
Abstract
Purpose
Contrast-enhanced magnetic resonance imaging (MRI) of the central nervous system (CNS) with gadolinium-based contrast agents (GBCAs) is standard of care for CNS imaging and diagnosis because of the visualization of lesions that cause blood–brain barrier breakdown. Gadobutrol is a macrocyclic GBCA with high concentration and high relaxivity. The objective of this study was to compare the safety and efficacy of gadobutrol 1.0 M vs unenhanced imaging and vs the approved macrocyclic agent gadoteridol 0.5 M at a dose of 0.1 mmol/kg bodyweight.
Materials and Methods
Prospective, multicenter, double-blind, crossover trial in patients who underwent unenhanced MRI followed by enhanced imaging with gadobutrol or gadoteridol. Three blinded readers assessed the magnetic resonance images. The primary efficacy variables included number of lesions detected, degree of lesion contrast-enhancement, lesion border delineation, and lesion internal morphology.
Results
Of the 402 treated patients, 390 patients received study drugs. Lesion contrast-enhancement, lesion border delineation, and lesion internal morphology were superior for combined unenhanced/gadobutrol-enhanced imaging vs unenhanced imaging (P < 0.0001 for all). Compared with gadoteridol, gadobutrol was non-inferior for all primary variables and superior for lesion contrast-enhancement, as well as sensitivity and accuracy for detection of malignant disease. The percentage of patients with at least one drug-related adverse event was similar for gadobutrol (10.0%) and gadoteridol (9.7%).
Conclusion
Gadobutrol is an effective and well-tolerated macrocyclic contrast agent for MRI of the CNS. Gadobutrol demonstrates greater contrast-enhancement and improved sensitivity and accuracy for detection of malignant disease than gadoteridol, likely because of its higher relaxivity.
Introduction
Gadolinium-based contrast agents (GBCAs) have been used in contrast-enhanced magnetic resonance imaging (MRI) for defining and characterizing intracranial and spinal lesions of the central nervous system (CNS) for more than 20 years.1–5 Normally, the blood–brain barrier prevents GBCAs from diffusing out of the vascular space into the extracellular fluid in the brain. However, many pathological conditions, such as primary or metastatic brain tumors, cause local disruption of the blood–brain barrier, allowing GBCAs to diffuse into the lesions, increasing their visual conspicuity (ie brightness on contrast-enhanced sequences). Therefore, combined unenhanced/GBCA-enhanced MRI is the gold standard for the non-invasive detection and delineation of most CNS lesions.6,7
Gadobutrol is a non-ionic, macrocyclic molecule with high kinetic stability.8,9 Gadobutrol is formulated in a 1 M concentration with an osmolarity of 1603 mOsm/kg. Gadoteridol 0.5 M is a chemically similar macrocyclic GBCA at 630 mOsm/kg, which was approved for use in CNS imaging in the USA at the time of this study.10,11 Gadobutrol is highly hydrophilic owing to the trihydroxybutyl group attached to the macrocyclic ligand. Gadobutrol has a greater T1-relaxivity than most GBCAs, including all other macrocyclic agents, which may improve the visualization of lesions.10,12,13 At 1.5 T, gadobutrol has a T1-relaxivity of 5.2 mmol/second vs 4.1 mmol/second for gadoteridol.
The objective of this trial was to evaluate the safety and efficacy of gadobutrol 0.1 mmol/kg bodyweight (BW) in contrast-enhanced MRI of CNS lesions.
Materials and Methods
Study design
This was a Phase III, prospective, multicenter, double-blind, crossover trial conducted between June 2008 and April 2009; it was designed to evaluate the safety and efficacy of combined unenhanced and gadobutrol-enhanced (combined gadobutrol) imaging vs unenhanced imaging and vs combined unenhanced and gadoteridol-enhanced (combined gadoteridol) imaging in patients referred for contrast-enhanced MRI of the CNS. The ethics committees of the participating centers granted approval of the study.
The study was conducted in accordance with the Declaration of Helsinki and International Conference on Harmonisation (Good Clinical Practice guidelines), and all patients provided written informed consent.
Patients
Men and women, aged ≥18 years referred for contrast-enhanced MRI of the CNS, based on current clinical symptoms or results of previous imaging, were recruited from 51 centers in Australia, Austria, Colombia, Germany, Japan, Switzerland, and the USA. Exclusion criteria included pregnant or breastfeeding women, history of severe allergic or anaphylactoid reaction, administration of any contrast agent within 24 hours prior to the study MRI, and underlying diseases or concomitant medications that may have interfered with efficacy or safety evaluations (ie severe cardiovascular disease, unstable angina, acute stroke [<48 hours], acute renal insufficiency, hepatorenal syndrome, or the perioperative liver transplant stage).
The final diagnosis for each patient was determined by a region/country-specific independent truth committee consisting of two experienced neurologists not affiliated with the study. All available patient-related information from referral for contrast MRI was collected for three months pre- and post-study enrollment. Study-specific MR image sets and interpretations were excluded from the truth committee evaluations. The truth panel's final diagnosis for each patient was reached by consensus using a list of >30 pre-specified CNS diagnoses, each of which was prospectively categorized as either benign or malignant (according to the 2007 World Health Organization classification of tumors of the CNS) 14 so that sensitivity, specificity, and accuracy for the detection of malignant disease could be calculated based on the standard of truth diagnosis. A majority reader (agreement of ≥2 blinded readers) diagnosis was utilized for the combined gadobutrol and the combined gadoteridol image sets.
Matching of diagnoses was performed by a computer algorithm using coded CNS diagnoses.
Contrast administration and MRI
Patients were randomized 1:1 to gadobutrol followed by gadoteridol, or gadoteridol followed by gadobutrol, which were administered by an onsite unblinded nurse or technologist, who ensured the fully blinded administration of the agent on separate days (mean time between injections 4.6 days) at the standard dose of 0.1 mmol/kg BW by single intravenous injection at a rate of 2 mL/second, followed by 20 mL 0.9% saline flush at the same rate by a power injector. No local or systemic therapy or biopsy/interventional therapeutic procedure occurred between the two MRI examinations. Patients underwent MRI with a 1.5 Tesla (T) MR system and a standard dedicated head or spine coil for imaging of respective regions. Both single-element and multi-element coils utilizing 8–32 elements were used at the multiple sites evaluated in this study. A standardized MRI protocol was used in all patients that T1-weighted (T1w) fast spin echo (SE) and transverse relaxation time (T2)-weighted (T2w) fast SE sequences, and either a fluid-attenuated inversion recovery (FLAIR) sequence for brain imaging or a short time inversion recovery (STIR) sequence for spine imaging of the unenhanced imaging protocol. For the contrast-enhanced imaging, T1w SE image acquisition was repeated following injection of the contrast agent in all patients. The same protocol was used for both MRI sessions for each patient. Quality control and assurance of the correct MR image sequences, as well as conduct of the blinded readings, were carried out at DIGIMA, the image core laboratory of Bayer Pharma AG, in Berlin, Germany.
Efficacy variables
The primary objective was to demonstrate superiority of combined gadobutrol vs unenhanced MRI for three visualization parameters (degree of lesion contrast-enhancement, lesion border delineation, and lesion internal morphology) and non-inferiority for total number of lesions. This trial was also designed to demonstrate non-inferiority vs the approved agent gadoteridol per regulatory requirements. Non-inferiority of combined gadobutrol to combined gadoteridol imaging was evaluated for all four parameters (degree of lesion contrast-enhancement, lesion border delineation, lesion internal morphology, and total number of lesions). Additional objectives to evaluate non-inferiority for combined gadobutrol vs combined gadoteridol imaging included sensitivity, specificity, and accuracy for the detection of malignant CNS lesions, and image quality based on direct paired comparison (based on T1w images only). The primary efficacy analysis was based on lesion/normal structure visualization scores; therefore, even if a patient had no pathological lesion, he/she was included in the primary analysis on the basis of the scoring of normal brain structures.
Image evaluation
All images were provided electronically by the centers and were reviewed for quality, clinical appropriateness, and protocol adherence by a central core laboratory. Images were evaluated by both the investigator and by three experienced (>10 years), independent neuroradiologists selected as fully blinded readers who also performed image quality assessment. Investigator and readers evaluated the following image sets separately: (i) combined unenhanced (T1w, T2w, FLAIR/STIR)/gadobutrol-enhanced T1w MR image sets, (ii) unenhanced MR image sets (not carried out by the investigator for degree of lesion contrast-enhancement), and (iii) combined unenhanced/gadoteridol-enhanced (T1w) MR image sets. The three image sets were randomized to ensure that only one of the three image sets for each patient was read in the same session. The primary efficacy analysis was evaluated using the average of three blinded reader assessments (average reader), and the sessions were separated by at least two weeks in order to minimize recall bias. The investigator and readers scored the lesion/normal structures using the image sequence that best depicted each efficacy variable in the particular image set. For each image set, the presence/absence of lesions and the total number of lesions, as well as the availability of images, were recorded. The degree of contrast-enhancement and border delineation were scored on a 4-point scale, where 1 = none and 4 = excellent. Internal morphology was scored on a 3-point scale, where 1 = poor (the structure and internal morphology of the lesion was poorly visible), 2 = moderate (the structure and internal morphology of the lesion was partially visible), and 3 = good (the structure and internal morphology of the lesion was sufficiently visible). Image quality was assessed by the direct paired comparison by the blinded readers of the T1w image sets for gadobutrol and gadoteridol, randomized on two display screens. Reader preference was rated on a 5-point scale (-2 to +2), where negative values indicated a worse image and positive values indicated a better image for gadobutrol vs gadoteridol, respectively. For determination of malignancy, diagnoses from the blinded readers and the truth committees were assessed as malignant, not malignant, or not assessable. For the malignant or non-malignant assessments, sensitivity, specificity, and accuracy were calculated.
Safety analysis
Vital signs and physical examinations were carried out at baseline. Laboratory parameters were monitored within one hour of contrast administration and up to the next contrast agent injection or >72 hours post-injection. Adverse events (AEs) were monitored >72 hours following the crossover MRI study with the second contrast agent (study Period 2) for all patients who received either gadobutrol or gadoteridol. As all subjects had normal renal function, >90% of gadobutrol or gadoteridol is excreted by the kidneys in 24 hours.
Statistical considerations
Sample size calculations were made based on non-inferiority of gadobutrol vs gadoteridol. A sample size of 231 patients was needed to provide 80% power to demonstrate non-inferiority. Additional patients were planned to be enrolled to account for patients having no lesions. Based on Phase II data in CNS imaging, the non-inferiority margin was set at -0.35, as this was the acceptable difference between means of the studied variable between the groups. The primary efficacy variables were analyzed using the arithmetic mean of the values for the four visualization parameters evaluated by the three blinded readers. For combined unenhanced/enhanced MR image sets, the three variables were analyzed separately for superiority using two-sided paired t-tests (P < 0.05 level of significance). Non-inferiority for the number of lesions was evaluated with one-sided t-tests (P < 0.025 level of significance). If the detected numbers of lesions were different, the denominator used to calculate the average of each modality of the other visualization parameters was determined by the modality with the greater number of lesions, which rewarded the detection of extra lesions. For image quality, frequency tables and descriptive statistics were generated on the scores given and the relative image qualities were tested for equality using a Wilcoxon signed-rank test. SAS version 9.1 was used for all statistical tests.
Results
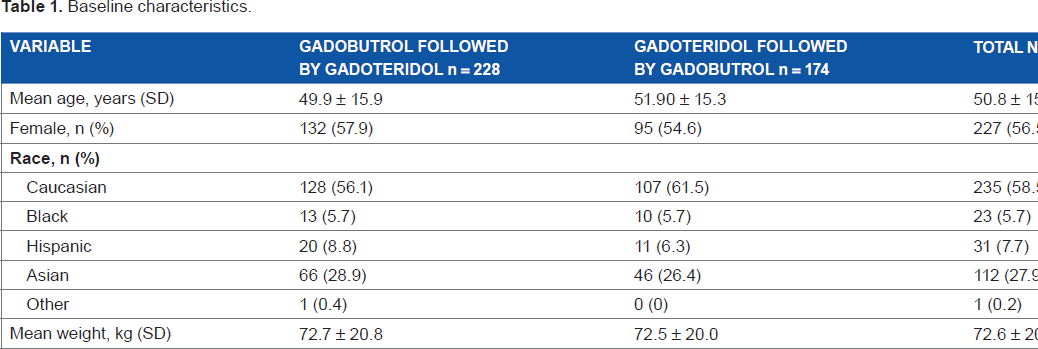
Patient disposition is shown in Figure 1. In all, 54 patients were not included in the primary efficacy analysis, with the majority of these cases being the initial training cases used for site validation and blinded reader training. Of the 402 treated patients, 390 patients received both gadobutrol and gadoteridol and 380 completed the study. The full analysis efficacy set included 336 patients. Patient baseline characteristics were similar between groups (Table 1). The most commonly reported lesion types were described as other (epilepsy/seizure/syncope, headache including migraines/pain/dizziness, transient ischemic attack/rule-out cerebral vascular accident/vascular malformations/subdural hematoma/trauma, depression/dementia and/or cognitive decline, infection/inflammation, and spinal pain including sciatica/extremity pain/radiculopathy; 36.3%), multiple sclerosis (15.9%), metastasis (14.9%), and meningioma (10.9%). Of the 60 patients considered to have metastasis, the primary tumor sites were lung (n = 35), breast (n = 11), other (n = 9), kidney (n = 2), stomach (n = 1), colon (n = 1), and unknown (n = 1).
Patient disposition. Baseline characteristics.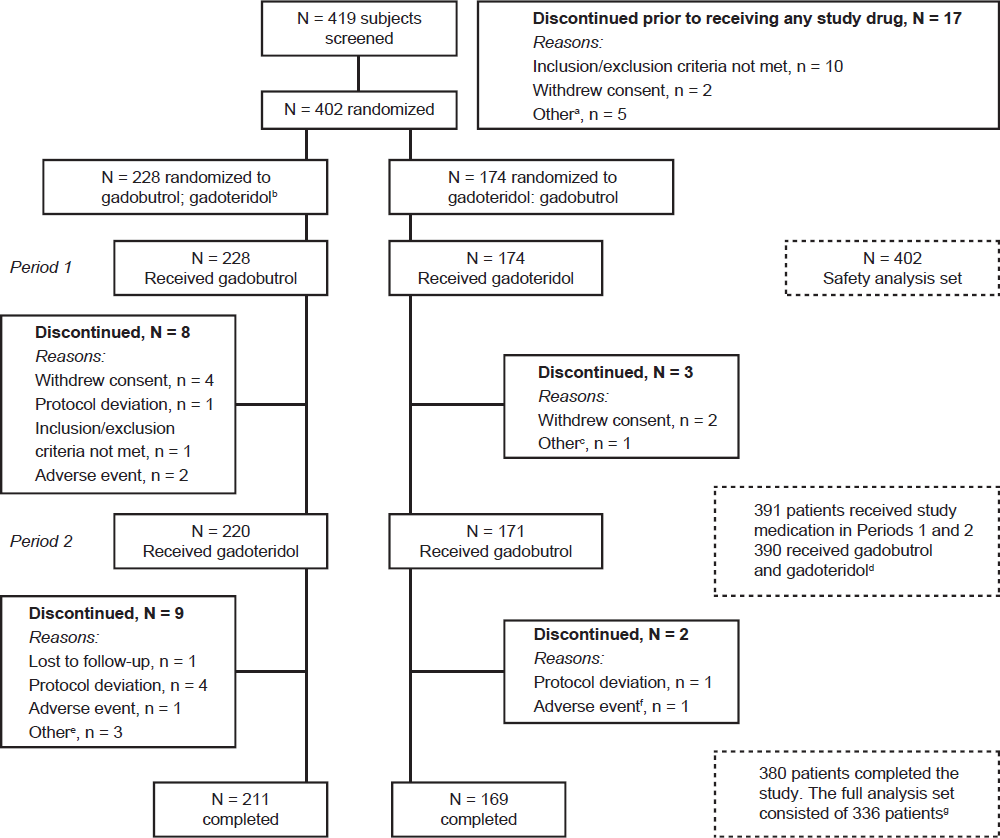
Visualization parameters
Test for superiority
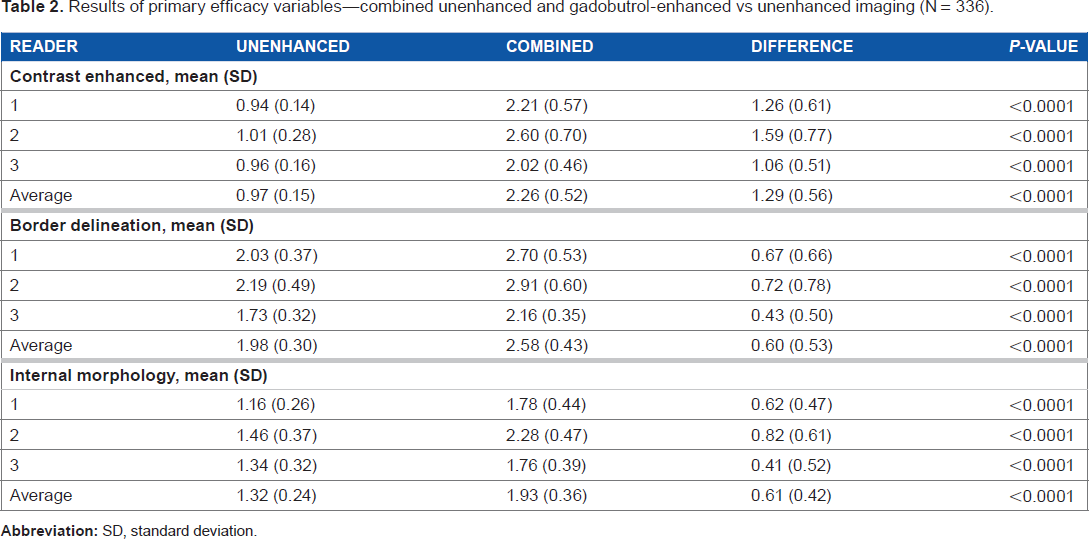
Results of primary efficacy variables—combined unenhanced and gadobutrol-enhanced vs unenhanced imaging (N = 336).
Test for non-inferiority
Combined gadobutrol vs unenhanced MRI did not achieve the pre-specified non-inferiority margin (the non-inferiority margin of 0.35 was met for only two of three blinded readers) for number of lesions. The mean number of lesions detected for the average reader was 8.08 for unenhanced MRI vs 8.25 for combined gadobutrol (difference = 0.17; 95% CI: -0.439, 0.780). As a supportive analysis, a non-parametric test was calculated using a pre-specified non-inferiority margin of -10% (which was considered clinically meaningful), for which non-inferiority was demonstrated for combined gadobutrol vs unenhanced images (difference for average reader = 8.9%; 95% CI: -0.5%, 18.4%). 15 Similarly, combined gadoteridol vs unenhanced MRI did not achieve the non-inferiority margin (the non-inferiority margin of 0.35 was met for only one of three blinded readers) for number of lesions. The mean number of lesions detected for the average reader was 8.08 for unenhanced MRI vs 8.24 for combined gadoteridol (difference = 0.16; 95% CI: -0.532, 0.851). Non-inferiority was demonstrated for combined gadoteridol vs unenhanced MRI for number of lesions for the non-parametric analysis at the margin of -10% (difference for average reader score = 3.6%; 95% CI: -5.9%, 13.1%).
For the average reader, combined gadobutrol was non-inferior (and actually demonstrated superiority) to combined gadoteridol for contrast-enhancement (average reader score: 2.28 vs 2.24, respectively; 95% CI: 0.004, 0.078). Non-inferiority was also demonstrated for border delineation (average reader score: 2.60 vs 2.56, respectively; 95% CI: -0.009, 0.082) and internal morphology (average reader score: 1.94 vs 1.91, respectively; 95% CI: -0.006, 0.059). The number of lesions detected was similar for combined gadobutrol- and combined gadoteridol-enhanced images (average reader score: 8.25 vs 8.24, respectively [difference = 0.01; 95% CI: -0.601,0.622]). As the lower limit of the 95% CI exceeded the pre-specified margin of -0.35, non-inferiority was not demonstrated.
Image quality
All three readers rated more positive scores for gadobutrol vs gadoteridol T1-enhanced images (indicating higher quality with gadobutrol) than negative scores (indicating higher quality with gadoteridol). The rates were 36.0%, 35.1%, and 62.2% in favor of gadobutrol vs 7.5%, 7.5%, and 24.4% in favor of gadoteridol. Mean scores ranged from 0.33 to 0.53 for the three readers (P < 0.0001 for each reader) (Fig. 2).
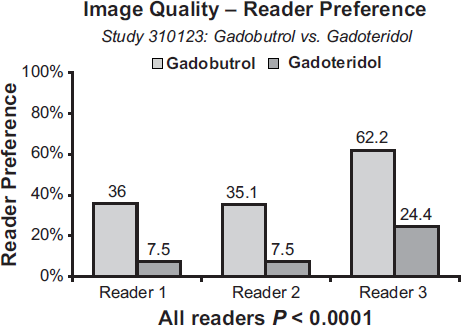
Preference rates for image quality for combined gadobutrol-enhanced vs combined gadoteridol-enhanced for the three blinded readers.
Detection of malignancy
For evaluation of sensitivity, specificity, and accuracy, 71 patients were excluded because the truth diagnoses were classified as not assessable. Based on the majority blinded reader, both the sensitivity and accuracy of combined gadobutrol were significantly greater than for combined gadoteridol (66.7% vs 60.2% [P = 0.014] and 87.7% vs 85.6% [P = 0.034], respectively). The improvement in sensitivity and accuracy for gadobutrol did not result in a corresponding decrease in specificity (specificity for both agents: 97.5%) (Fig. 3).
Sensitivity, specificity, and accuracy in determination of malignancy for combined gadobutrol-enhanced vs combined gadoteridol-enhanced imaging (majority reader diagnosis). Full analysis set (n = 336).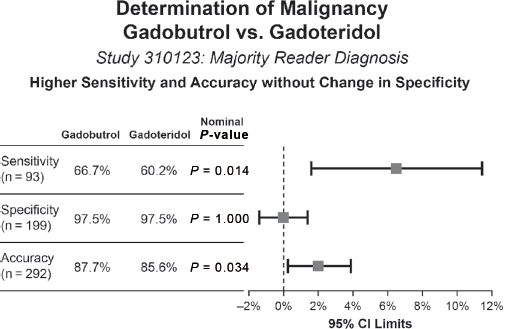
Adverse events
A total of 40 (10.0%) patients in the gadobutrol group and 38 (9.7%) patients in the gadoteridol group reported at least one treatment-related AE during the study (Table 3). One patient prematurely discontinued because of two serious AEs (worsening of general condition and somnolence) 26 hours after receiving gadobutrol and died after the follow-up period. This patient had high-grade glioma and died of his disease, and death was not considered to be related to the study drug or study conduct. Two patients experienced one serious AE during the gadobutrol period and one patient experienced two serious AEs during the gadoteridol period, none of which were considered to be related to the study drugs. Three patients in the gadobutrol period and one in the gadoteridol period discontinued because of AEs (reasons for discontinuation were allergic reaction with respiratory slowing, injection-site swelling, and blurred vision). There were no clinically relevant changes in laboratory evaluations, including serum creatinine levels in any patient.
Adverse events.
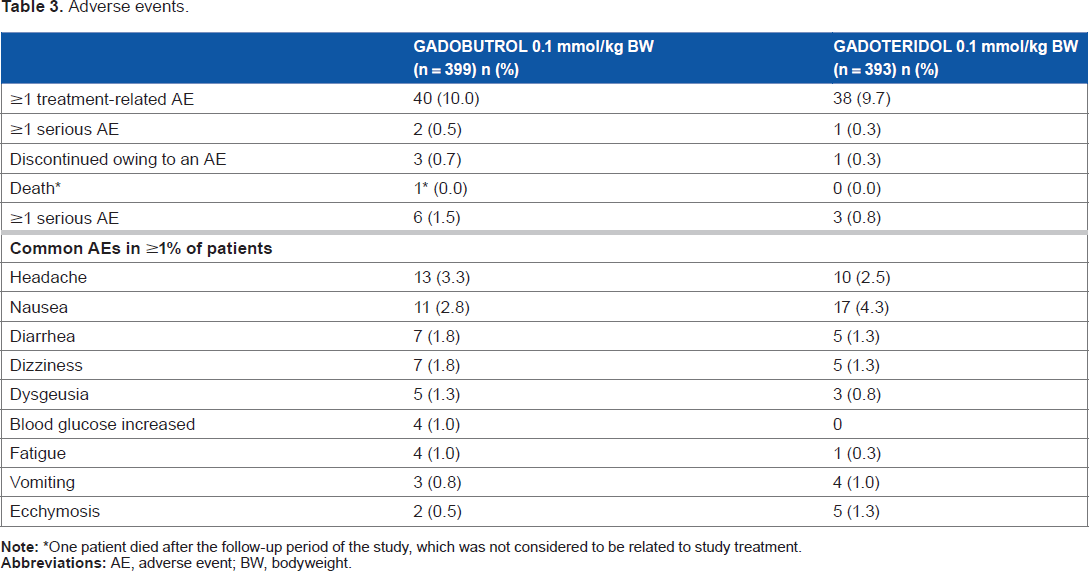
One patient died after the follow-up period of the study, which was not considered to be related to study treatment.
Case studies
Three patient case studies are presented that show a combination of gadobutrol-enhanced, gadoteridol-enhanced, or unenhanced images (Figs. 4–6). Figure 4 shows a follow-up evaluation after a glioma diagnosis, showing a small subdural hematoma with enhancement of the adjacent dura and a ring of parenchymal enhancement adjacent to the resection cavity. High relaxivity can give better lesion delineation; if the margins of the lesion are broader, they will be depicted more clearly by the high relaxivity agent. Figure 5 shows a patient with a recurrent glioma. The gadobutrol-enhanced T1w image showed increased intensity and fullness adjacent to the left temporal horn, which was interpreted as a glial tumor by the blinded readers (two of three readers) (Fig. 5A), whereas the gadoteridol-enhanced T1w image (b) had lower conspicuity as the blinded readers did not diagnose recurrent/ residual glial tumor (one of three readers) (Fig. 5B). Figure 6 shows a patient with a parietal-occipital metastasis. The gadobutrol-enhanced T1w image showed a ring-enhancing lesion in the right parietal-occipital region that extended to the dura but had no dural tail. The lesion involved both white and gray matter, had significant edema, and a central area of necrosis that was not enhanced, with a central dot probably representing a central feeding vessel (arrow) to the tumor. Two of the blinded readers interpreted this as a tumor but only one as metastatic disease and the other one as a glioma (Fig. 6A). The gadoteridol-enhanced T1w images showed an enhanced lesion in the parietal-occipital region; however, the internal morphology was poorly delineated. The area of necrosis was not as well defined, and the central vessel was not observed. Only one of the blinded readers interpreted this as a tumor (Fig. 6B). The FLAIR (non-contrast) images revealed the significant edema, but the lesion was hard to identify and the internal morphology was not depicted at all. A diagnosis was not possible from the non-contrast image alone (Fig. 6C).
Follow-up evaluation for a glioma diagnosis. (A) Gadobutrol-enhanced T1w image showed enhancement with sharp delineation of the anatomic involvement, which was diagnosed as residual/recurrent high-grade glial tumor by the blinded readers (two of three readers). (B) Gadoteridolenhanced T1w image shows less sharp rings of enhancement that were characterized by the blinded readers as infection rather than tumor (none of the three readers), which is in disagreement with the truth panel diagnosis. Patient referred for evaluation of brain metastasis. (A) Gadobutrol-enhanced T1w Spin Echo image through the left temporal lobe showing approximately a 1.5 mm metastatic foci. (B) Gadoteridol-enhanced T1w Spin Echo image at the same level demonstrates a vague intensity that was not identified as metastasis. More lesions were seen with Gadobutrol then with Gadoteridol. Parietal-occipital metastasis. (A) Gadobutrol-enhanced T1w image. (B) Gadoteridol-enhanced T1w image. (C) FLAIR (non-contrast) image.


Discussion
This Phase III trial supports previous findings that gadobutrol is efficacious at the dose tested (0.1 mmol/kg BW), with a safety profile consistent with previous studies and other approved extracellular MR contrast agents.3,8,16–19 The intra-individual crossover design of this study eliminated patient population variation between the treatment groups.
Gadoteridol was chosen as the comparator in this study as it is a macrocyclic agent approved for CNS imaging in the USA and was considered the best choice for patients receiving two gadolinium contrast agents within a short period of time. Both combined gadobutrol imaging and combined gadoteridol imaging were superior to unenhanced imaging for lesion contrast-enhancement, lesion border delineation, and lesion internal morphology and, based on non-parametric analyses, non-inferior for the number of lesions detected. The success of both contrast agents in comparison to unenhanced imaging was expected and strengthens the validity of the direct comparison of gadobutrol and gadoteridol. Non-inferiority of gadobutrol vs gadoteridol was demonstrated. For contrast-enhancement, the lower limit of the 95% CI was greater than zero, which demonstrates superiority of gadobutrol over gadoteridol for this parameter.
Image quality assessment for the paired T1w images from gadobutrol and gadoteridol was also overwhelmingly in favor of gadobutrol. As this was a prospective, intra-individual comparison study, most of the factors impacting the degree of contrast-enhancement, including subject/pathology variability, magnet field strength, contrast dose, post-dose image acquisition timing, and machine variability, were all controlled. The most likely reason for the enhancement differences is, therefore, likely to be based on the r1 relaxivity of the agents. All imaging was performed on 1.5 T systems, and the r1 relaxivity at this field strength is 5.2 L·mmol -1·second-1 in plasma at 37°C for gadobutrol and 4.1 L·mmol -1·second-1 for gadoteridol. 13 The type of coil used during imaging may also have some influence on image quality, although this was not investigated in this study. Another important aspect is the use of an acceleration factor that results in good image quality, and there is a balance between increasing imaging time and degree of acceleration. Each site tried to optimize image quality; however, it is not expected that this played a significant role in this study. The results here should, therefore, be representative of typical clinical CNS imaging.
Contrast-enhancement and image quality are both subjective assessments. The critical question therefore becomes: was there a difference in diagnostic outcome? An important diagnostic outcome is the ability to correctly detect or exclude malignancy. All CNS diagnoses were prospectively categorized as either malignant or non-malignant based on WHO criteria 2007. The majority blinded reader assessment of combined gadobutrol imaging had significantly higher sensitivity and accuracy for the detection of malignancy compared to combined gadoteridol imaging without a decrease in specificity. This diagnostic performance increase may be a result of improved enhancement in poorly enhancing malignant lesions. This is certainly a clinically relevant result as a missed malignancy could delay appropriate therapeutic intervention. It should be noted that, in this post-nephrogenic systemic fibrosis environment, gadobutrol has the highest T1-relaxivity among the three currently approved macrocyclic agents. Since gadoterate has a slightly lower relaxivity than gadoteridol, similar results in favor of gadobutrol would be expected in comparison with this agent. 20 In addition, the relaxivity of gadobutrol is only slightly decreased at a field strength of 3 T (5.0 L·mmol-1·second-1 at 3 T vs 5.2 L·mmol-1·second-1 at 1.5 T) compared with gadoteridol (3.7 L·mmol-1·second-1 at 3 T and 4.1 L·mmol-1·second-1 at 1.5 T). 13
Conclusions
The Phase III trial demonstrated that gadobutrol at a dose of 0.1 mmol/kg BW is an effective and well-tolerated contrast agent for MRI of the CNS. Gadobutrol-enhanced imaging significantly improved lesion contrast-enhancement, lesion internal morphology, and lesion border delineation vs unenhanced imaging. In comparison to gadoteridol, superior contrast-enhancement, good image quality, and improved differentiation of malignant vs benign lesions was demonstrated, which is attributed to the higher relaxivity of gadobutrol.
Australia
Lavier Gomes, Westmead Hospital, Westmead. Thanh Phan, Monash Medical Centre, Clayton.
Austria
Franz Ebner, Medizinische Universität Graz, Graz. Daniela Prayer, Allgemeines Krankenhaus der Stadt Wien Universitätskliniken, Wien.
Colombia
Jorge Andrés Delgado, Instituto de Alta Tecnología Médica de Antioquia, Medellín. Jaime Eduardo Ortiz, Centro de Diagnóstico Médico, Medellín. Fernando Gómez, DIME Diagnostico Medico, Cali.
Germany
Klaus Bohndorf, Zentralklinikum Augsburg, Augsburg. Eva Bültmann, Kliniken der Medizinischen Hochschule Hannover, Hannover. Arnd Dörfler, Friedrich-Alexander-Universität Erlangen-Nürnberg, Erlangen. Marco Essig, Deutsches Krebsforschungszentrum, Heidelberg. Christoph Groden, Klinikum Mannheim gGmbH, Mannheim. Martin Heller, Klinikum der Christian-Albrechts-Universität, Kiel. Johannes Hierholzer, Klinikum Ernst von Bergmann, Potsdam. Olav Jansen, Klinikum der Christian-Albrechts-Universität, Kiel. Randolf Klingebiel, Universitätsklinikum Charite zu Berlin, Berlin. Bodo Kress, Krankenhaus Nordwest, Frankfurt. Barbara Krug, Medizinische Einrichtungen der Universität zu Köln, Köln. Peter Reimer, Städtisches Klinikum Karlsruhe gGmbH, Karlsruhe. Wolfgang Reith, Universitätskliniken des Saarlandes, Homburg. D. Uhlenbrock, Medizinisches Versorgungszentrum, Dortmund. Rüdiger von Kummer, Medizinische Fakultät Carl Gustav Carus, Dresden.
Japan
Masaki Goto, Himeji Central Hospital, Himeji. Akira Ikeda, Social Insurance Chukyo Hospital, Nagoya. Seigo Ishii, Kishiwada Tokushukai Hospital, Kishiwada. Yasushi Ito, Osaka Medical Center for Cancer and Cardiovascular Diseases, Osaka. Nobuyuki Katakami, Institute of Biomedical Research and Innovation, Kobe. Seichi Kawamoto, Osaka General Medical Center, Osaka. Keiko Kuriyama, Osaka National Hospital, Osaka. Tsutomu Maruta, Himeji Medical Center, Himeji. Tatsuo Morimura, Utano National Hospital, Kyoto. Yoshimasa Mori, Nagoya Kyoritsu Clinic, Nagoya. Hidehiro Shima, Shimonoseki Kosei Hospital, Shimonoseki. Hisahiko Suzuki, Shin Suma Hospital, Kobe.
Switzerland
Karl Olof Lövblad, Hôpital Cantonal Universitaire de Genève, Genève. Christoph Ozdoba, Inselspital Bern, Bern. Thomas Treumann, Luzerner Kantonsspital, Luzern. Stephan Wetzel, Universitätsspital Basel, Basel.
USA
Robert Booth, University of Florida—Jacksonville, FL. Michael Brant-Zawadzki, Hoag Memorial Hospital Presbyterian, Newport Beach, CA. Fabio Danisi, Kingston Neurological Associates, PC, Kingston, NY. Colin P. Derdeyn, Washington University School of Medicine, St. Louis, MD. Kenneth R. Maravilla, University of Washington Medical Center, Seattle, WA. Elias R. Melhem, Hospital of the University of Pennsylvania, Philadelphia, PA. Joel R. Meyer, NorthShore University HealthSystem—Evanston Hospital, Evanston, IL. R. Michael Murray, West Alabama Research, Inc., Birmingham, AL. Jeffrey Rogg, Rhode Island Hospital, Providence, RI. Murray Solomon, Los Gatos MRI, Los Gatos, CA. Maria Spampinato, Medical University of South Carolina, Charleston, SC. Kipp VanCamp, Atchison Hospital, Atchison, KS. David L. Williams, Achieve Clinical Research, LLC, Tuscaloosa, AL.
The authors thank Sara Koenig, The University of Texas Health Science Center at San Antonio, Texas, for reviewing the manuscript and Discovery London, on behalf of Bayer HealthCare, for editorial support in preparing the manuscript.
Author Contributions
Conceived and designed the experiments: JEG, MR, JB, TB, JS. Analyzed the data: MR, JB, JA, TB, JS, DH, NA. Wrote the first draft of the manuscript: JEG, MR, JS. Contributed to the writing of the manuscript: JB, JA, TB, JS, DH. Agree with manuscript results and conclusions: JEG, MR, JB, JA, TB, JS, DH, NA. Jointly developed the structure and arguments for the paper: TB, JB, DH, MR, JS. Made critical revisions and approved final version: JEG, MR, JB, JS, TB, DH, NA. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgments
The authors would like to thank the following for their participation in this study: