostic workup. Gadoxetate disodium is marketed in all participating countries and was purchased locally by the centers at hospital pharmacies.
Target variables
Safety was determined based on adverse events (AEs), laboratory test results (hematology, serum chemistry parameters, glomerular filtration rate), physical examinations, and vital signs. We analyzed all documented AEs up to 24 hours after gadoxetate disodium injection and all AEs that were serious and unexpected up to 1 year after injection.
For AEs and SAEs, the definitions set forth by the ICH Harmonized Tripartite E2D Guideline (Post-Approval Safety Data Management: Definitions and Standards for Expedited Reporting) were applied. 15
The primary efficacy variable was the additional diagnostic information obtained from the combined (precontrast and postcontrast) image sets versus the precontrast image sets. We recorded and analyzed the following parameters: (1) change in number of lesions (fewer/equal/more); (2) improved border delineation of the primary lesion (yes/no); (3) increased contrast of primary lesion vs background (yes/no); (4) change in the size of the primary lesion (larger/no change/smaller); (5) change in information about lesion characterization (improved/unchanged/worsened).
Secondary efficacy variables, based on the comparison of combined (precontrast and postcontrast) versus precontrast image sets and final diagnosis were (1) change in diagnosis; (2) change in confidence of diagnosis; (3) change in the number of nonmalignant lesions; (4) change in the number of malignant lesions; and (5) change in the recommended next step of patient management/therapy.
Sensitivity, specificity, and accuracy were the parameters for lesion classification. For the precontrast as well as the combined (precontrast and postcontrast) images, the percentage of patients with true positive diagnoses and true negative diagnoses (ie, sensitivity and specificity) and the accuracy of diagnoses were calculated. A malignant diagnosis of the precontrast (or the combined precontrast and postcontrast) images was true positive if the final diagnosis was “malignant.” Similarly, a benign diagnosis of the precontrast (or the combined precontrast and postcontrast) images was true negative if the final diagnosis was “benign.” We used the final diagnosis mentioned in the patients’ medical records as standard of truth (SoT), which was derived by biopsy or biopsy plus surgery (lesion histology assessed by pathology).
Study procedures
As this was a retrospective study, the safety information requested in the study protocol was captured from the patients’ medical records and entered in electronic case report forms (eCRFs). We recorded the following variables: demographics, indication for liver MRI, gadoxetate disodium dose, final diagnosis, details on AEs up to 24 hours after injection, details up to one year after gadoxetate disodium injection for all AEs that were serious and unexpected and for SAEs occurring during the one-year follow-up monitoring until resolution. In addition, medical history, concomitant medication, laboratory parameters (including estimated glomerular filtration rate [eGFR]), physical examination results, and vital signs were captured.
Efficacy variables were assessed by a radiologist (O.E.O.), who was an independent certified radiologist not affiliated with any of the clinical sites and with over 12 years of experience.
Anonymous digital copies of the MR images in the DICOM format were taken from the medical records and were provided in random order to the blinded reader for evaluation. The blinded read was carried out as follows. For each subject, first the precontrast images were evaluated and results were saved and locked. After this first step, the postcontrast images were added and displayed together with the precontrast images for the combined evaluation by the reader.
Image sets from the following MR techniques were evaluated: precontrast T1, postcontrast dynamic T1, postcontrast steady-state T1, and any other precontrast or postcontrast images (eg T2 weighted).
Statistics and sample size
As this study was a postmarketing requirement, the sample size of n = 50 was specified by the FDA when gadoxetate disodium was approved in the United States. 14 We performed efficacy and safety analyses on the full analysis set, that is, on patients who received any amount of gadoxetate disodium.
Available data, mean, standard deviation, median, and minimum and maximum frequency were calculated for quantitative variables. For qualitative variables, we generated frequency tables. Confidence intervals (CIs) of up to 95% are provided for parameters of the primary efficacy variable. For statistical evaluation, we used the software package SAS release 9.1.
Results
Demographics.

Height, weight, and race were not provided for all patients.
Safety
Overall summary of (S)AEs.
(S)AEs by system organ class.
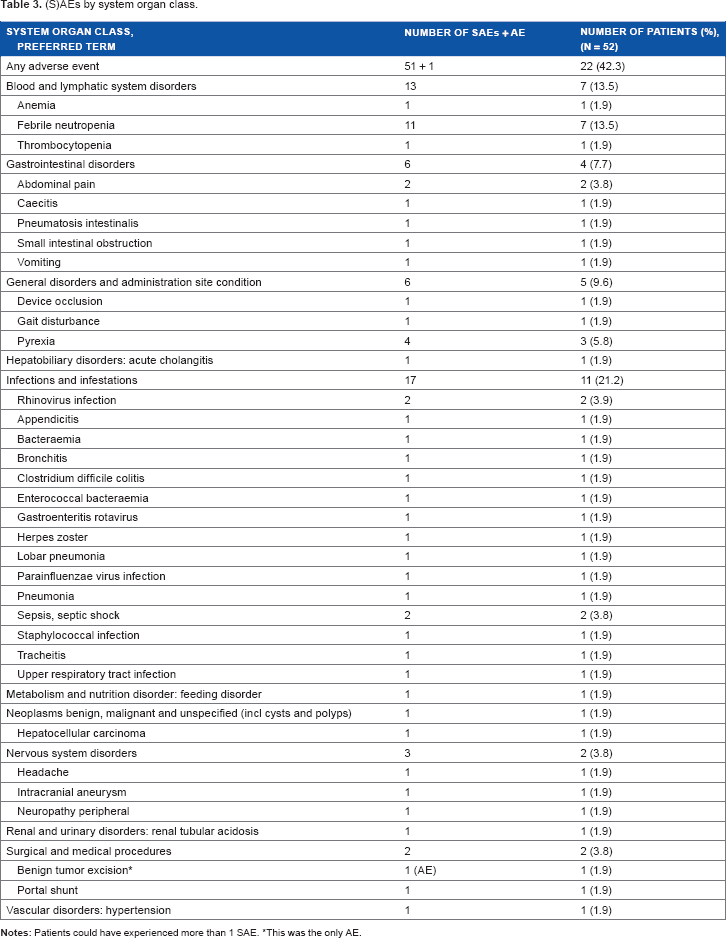
This was the only AE.
Eleven of 14 patients (78.6%) age >2 months to ≤2 years, 8/25 patients (32%) age >2 years to ≤12 years, and 2/13 patients (15.4%) age >12 years to <18 years experienced an SAE, likely reflecting the underlying diseases.
With the exception of one case (hepatocellular carcinoma), all patients recovered from their SAEs.
We did not see any clinically notable effects on vital signs in 30 patients who had both preinjection and postinjection assessments. There were no clinically notable effects on hematology and routine blood chemistry parameters following gadoxetate disodium injection in the eight patients who had both preinjection and postinjection assessments for at least one laboratory parameter.
Efficacy
Primary efficacy variable: additional diagnostic information (combined precontrast/postcontrast images vs precontrast images).
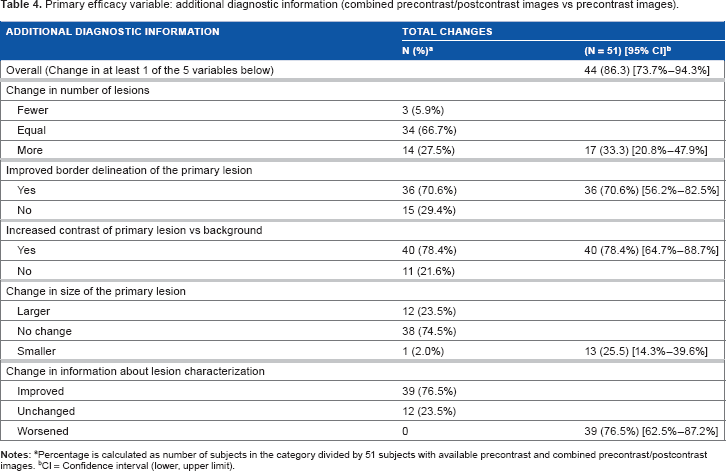
Percentage is calculated as number of subjects in the category divided by 51 subjects with available precontrast and combined precontrast/postcontrast images.
CI = Confidence interval (lower, upper limit).
Secondary efficacy variables
Secondary efficacy variables (combined precontrast and postcontrast MRI vs precontrast MRI).
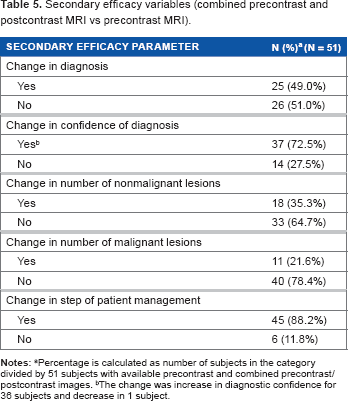
Percentage is calculated as number of subjects in the category divided by 51 subjects with available precontrast and combined precontrast/ postcontrast images.
The change was increase in diagnostic confidence for 36 subjects and decrease in 1 subject.
Sensitivity of lesion classification was 70.8% for the combined (precontrast and postcontrast) vs 66.7% for the precontrast MRI; specificity was 66.7% vs 88.9% and accuracy was 68.6% vs 78.4%, respectively. There were six more false-positive diagnoses for combined (precontrast and postcontrast) imaging: For three patients, the final diagnosis was focal nodular hyperplasia and for one patient each, the final diagnosis was benign tumor, telangiectasia, or suspected hepatic angioma. For these patients, the blinded reader diagnosed either metastases or malignant tumors. For three patients, both precontrast and postcontrast MRI procedures were false positive. The final diagnoses for these three patients were biliary atresia, atypical hepatocellular lesion consistent with at least high-grade dysplastic nodule, and focal nodular hyperplasia.
Discussion
To the best of our knowledge, this is the first systematic evaluation of the safety and efficacy of gadoxetate disodium in a pediatric population. Contrast-enhanced liver imaging with gadoxetate disodium did not raise any safety concern, and additional clinically relevant information was noted from postcontrast imaging.
Contrast-enhanced liver MRI in pediatric populations is increasingly used to help with the clinical management of children and adolescents with a wide range of liver disease. In response to a request by the FDA specific to this initiative, a sample size of n = 50 14 was to be accrued covering the age range from >2 months to <18 years. This population represents a diverse ethnic background accrued in three separate continents, suggesting that our study population is a fair representation of relevant age groups in a pediatric population.
Overall, gadoxetate disodium up to a dose of 0.2 mL/kg BW (0.05 mmol/kg BW) was well tolerated in our cohort, with no (S)AE attributed to the study drug or injection process. Safety data on gadoxetate disodium in children are extremely scarce in the literature, although this agent is becoming more widely used in this age group. 16 Meyers et al recently summarized their experience in hepatoblastoma imaging. They did not record any adverse event in more than 120 administrations in their pediatric population. 16 Also, in two case reports, one on a six-year-old and one on a nine-year-old boy, no immediate adverse effects of the contrast, neither clinically nor biochemically, were seen.17,18 Tamrazi et al as well as Kolbe et al used gadoxetate disodium in 22 and 112 pediatric patients, respectively. However, these authors focused on a variety of efficacy parameters but did not report on safety or tolerability.19,20 The same holds true for a series of patients aged 11–78 years with hepatocellular adenoma or focal nodular hyperplasia reported by Grazioli et al. 21
Since approval in March 2004, more than 2.7 million patients have been exposed to gadoxetate disodium worldwide. Of these, according to market research data, less than 0.1%, or between 1,000 and 2,000 patients are estimated to have been below the age of 18. 22 As of March 26, 2015, the Global Pharmacovigilance Department of the manufacturer has received three spontaneous postmarketing reports of AEs occurring in patients <18 years (16-year-old: vomiting; 15 year old: dyspnea; 9-year-old: anaphylactoid reaction). 23 These AEs are consistent with those reported in adults and with other GBCAs. No safety concerns unique to the pediatric population were identified.
Additional diagnostic information was obtained for 86.3% of patients receiving gadoxetate disodium in our cohort. The three most improved variables were lesion-to-background contrast, lesion characterization, and improved border delineation. Similar to safety, efficacy studies with gadoxetate disodium in the pediatric population are scarce. Altogether, our findings are in line with Meyers et al who described their pediatric MRI protocol for differential diagnosis of a broad variety of liver lesions. They found gadoxetate disodium useful in the evaluation of pediatric liver lesions, particularly in the differentiation of focal nodular hyperplasia (FNH) from metastases, the sharp distinction of tumor from normal liver parenchyma, and the clear delineation of tumor margin with respect to the biliary tree. In conclusion, they stated that gadoxetate disodium has the potential to improve characterization and staging of pediatric liver masses. 24
In our study, we recorded a change in diagnosis and/or a change in the next step of patient management in 49.0% and 88.2% of patients, respectively. In their study on hepatoblastoma imaging with gadoxetate disodium enhanced MRI, Meyers et al suggested that identification of subtle satellite lesions had the potential to substantially impact both medical and surgical treatment approaches. Moreover, contrast-enhanced liver MRI helps to differentiate FNH from recurrent typical hepatoblastoma. 16 Also, Kolbe et al assessed the impact of the hepatocyte phase of imaging on lesion detection, tumor staging, and diagnostic confidence in 112 patients. The addition of the hepatocyte phase of imaging significantly improved the diagnostic confidence for all patients (P < 0.0001) as well as specifically for patients diagnosed with FNH (P = 0.003). In nearly a quarter of patients, the hepatocyte phase of imaging allowed the reviewer to detect additional lesions (P = 0.005). 20 In addition to what we investigated, another group focused on functional hepatobiliary imaging. Tamrazi et al retrospectively investigated 21 children with gadoxetate disodium and looked at the clinical value gained beyond traditional noncontrast fluid-sensitive MR cholangiopancreatography and other imaging modalities. They saw benefit in cases of iatrogenic and noniatrogenic biliary strictures, perihepatic fluid collections for biliary leak, hepatobiliary dysfunction in the absence of hyperbilirubinemia, and in the functional exclusion of cystic duct occlusion that can be seen in acute cholecystitis. 19
Sensitivity for lesion classification (benign vs malignant) was 70.8% for the combined (precontrast and postcontrast) vs 66.7% for the precontrast MRI; specificity was 66.7% vs 88.9% and accuracy was 68.6% vs 78.4%, respectively. These blinded read results were not as conclusive with regard to specificity and accuracy as was observed in the large, phase 3 clinical trials in adults.1,7,25 For example, Halavaara et al reported on liver lesion classification in adults. His three blinded readers presented somewhat similar sensitivities (72.9–85.9%) but better specificity (75.9–81.9%) and accuracy (78.9–85.9%). 7 In these phase 3 clinical trials, the procedure for the MR sequences were specified in the protocol and hence, standardized. In addition, the MR images were checked for quality on an ongoing basis during the study in order to make any necessary adjustments to increase the quality of the images. In this retrospective study, the MRI had been completed previously, and the authors had no control over the quality of the images or standardization of the image acquisition. Although the minimum set of images specified in the protocol were available, not all subjects had a complete set of pre- and postcontrast (arterial, portovenous, equilibrium, and steady stage phases) images necessary for establishing a diagnosis.
Finally, this small study was designed to have one blinded central radiological reviewer who did not have any clinical information, and as such, efficacy results from this study could be impacted by such somewhat “experimental” setting.
We acknowledge three limitations of our study. (1) The sample size of n = 52 (as specified by the FDA) was rather small and not based on a statistical rationale. In addition, only children with focal liver lesions but not diffuse liver disease were requested by the FDA and this made recruitment extremely difficult. However, the population appears to represent a diverse array of pediatric and adolescent patients of various backgrounds, and thus is a decent representation of liver pathology in this age group. (2) Our study retrospectively analyzed cases of gadoxetate disodium–enhanced liver MRI in routine clinical use. Retrospective trials present the potential for selection bias and lack of compulsory data collection such as vital signs and laboratory evaluation within 24 hours of injection. This means, in contrast to prospective studies, onsite staff are not specially sensitized to pay attention to AEs and to record them. Nonetheless, the lack of any side effects is encouraging. (3) Finally, limiting our radiological efficacy review to a single, central, blinded reviewer could have impacted our secondary efficacy endpoints compared to evaluation with a panel of expert reviewers.
In conclusion, Gadoxetate disodium in pediatric patients did not raise any clinically significant safety concern. Contrast enhancement provided additional clinically relevant information for diagnosis and patient management.
Author Contributions
Conceived and designed the experiments: JG, FK. Analyzed the data: FK, JG, JE. Wrote the first draft of the manuscript: JE, JG. Contributed to the writing of the manuscript: JG, MK, MM, AS, FK, JE. Agree with manuscript results and conclusions: JG, MK, MM, AS, FK, JE. Jointly developed the structure and arguments for the paper: JE, JG, FK. Made critical revisions and approved final version: JG, MK, MM, AS, FK, JE. All authors reviewed and approved the final manuscript.
Footnotes
Acknowledgments
We thank the patients and families for their cooperation and the staff in the centers for allowing us to retrieve all the documents on the enrolled patients.