
Abstract
Objective
To describe the spectrum of etiologic agents causing community associated UTI and their antimicrobial resistance trends in a large teaching hospital in Sharjah, United Arab Emirates.
Methods
A retrospective review of the microbiology laboratory records of four hundred ninety two cases of community associated UTI between April 2006 and March 2007 was carried out. Etiologic agents and their antimicrobial susceptibility pattern were analyzed.
Results
A wide spectrum of uropathogens was isolated of which the leading etiologic agents of community associated UTI were Escherichia coli (207 strains) and Klebsiella species (90 strains). Sixty-six per cent of Gram-negative bacilli were resistant to amoxicillin, 58.5% were resistant to trimethoprim-sulfamethoxazole and more than 50% were resistant to cephalexin. However, resistance rate to antimicrobials like ciprofloxacin and ceftriaxone remain relatively low 9.7% and 7.6% respectively.
Conclusions
Escherichia coli remains the leading cause of community associated UTI. In-vitro antimicrobial resistance pattern of the isolates revealed that trimethoprim-sulfamethoxazole, cephalexin and amoxycillin the commonly used first-line antimicrobials were becoming less and less effective in their treatment. This information can help in changing preferences of suitable antimicrobial agent in treatment of community associated UTI.
Introduction
Urinary tract infection (UTI) is one of the most common infections encountered and treated worldwide. The spectrum of etiologic agents causing urinary tract infections and their antimicrobial resistance pattern have been continuously changing over the years, both in community and in hospitals [1]. Trimethoprim-sulfamethoxazole (TMP-SMX) is the current treatment of choice in community associated UTI [2]. Many other antibiotics like amoxicillin, amoxicillin/clavulanic acid, cephalexin and ciprofloxacin are also often used in the empirical therapy for community associated UTI [3]. However, as with many community acquired infections, antimicrobial resistance among the uropathogens that cause community associated UTI is increasing [4]. For rational empirical therapy of community associated UTI, it is necessary to consider the spectrum of uropathogens and their antimicrobial susceptibility pattern time to time, as it may vary institutionally, temporally and geographically [5–8]. No data concerning the antimicrobial resistance of bacteria isolated from UTI in United Arab Emirates have been published to date. We obtained data on the uropathogens responsible for community associated UTI and their susceptibility patterns to the antimicrobial agents that are currently used for treatment in Sharjah, UAE. Such an evaluation may also be useful to detect emerging trends of antimicrobial resistance and serve as an indicator for change in antimicrobial prescriptions.
Methods
A retrospective review of the microbiology laboratory record of four hundred ninety two cases of community associated urinary tract infections attending to the Al Qassimi Hospital Sharjah between April 2006 and March 2007 was performed. Symptomatic UTI, was defined as a positive urine culture >/=10 5 CFU/mL of an uropathogen and the presence of >/=2 acute urinary symptoms. However, colony counts of 10 4 /mL and 10 3 /mL were also considered significant for non-enterobacteriaceae isolates, prior antimicrobial usages and yeast isolates respectively [9]. In cases where more than 1 pathogen was isolated, provided each reached the accepted threshold, they were both taken as uropathogen of significance. The urinary isolates were identified and antimicrobial susceptibility testing was carried out using the Vitek automated system (BioMerieux Vitek, Inc.,). Antimicrobial susceptibility test result of ten most commonly used antibiotics like amoxicillin (AMX) 25 μg, amoxicillin/clavulanic acid (AUG) 30 μg, trimethoprim-sulfamethoxazole (SXT) 25 μg, cephalexin (CPH) 30 μg, ceftriaxone (CFT) 30 μg, gentamicin (GEN) 120 μg, amikacin (AMK) 30 μg, norfloxacin (NFX) 10 μg, ciprofloxacin (CIP) 5 μg, and nitrofurantoin (NFT) 30 μg supplied by Oxoid, U.K. were analyzed only.
Results
During a period of one year, a total of four hundred ninety two bacterial isolates from community associated urinary tract infections were studied. The majority 406 (82.5%) of the isolates were from women while the remaining 86 (17.5%) were from men. Escherichia coli were the predominant pathogen (270 strains; 55%). The next four pathogens of importance were Klebsiella species including pneumoniae, oxytoca and ozanae (90 strains; 18%), and Citrobacter, Group B streptococci and Enterococcus species each (4%) (Fig. 1). Pathogens less frequently isolated (<4%) were not considered in this analysis. The antimicrobial resistance pattern for 10 commonly used antimicrobial agents of different classes against the six most frequent uropathogens of community associated UTI are summarized in (Table 1).
Causative agents of community associated urinary tract infections. Others* Includes Staphylococcus, Proteus, Pseudomonas and Enterobacter. Resistance pattern (%) of the most prevalent microorganisms isolated from community associated UTIs.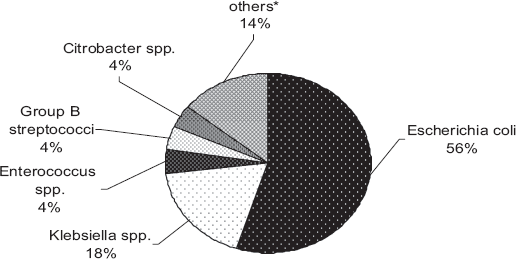
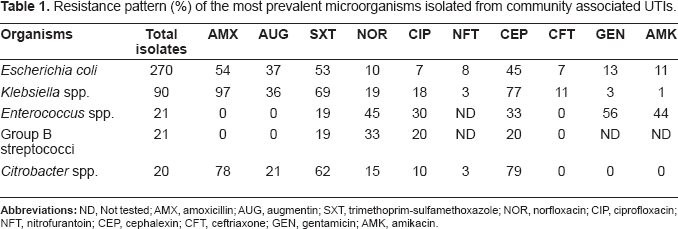
Escherichia coli showed high percentage of resistance to amoxicillin (54%), trimethoprim-sulfamethoxazole (53%), cephalexin (45%) and augmentin (37%). Aminoglycosides, third generation cephalosporins, and quinolones were better effective against E. coli isolates with susceptibility rate ranging between 87% to 92%. Klebseilla and Citrobacter spp. also had a similar spectrum displaying high percentage of resistance to trimethoprim-sulfamethoxazole, amoxycillin and cephalexin. Quinolones, amnoglycosides and third generation cephalosporins were found to be having better coverage with relatively low reported resistance.
Resistance rates of 20%–56% were observed against trimethoprim-sulfamethoxazole cephalexin, norfloxacin, gentamicin, and ciprofloxacin among the Gram-positive isolates like Enterococcus spp. and Group B streptococci. The same isolates were found to be better susceptible to amoxycillin, augmentin, and ceftriaxone with few reportable resistances.
Overall trimethoprim-sulfamethoxazole was the least effective against both gram-positive cocci and gram-negative bacilli. Amoxycillin, augmentin and cpehalexin were found to be less effective with significant resistance by the gram negative uropathogens. Qinolones, aminoglycosides and third generation cephalosporins provided the widest coverage.
Discussion
This study shows the distribution and antimicrobial resistance pattern of uropathogens isolated from community associated UTI in a hospital in Sharjah, United Arab Emirates. In our study, Escherichia coli remain the most important uropathogen causing community associated UTI and was isolated in 55% cases. Isolation of Escherichia coli as the predominant pathogen of community associated UTI has been extensively reported in many studies [10,11]. Although, the decline in E. coli isolation (55%) rate in our setting remains unclear. But, similar low rate isolation E. coli have also been reported by investigators from developed and developing countries [10,12]. K. pneumoniae was the second most common pathogen (18%). Increase isolation of gram-negative pathogens like Klebsiella and Citrobacter species, ahead of Proteus and Staphylococcus which are traditionally associated with community associated UTI clearly demonstrate a change in the spectrum which might have been affected by underlying host factors in general and development of antimicrobial resistance in particular [13,14].
Resistance rates among common uropathogens to many commonly used antimicrobial agents have increased over the years and theses resistance rates vary from country to country [15]. In our study, among the β-lactam antibiotics, amoxicillin had good activity against gram-positive cocci like enterococci and group B streptococci, intermediate activity against E. coli and very high resistance percentage (78%–97%) against pathogens like Klebsiella spp., Citrobacter spp. Similar to this observation various other studies have reported that the overall resistance rates to amoxicillin are between 45%–100% among the different urinary isolates [16,17]. This clearly states that using amoxicillin as a single agent for empirical treatment of a suspected UTI would not cover the majority of uropathogens especially the Enterobacteriacae family. Augmentin was found to be performing relatively better in the similar situation. Trimethoprim-sulfamethoxazole another commonly used 1st-line antimicrobial agent had very high resistance rates among the gram-negative isolates (53%–69%). This is in keeping with similar increase in resistance to trimethoprim-sulfamethoxazole reported in other countries [18,19], and indicates that the use of this antibiotic as a single agent for the treatment of UTI is not appropriate in our setting.
Alternative regimens such as fluoroquinolone are widely accepted as better empiric choice of UTI treatment in many countries [20]. We found that the fluoroquinolones provided good coverage against most gram-negative isolates with susceptibility rate ranging between 82% to 93% and a comparable rate among the gram-positives (susceptibility rates of 70%–80%). Similarly, low level resistance was reported to nitrofurantoin. This drug exhibited low resistance rate in the major part of the world (0%–5.4%), despite of it's being used for many years [21]. Our results shows fluoroquinolones are a better choice as reasonable empirical agents of community associated UTI.
Among the cephalosporins, first generation cephalosporin (cephalexin) was found to be least effective for all the uropathogens which showed significant degree of resistance. Whereas, third generation cephalosporin, ceftriaxone had a better spectrum of activity. However, these third generation cephalosporins should be recommended to patients with complicated pyelonephritis and patients who are unable to take oral antimicrobial therapy [15].
Aminoglycosides like gentamicin and amikacin which are known to have good coverage against Pseudomonas and other bacteria that are resistant to other antibiotics are usually reserved for serious UTI and used in combination with other antibiotics [22]. In our study, except Enterococci isolates which showed approximately 50% resistance to these aminoglycosides, others including E.coli were found to be better covered with susceptibility percentage ranging from 90%–100%.
This laboratory based in vitro study had several potential limitations like unavailability of information on age distribution of the patients and production of Extended-Spectrum beta-Lactamase (ESBL) by the isolates. We do appreciate the fact that multi-resistance is usually related to production of ESBL that lead to inappropriate use of antibiotics and treatment failure [23]. To solve this issue, our laboratory has recently (Jan 2008) incorporated ESBL testing as a routine procedure for the required isolates and we should be able to address the problem in near future.
In conclusion, this study provided the much needed information on the prevalence of common uropathogens of community associated UTI and their resistance trend to commonly used antimicrobials in Sharjah, United Arab Emirates. This study revealed that E. coli is the predominant bacterial pathogen of community associated UTI in Sharjah, UAE. It also demonstrated an increasing resistance to commonly used 1st- line antimicrobials like amoxicillin, trimethoprim-sulfamethoxazole and cephalexin by these isolates. We believe this information would provide a baseline for continuous surveillance of uropathogens spectrum and their resistance pattern to ensure appropriate treatment and prevent further development of drug resistance. Currently, the most appropriate agent for the empirical management of community associated UTI seems to be a fluoroquinolone like the ciprofloxacin.
Conflict of Interest Statement
Nothing to declare.
Footnotes
Acknowledgments
We are grateful to the staff members of the Laboratory Services, Al Qassimi Hospital, Sharjah, UAE who assisted in collection of study data.