Open accessResearch articleFirst published online 2010
Trend in Antibiotic Resistance of Streptococcus Pneumoniae and Haemophilus Influenzae Strains Isolated from Community Acquired Respiratory Tract Infections in Dakar,Senegal between 2005 and 2008
Development of antibiotic resistance among common respiratory pathogens is a major cause of concern worldwide. Streptococcus pneumoniae and Haemophilus influenzae are among the most common respiratory pathogens. In this study, representative samples obtained from 3 different medical centers in Dakar, Senegal were subjected to antibiotic susceptibility testing. The samples were collected from 2005 to 2008 and the data obtained was compared to establish resistance patterns between the two years (i.e. 2005–2006 to 2007–2008). S. pneumoniae exhibited a significant increase in the resistance to azithromycin and the intermediate susceptibility to penicillin G and cotrimoxazole. H. influenzae also exhibited a significant increase in resistance to azithromycin and intermediate susceptibility to chloramphenicol. None of H. influenzae samples were resistant to amoxicillin/clavulanic acid, cephalosporin and fluroquinolones and most of the S. pneumoniae isolates demonstrated high susceptibility to the antibiotics tested. Results from this study will provide greater insights to antibiotic therapy during respiratory tract infections in Dakar, Senegal. This study also establishes the importance of continuous monitoring of antibiotic susceptibility patterns that are often region-specific.
Respiratory tract infections (RTI) caused by Streptococcus pneumoniae along with Haemophilus influenzae are a leading cause of death despite antibiotic therapy. S. pneumoniae is a causative organism for severe RTIs including acute otitis media, acute bacterial exacerbations of chronic bronchitis and sinusitis, bacteremia, and community-acquired pneumonia.1–4 Including the above mentioned diseases, H. influenzae is also responsible for diseases such as childhood pneumonia and meningitis. There is increasing evidence of continuous evolution and geographical variation amongst these strains that is responsible for treatment complications.2,5–7 A major concern is the development of anti-bacterial resistance, as result it is imperative to choose a treatment regimen that is region-specific based on the local susceptibility patterns of the bacteria.
It has been previously established that the incidence of penicillin-resistant pneumococci has increased significantly, worldwide.8 The macrolide resistance in S. pneumoniae is mediated by two mechanisms; methylation of ribosomal macrolide target sites encoded by erm(B) gene and drug efflux encoded by the mef(A) gene.9 The development of resistance can often lead to complications in the otherwise empirical treatment of S. pneumoniae infections. On the other hand, H. influenzae strains exhibit disparate mechanisms of resistance. The most common mechanism of resistance to ampicillin and amoxicillin is β-lactamase production.10
The data obtained from different countries reveal significant geographical heterogeneity in the antibiotic resistance pattern.11–16 Hence, it is mandatory to determine resistance patterns that are region-specific rather than generalized. To date, none of the resistance studies focus on West Africa. In this retrospective study, we intend to report the antibacterial resistance pattern of S. pneumoniae, and H. influenzae, in Dakar, the capital city of Senegal. Clinical specimens were collected between 2005 and 2008. The changes in resistance pattern of these two organisms data obtained from 2005–2006 was compared to results obtained from 2007–2008. With this information, we aim to present valuable insights to the antibiotic treatment strategies that could aid in the physicians’ decision-making process.
Material and Methods
Sample collection
Clinical isolates of S. pneumoniae and H. influenzae were collected from patients with upper (acute otitis media and sinusitis) or lower RTI (community-acquired pneumonia, acute bronchitis). The clinical specimens included sputum, bronchoalveolar lavage, acute otitis medium effusions, blood, pus swab, sinus fluids, and throat swab. Patients were recruited at the Departments of Paediatrics and ORL, University Hospital of Aristide Le Dantec; Pneumology Department of University Hospital of Fann, and a private medical setting in Dakar, Senegal. The samples were analyzed at the Bacteriology and Virology Laboratory of the University Hospital Aristide Le Dantec. They were immediately cultured, and the strains isolated were identified according to the standard methods of microbiology. Antimicrobial susceptibility data from 2005–2006 were compared to data from 2007–2008.
Identification of bacterial isolates
S. pneumoniae was identified by presence of tiny, round, flat, and transparent colonies, with central depression (checker piece and nail head colonies), hemolysis of α-viridans, negative catalase and oxidase test, absence of bile-esculin hydrolysis, lysis by bile-salts, susceptibility to optochin and others biochemical characters (using API® Strep BioMérieux, La Balme-les-Grottes, France).
H. influenzae was identified by presence of tiny, moist, and smooth gray colonies, absence of hemolysis, positive catalase and oxidase test, presence of growth factors X and V, satellite growth around streaks of Staphylococcus aureus, and others biochemical characters (using API NH® galleria, BioMérieux, La Balme-les-Grottes, France).
Antibiotic susceptibility testing
Antibiotic susceptibility of all isolates of the test pathogens was analysed using the standard agar disk diffusion method and the E-test. The bacterial suspensions were suitably diluted to attain a final concentration of 105 CFU/ml (an optical density of 0.5 on the McFarland scale). H. influenzae suspension was inoculated on Haemophilus test medium, and S. pneumoniae was inoculated on Mueller-Hinton supplemented with 5% sheep blood. Disks (diffusion method) or strips (E-test) containing selected antibiotics were then placed on the inoculated plates. These plates were then incubated at 37 °C in a CO2 atmosphere for 18–24 hours. The test panel for S. pneumoniae includes penicillin G, amoxicillin-clavulanic acid, cefuroxime, ceftriaxone, azithromycin, levofloxacin, cotrimoxazole, chloramphenicol, clindamycin, erythromycin, and tetracycline. The test panel for H. influenzae included ampicillin, amoxicillin-clavulanic acid, ceftriaxone, ofloxaxin, azithromycin, chloramphenicol, and tetracycline. ATCC 49247 strain of H. influenzae and ATCC 49619 strains of S. pneumoniae were used as quality control strains. Minimal inhibitory concentrations (MICs) were calculated as MIC50 (MIC causing inhibition of 50% of isolates) and MIC90 (MIC causing inhibition of 90% of isolates). Percentage susceptibilities were calculated based on Clinical Laboratory Standards Institute (CLSI) break points.17
β-lactamase tests and typing of Hamophilus influenzae isolates
The H. influenzae isolates were examined for production of β-lactamase using a nitrocefin-based test (Cefinase, Becton Dickinson Microbiology Systems, Cockeysville, MD).
A latex particle agglutination test (Slidex, Biomerieux) was used to type all Haemophilus influenzae isolates.
Erythromycin and clindamycin double-disc diffusion test
The test was performed to identify the erythromycin resistant phenotype. On a blood agar plate, an erythromycin disk (15 μg) was placed 20 mm from the centre of a disc containing 10 μg of clindamycin. Blunting of the clindamycin inhibition zone proximal to the erythromycin disc indicated an inducible resistant phenotype, while susceptibility only to clindamycin with no blunting indicated the M-phenotype. Resistance to both erythromycin and clindamycin indicated constitutive resistance.
Statistical analysis
The WHONET software was used to analyze the antibacterial susceptibility test results.18 Comparisons of resistance development were made using the chi square test for frequencies (k proportions test). Significance was realised at P ≤ 0.05 (95% confidence interval).
Results
Patient demographics
For both microorganisms, the most frequent sources of bacterial isolates were bronchoalveolar lavage and sputum for both the time periods. Between November 2005 and August 2006, 100 isolates of S. pneumoniae and 71 of H. influenzae were collected, and 105 isolates of S. pneumoniae and 75 H. influenzae were collected between July 2007 and May 2008. For H. influenzae, 43 strains have been isolated in 2005–2006 and 39 in 2007–2008 from bronchoalveolar lavage. For S. pneumoniae, 36 strains have been isolated in 2005–2006 and 48 strains in 2007–2008 from bronchoalveolar lavage. Strains from sputum were obtained from 33 isolates in 2005–2006 and 30 in 2007–2008 (19 isolates for H. influenzae in 2005–2006 and 25 isolates for S. pneumoniae 2007–2008). Most of the isolates included in this study were obtained from patients >15 years of age.
Antibiotic susceptibility testing
All antibiotics demonstrated acceptable MICs values toward the controls strains.
S. pneumoniae
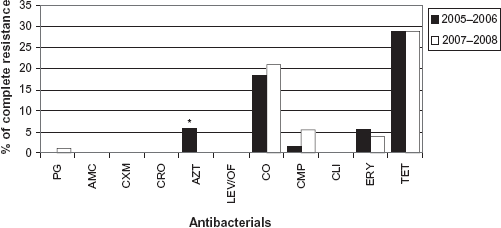
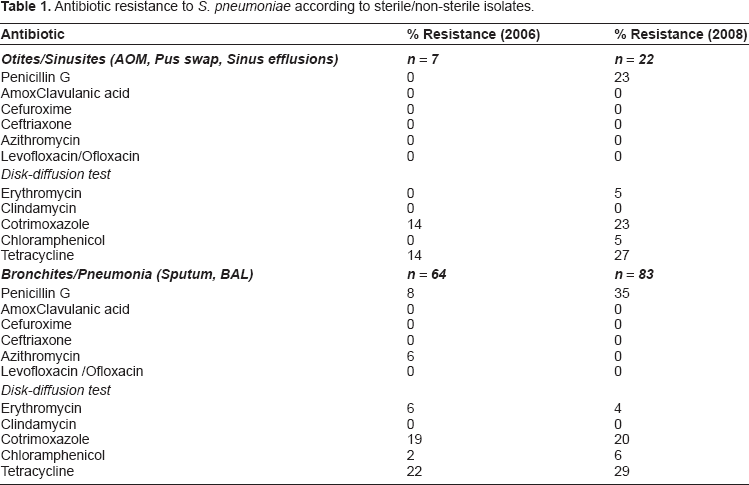
The resistance pattern of S. pneumoniae for each test antibacterial is given in Figure 1. For both the time periods, S. pneumoniae exhibited high susceptibility towards most of the antibacterials. The rate of resistance increased for penicillin G, cotrimoxazole, chloramphenicol, and tetracycline from 2005–2006 to 2007–2008. However, this increase was not statistically significant. The rate of resistance to azithromycin significantly decreased from 2005 to 2008. The intermediate susceptibility increased for all antibacterial except for amoxicillin/clavulanic acid, ceftriaxone and chloramphenicol. The rate of isolates that exhibited intermediate susceptibility to penicillin G increased significantly from 7.0% in 2005–2006 to 33.3% in 2007–2008. There was also a significant increase in the intermediate susceptibility to cotrimoxazole from 2005–2006 to 2007–2008. Few isolates (6%, 43 isolates in 2005–2006; 4%, 28 isolates in 2007–2008) were completely resistant to erythromycin and all were of the M phenotype (erythromycin-resistant, clindamycin susceptible). In order to further characterize the resistance pattern, data was individually analyzed according to isolates collected from sterile vs. non-sterile sites (Table 1). A difference was observed only in the resistance to penicillin G (8%, 5 isolates bronchitis/pneumonia samples; 0%, Otitis/Sinusitis samples in 2006).
Rate of complete resistance of S. Pneumoniae.
Antibiotic resistance to S. pneumoniae according to sterile/non-sterile isolates.
Antibiotic
% Resistance (2006)
% Resistance (2008)
Otites/Sinusites (AOM, Pus swap, Sinus efflusions)
n = 7
n = 22
Penicillin G
0
23
Amoxclavulanic acid
0
0
Cefuroxime
0
0
Ceftriaxone
0
0
Azithromycin
0
0
Levofloxacin/Ofloxacin
0
0
Disk-diffusion test
Erythromycin
0
5
Clindamycin
0
0
Cotrimoxazole
14
23
Chloramphenicol
0
5
Tetracycline
14
27
Bronchites/Pneumonia (Sputum, BAL)
n = 64
n = 83
Penicillin G
8
35
AmoxClavulanic acid
0
0
Cefuroxime
0
0
Ceftriaxone
0
0
Azithromycin
6
0
Levofloxacin /Ofloxacin
0
0
Disk-diffusion test
Erythromycin
6
4
Clindamycin
0
0
Cotrimoxazole
19
20
Chloramphenicol
2
6
Tetracycline
22
29
H. influenzae
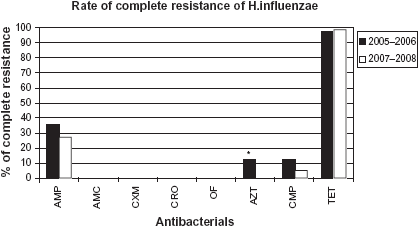
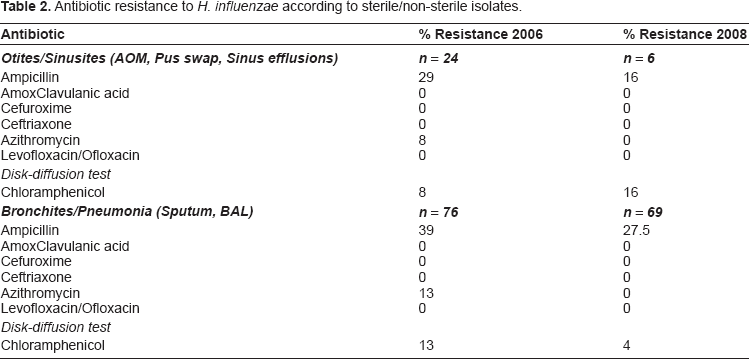
The resistance pattern of H. influenzae for each test antimicrobial is given in Figure 2. None of the isolates was resistant to amoxicillin/clavulanic acid, cephalosporin, and fluorquinolones For ampicillin, azithromycin, and chloramphenicol, the rate of resistance decreased from 2005–2006 to 2007–2008. However, this difference was significant only for azithromycin. Except for chloramphenicol and tetracycline, the rate of intermediate susceptibility remained fairly constant from 2005–2006 to 2007–2008. A significant increase in intermediate susceptibility was observed only for chloramphenicol. The rate of β-lactamase producing isolates decreased from 37% (37 isolates) in 2005–2006 to 27% (20 isolates) in 2007–2008 (P = 0.049). Subsequently, data was also analyzed according to the site of sample collection (Table 2). A difference was observed in the ampicillin resistance (29%, 7 isolates in otitis/sinusitis vs. 39%, 30 isolates in bronchitis/pneumonia sample in 2006). However, a decrease in resistance was observed in 2008 in otitis vs. bronchitis samples.
Rate at intermediate susceptibility of S. pneumoniae.
Antibiotic resistance to H. influenzae according to sterile/non-sterile isolates.
Antibiotic
% Resistance 2006
% Resistance 2008
Otites/Sinusites (AOM, Pus swap, Sinus efflusions)
n = 24
n = 6
Ampicillin
29
16
Amoxclavulanic acid
0
0
Cefuroxime
0
0
Ceftriaxone
0
0
Azithromycin
8
0
Levofloxacin/Ofloxacin
0
0
Disk-diffusion test
Chloramphenicol
8
16
Bronchites/Pneumonia (Sputum, BAL)
n = 76
n = 69
Ampicillin
39
27.5
Amoxclavulanic acid
0
0
Cefuroxime
0
0
Ceftriaxone
0
0
Azithromycin
13
0
Levofloxacin/Ofloxacin
0
0
Disk-diffusion test
Chloramphenicol
13
4
Discussion
The main aim of this study was to determine the trend of resistance of two common bacterial pathogens (S. pneumoniae and H. influenzae) responsible for development of RTIs in Dakar, Senegal from 2005 to 2008. Samples for this study were recovered from patients recruited at 3 different medical centres in Dakar. The majority of isolates were recovered from patients more than 15 years of age. Camara et al (Camara et al, 2003), have shown that 35% of bacteria isolated from meningitis were H. influenzae type-b. In this study, we have type the strains and found only 5 Hib among from children aged of 6–9 and one from children aged of 11 years. A total of 92% of isolated were non HIb. In Senegal Hib vaccine is included in the Expended Program for Immunization. This could explain the small number of Hib Isolates.
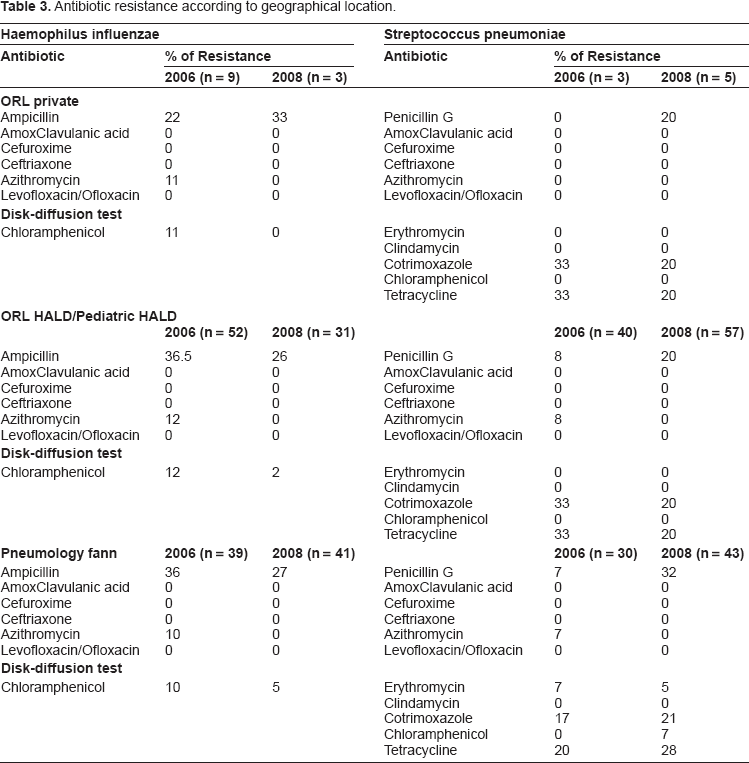
Individual data collected and analyzed for each of the three locations in presented in Table 3. Although information on previous antibiotic therapy could provide valuable information, since this is a retrospective study we were unable to obtain this information.
Antibiotic resistance according to geographical location.
Haemophilus influenzae
Streptococcus pneumoniae
Antibiotic
% of Resistance
Antibiotic
% of Resistance
2006 (n = 9)
2008 (n = 3)
2006 (n = 3)
2008 (n = 5)
ORL private
Ampicillin
22
33
Penicillin g
0
20
Amoxclavulanic acid
0
0
Amoxclavulanic acid
0
0
Cefuroxime
0
0
Cefuroxime
0
0
Ceftriaxone
0
0
Ceftriaxone
0
0
Azithromycin
11
0
Azithromycin
0
0
Levofloxacin/Ofloxacin
0
0
Levofloxacin/Ofloxacin
0
0
Disk-diffusion test
Chloramphenicol
11
0
Erythromycin
0
0
Clindamycin
0
0
Cotrimoxazole
33
20
Chloramphenicol
0
0
Tetracycline
33
20
ORL HALD/Pediatric HALD
2006 (n = 52)
2008 (n = 31)
2006 (n = 40)
2008 (n = 57)
Ampicillin
36.5
26
Penicillin g
8
20
Amoxclavulanic acid
0
0
Amoxclavulanic acid
0
0
Cefuroxime
0
0
Cefuroxime
0
0
Ceftriaxone
0
0
Ceftriaxone
0
0
Azithromycin
12
0
Azithromycin
8
0
Levofloxacin/Ofloxacin
0
0
Levofloxacin/Ofloxacin
0
0
Disk-diffusion test
Chloramphenicol
12
2
Erythromycin
0
0
Clindamycin
0
0
Cotrimoxazole
33
20
Chloramphenicol
0
0
Tetracycline
33
20
Pneumology fann
2006 (n = 39)
2008 (n = 41)
2006 (n = 30)
2008 (n = 43)
Ampicillin
36
27
Penicillin g
7
32
Amoxclavulanic acid
0
0
Amoxclavulanic acid
0
0
Cefuroxime
0
0
Cefuroxime
0
0
Ceftriaxone
0
0
Ceftriaxone
0
0
Azithromycin
10
0
Azithromycin
7
0
Levofloxacin/Ofloxacin
0
0
Levofloxacin/Ofloxacin
0
0
Disk-diffusion test
Chloramphenicol
10
5
Erythromycin
7
5
Clindamycin
0
0
Cotrimoxazole
17
21
Chloramphenicol
0
7
Tetracycline
20
28
The most significant changes were observed in the resistance of S. pneumoniae to penicillin G. Rates of intermediate susceptible isolates increased from 7% in 2005 to 33.3% in 2008. These rates were lower than those previously reported by Benbachir et al; 8.6% of pneumococcal isolates were fully resistant and 53.1% had intermediate susceptibility to penicillin G.19 The rate of complete resistance to penicillin G was 1% in 2007–2008 which is similar to a previous study reporting data from paediatric patients.20 Benbachir et al observed that resistance to other antibiotics (erythromycin, chloramphenicol and trimethoprim/sulfamethoxazole) is more frequent among pneumococcal isolates with reduced susceptibility to penicillin G as compared to the more susceptible isolates.19 In this study, although sharp differences were observed between penicillin G susceptible and non-susceptible isolates they were not statistically significant. In particular, the rates of resistance to trimethoprim/sulfamethoxazole and tetracycline were relatively high among penicillin G resistant isolates. On the other hand the rates of resistance to amoxicillin/clavulanic acid, cefuroxime, cefaclor, azithromycin, and ofloxacin were almost negligible.
Resistance of H. influenzae to ampicillin deceased from 35.4% in 2005–2006 to 26.7% in 2007–2008. These rates of resistance are in accordance with findings from a study conducted in the paediatric department of Fann hospital in Dakar on meningitis,20 as well as other studies conducted in other countries in Africa.21–27 In our study, we observed that β-lactamase production was the primary mechanism of ampicillin resistance for H. influenzae; all isolates that were resistant to ampicillin produced β-lactamase. The same results were observed in a previous study conducted in other parts of the world.10 Among other antibiotics tested the resistance to azithromycin decreased significantly between the two years whereas the decrease in resistance to chloramphenicol and tetracycline was insignificant.
In conclusion, the results from this study indicate that a significant increase of resistance of S. pneumoniae isolates to penicillin G. Resistance of H. influenzae remain relatively high; β-lactamase production was the primary reason for these high rates of resistance of H. influenzae associated with ampicillin. All bacteria remain susceptible to cephalosporins, fluoroquinolones, and macrolides. The results from this study re-emphasize the need for continuous epidemiological monitoring of antibiotic resistance.
Selecting an appropriate treatment regimen can often be a challenging task owing to rapid changes in resistance patterns. Thus the appropriate use of antibiotics should be guided by current trends in antibiotic resistance. The data reported thus far is intended to achieve this objective in Dakar. However, these trends should not be extrapolated to other regions of Senegal as it has been previously reported that resistance patterns exhibit significant geographic heterogeneity. Also, additional surveillance data is necessary from paediatric samples to report differences in the resistance pattern between adults and children, if any.
Publish with Libertas Academica and every scientist working in your field can read your article
“I would like to say that this is the most author-friendly editing process I have experienced in over 150 publications. Thank you most sincerely.”
“The communication between your staff and me has been terrific. Whenever progress is made with the manuscript, I receive notice. Quite honestly, I've never had such complete communication with a journal.”
“LA is different, and hopefully represents a kind of scientific publication machinery that removes the hurdles from free flow of scientific thought.”
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.
References
1.
HobermanA., MarchantC.D., KaplanS.L., FeldmanS.Treatment of acute otitis media consensus recommendations. Clin Pediatr (Phila).2002; 41(6): 373–90.
2.
BallP.Epidemiology and treatment of chronic bronchitis and its exacerbations. Chest.1995; 108(2 Suppl): 43S–52S.
3.
AnonJ.B., JacobsM.R., PooleM.D.Antimicrobial treatment guidelines for acute bacterial rhinosinusitis. Otolaryngol Head Neck Surg.2004; 130(1 Suppl): 1–45.
4.
NiedermanM.S., MandellL.A., AnzuetoA.Guidelines for the management of adults with community-acquired pneumonia. Diagnosis, assessment of severity, antimicrobial therapy, and prevention. Am J Respir Crit Care Med.2001; 163(7): 1730–54.
5.
MandellL.A.Community-acquired pneumonia: etiology, epidemiology and treatment. Chest.1995; 108: 35–42.
6.
GoldsteinF., BryskierA., AppelbaumP.C.The etiology of respiratory tract infections and the antibacterial activity of fluoro quinolones and other oral bacterial agents against respiratory pathogens. Clinical Microbiology and Infection.1998; 4(2): 8–18.
7.
JacobsM.R., FelminghamD., AppelbaumP.C., GrünebergR.N., the Alexander Project Group. The Alexander Project 1998–2000: susceptibility of pathogens isolated from community-acquired respiratory tract infection to commonly used antimicrobial agents. J Antimicrob Chemother.2003; 52: 229–46.
8.
FelminghamD., GrunebergR.N.The Alexander project 1996–1997: Latest susceptibility data from this international study of bacterial pathogens from community-acquired lower respiratory tract infections. J Antimicrob Chemother.2000; 45: 191–203.
ZhangR., EgglestonK., RotimiV., ZeckhauserR.J.Antibiotic resistance as a global threat: Evidence from China, Kuwait and the United States. Globalization and Health.2006; 2: 6.
12.
ChohanL., HollierL.M., BishopK., KilpatrickC.C.Patterns of Antibiotic Resistance Among Group B Streptococcus Isolates: 2001–2004. Infect Dis Obstet Gynecol.2006; 2006: 57492.
13.
MatsubaraK., NishiyamaY., KatayamaK.Change of antimicrobial susceptibility of group B streptococci over 15 years in Japan. J Antimicrob Chemother.2001; 48(4): 579–82.
14.
BaeS., LeeJ., LeeJ.Antimicrobial Resistance in Haemophilus influenzae Respiratory Tract Isolates in Korea: Results of a Nationwide Acute Respiratory Infections Surveillance. Antimicrob Agents Chemother.2010; 54(1): 65–71.
15.
SakataH.Changes over 10 years of ampicillin-resistant Haemophilus influenzae isolated from children. Jpn J Antibiot.2009; 62(4): 341–5.
16.
BorgmannS., JakobiakT., GruberH., SchröderH., SagelU.Prescriptions of broad-spectrum antibiotics to outpatients do not match increased prevalence and antibiotic resistance of respiratory pathogens in Bavaria. Pol J Microbiol.2009; 58(2): 105–10.
17.
Clinical, and Laboratory Standards Institute M2-A9.2006. Performance standards for antimicrobial disk susceptibility tests.Ninth edition. Approved Standard. Wayne. PA: CLSI.
BenbachirM., BenredjedS., BoyeC.S.Two-Year Surveillance of Antibiotic Resistance in Streptococcus pneumoniae in four African Cities. Antimicrob. Agents Chemother.2001; 45(2): 627–29.
20.
CamaraB, CisseM.F., FayePM BaPurulent meningitis in a paediatric hospital (Dakar, Senegal. Med Mal Infect.2003; 33(8): 422–26.
21.
Sife MefoH., SifeH., MbondaE.Les méningites purulentes de l'enfant au Nord Cameroun: Aspects cliniques, Bactériologiques et thérapeutiques. Med Afr Noire.1999; 46(1): 15–9.
22.
Akoua KoffiC., AnghuiH., Faye-KetteH.Aspects bactériologiques des méningites purulentes au CHU de Yopoughon, 1995–1998. Med Mal Infect.2000; 31: 475–81.
23.
DagnraA. Y., TigossouS., Prince-DavidM.Prévalence et sensibilité aux antibiotiques des bactéries isolées des méningites. Med Mal Infect.2000; 30(5): 291–94.
24.
BiendoM., YalaF., KounkouR.Les méningites bactériennes du nouveau-né et de l'enfant à Brazzaville: aspects bactériologiques et épidémiologiques (à propos de 348 cas). Afr Med.1990; 29(284): 201–04.
25.
EmeleF.E.Etiologic spectrum and pattern of antimicrobial drug susceptibility in bacterial meningitis in Sokoto, Nigeria. Acta Pediatr.2000; 89: 942–6.
26.
ThabetL., BoussetaK., KaabachiO.Bacteriological profile of bacterial meningitis in the Tunis childern hospital. Med Mal Infect.2002; 32(1): 1–7.
27.
CamaraB., FayeP.M., DioufS.Pediatric haemophilus influenzae b meningitis in Dakar. Med Mal Infect.2007; 37(11): 753–57.