
Abstract
Fish oil is rich in the omega-3 polyunsaturated fatty acids (PUFAs) eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). Numerous epidemiological studies and several large randomized clinical trials have shown that modest doses of omega-3 PUFAs significantly reduce the risk of unstable angina, myocardial infarction, and sudden cardiac death as well as death in coronary artery disease and heart failure patients. Based on the scientific evidence, the American Heart Association (AHA) has recommended all individuals eat fish at least twice a week to prevent cardiovascular disease. For individuals with coronary artery disease, the recommended dose of omega-3 PUFAs is 1 g of EPA and DHA daily. To lower triglyceride levels, much higher doses are needed. However, more recent randomized clinical trials have questioned the cardiovascular benefits of fish oil. These studies have contributed to the uncertainty health care providers face when recommending omega-3 PUFA supplementation according to clinical guidelines. The purpose of this review is to examine the randomized clinical trials and scientific evidence between omega-3 PUFAs and cardiovascular outcomes to better understand the current role of omega-3 PUFAs in improving cardiovascular health.
Introduction
Fish oil is rich in the omega-3 polyunsaturated fatty acids (PUFAs) eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). Treating individuals at risk for or with coronary heart disease (CHD) with these marine-derived omega-3 PUFAs, to improve cardiovascular outcomes, is supported by a number of epidemiological and randomized clinical trials (RCTs).1–6 The mechanism by which omega-3 PUFAs improve cardiovascular outcomes is thought to be due to their anti-inflammatory, anti-platelet, and anti-thrombotic effects as well as their favorable effects on arrhythmias, hypertriglyceridemia and other atherogenic lipoproteins, and endothelial function.7,8 Current guidelines from the American Heart Association (AHA) 9 recommend a dose of 1 g of EPA and DHA daily for patients after a myocardial infarction (MI). To lower triglyceride levels, much higher doses are needed and the AHA recommends a dose 2 g to 4 g of EPA and DHA daily. 10 To obtain the recommended dose of omega-3 PUFAs for individuals with coronary artery disease or to lower triglyceride levels, fish oil supplements are often needed.
In contrast to the early positive clinical trials of omega-3 PUFAs,3–6 other RCTs11–15 and a recent large meta-analysis 16 showed no protective effect on cardiovascular outcomes from omega-3 PUFA supplementation. These studies have cast into question the benefit of marine-derived omega-3 PUFAs and have contributed to the uncertainty health care providers face when recommending omega-3 PUFA supplementation according to clinical guidelines. The purpose of this review is to examine the RCTs and scientific evidence between omega-3 PUFAs and cardiovascular outcomes to better understand the current role for omega-3 PUFAs in improving cardiovascular health.
Clinical Evidence
Many prospective observational studies, large RCTs, and several meta-analyses have investigated the benefits of fish or omega-3 PUFA supplements on cardiovascular outcomes. Most have shown a significant reduction in CHD mortality and cardiovascular events in patients with and without cardiovascular disease. In contrast to these studies, other RCTs and a recent meta-analysis failed to demonstrate a reduction in CHD mortality or cardiovascular events with omega-3 PUFA supplementation (Table 1).
Overview of the randomized clinical studies evaluating omega-3 PUFAs.

Positive clinical trials
Four large RCTs have shown a benefit of omega-3 PUFAs in reducing mortality or cardiovascular events in patients with cardiovascular disease (Table 1). These include DART (Diet and Reinfarction Trial), 3 GISSI-Prevenzione (Gruppo Italinao per lo Studio della Sopravvivenza nell'Infarto miocardico-prevenzione), 4 JELIS (Japan EPA Lipid Intervention Study), 5 and GISSI-HF (Gruppo Italinao per lo Studio della Sopravvivenza nell'Infarto miocardico-heart failure). 6 DART randomized 2,033 men with a recent MI to receive or not receive a dietary intervention of eating at least two weekly portions of fatty fish. This corresponded to about 350 mg of EPA daily. The group that received advice to eat fatty fish demonstrated a 29% reduction in all-cause mortality. The reduction in all-cause mortality was driven primarily by a reduction in CHD deaths.
The GISSI-Prevenzione trial randomized 11,324 patients with a recent MI to receive either 850 mg of EPA and DHA daily, 300 mg of Vitamin E daily, supplementation of both, or no supplementation. Treatment with omega-3 PUFAs reduced the primary endpoint, a composite of death and cardiovascular events, by 15%. Among individual endpoints, omega-3 PUFA supplementation reduced all cause-mortality by 20%, cardiovascular death by 30%, and sudden cardiac death by 45%. There was no difference between the treatment groups for nonfatal cardiovascular events. The reduction in sudden cardiac death was particularly marked in the subgroup of patients with left ventricular systolic dysfunction, supporting an antiarrhythmic effect of omega-3 PUFAs. 17 Several other studies have also shown that omega-3 PUFAs can reduce the risk of ventricular arrhythmias and sudden cardiac death in patients with structural heart disease.18,19
The JELIS trial, examined omega-3 PUFA supplementation for primary as well as secondary prevention. In this study 18,645, mostly female patients with hypercholesterolemia were randomized to receive a statin with either 1,800 mg of EPA daily or placebo. Among individuals with CHD, the group receiving EPA had a significant 19% reduction in major coronary events, largely due to a reduction in unstable angina and nonfatal MI. In the primary prevention group EPA treatment showed a similar 18% reduction in major coronary events, though this did not reach statistical significance. However a subsequent analysis was able to show a significant 53% reduction in major coronary events in the subgroup of primary prevention patients with high triglyceride and low high-density lipoprotein (HDL) levels. 20 EPA supplementation did not reduce the risk of sudden or CHD death in either group.
The GISSI-HF trial randomized 6,975 patients with chronic heart failure to receive either 850 mg of EPA and DHA daily or placebo. Patients were also randomized to receive 10 mg of rosuvastatin daily or placebo. Omega-3 PUFA supplementation resulted in a small but significant 1.8% reduction in all-cause mortality and a 2.3% reduction in death or admission to the hospital for any cardiovascular reason. While the reduction in arrhythmic death was lower in the omega-3 PUFA group, the difference was not statistically significant. The rate of MI did not differ between the groups and in contrast to the benefit seen with omega-3 PUFAs, no benefit was seen in the group randomized to rosuvastatin.
Negative clinical trials
In contrast to these positive RCTs, five other large RCTs failed to show any benefit of omega-3 PUFAs in reducing cardiovascular mortality or events (Table 1). Similar in design to the DART trial, the DART 2 trial 11 performed in men with angina failed to reproduce the findings of the DART 1 trial. The Alpha Omega 12 and Omega 13 trials randomized patients after an MI to omega-3 PUFA supplements or placebo. However, unlike GISSI-Prevenzione and the GISSI-HF trials, no reduction in CHD mortality, sudden death, or cardiovascular events were seen. A post hoc analysis of the Alpha Omega trial showed, however, that in patients with MI and diabetes, a combination of EPA and DHA reduced both fatal CHD and ventricular arrhythmia related events by 40%. 21 The reduction in these endpoints was similar to the reductions seen in the GISSI-Prevenzione trial.
The SU.FOL.OM3 trial studied 2,501 patients with a history of cardiovascular disease and randomized them to a daily supplement of vitamins or placebo or to a daily combination 400 mg of EPA and 200 mg of DHA or placebo. 14 Supplementation with omega-3 PUFAs did not confer any significant benefit with regards to reducing major cardiovascular events, non-fatal MI, or total mortality.
Most recently, the ORIGIN trial studied 12,536 high-risk patients with or at risk for diabetes and randomized them to receive 840 mg of EPA and DHA daily or olive oil placebo capsules. 15 Just over one-half of patients had a history of cardiovascular disease. Treatment with omega-3 PUFAs did not result in a reduction in total mortality, cardiovascular mortality, or any cardiovascular event compared to placebo.
A recent meta-analysis by Rizos and colleagues 16 included 20 RCTs evaluating the effect of omega-3 PUFAs on cardiovascular outcomes and failed to show any statistically significant association with omega-3 PUFAs and major cardiovascular outcomes, including cardiac and sudden cardiac death, MI and stroke. The study has been criticized as it included clinical trials that used different doses and sources of omega-3 PUFAs and used an unusually strict standard for statistical significance. Using the typical standard, the analysis would have concluded that omega-3 PUFA supplements are associated with a 9% reduction in cardiac deaths. 22
Explaining the differences between studies
There are several possible explanations for the different outcomes seen between the RCTs of omega-3 PUFAs. These include differences in trial design, omega-3 PUFA dose, patient characteristics, duration of follow-up, and better compliance with evidence-based guidelines for the treatment of coronary artery in patients randomized to omega-3 PUFAs (Table 2).
Details of the randomized clinical studies.
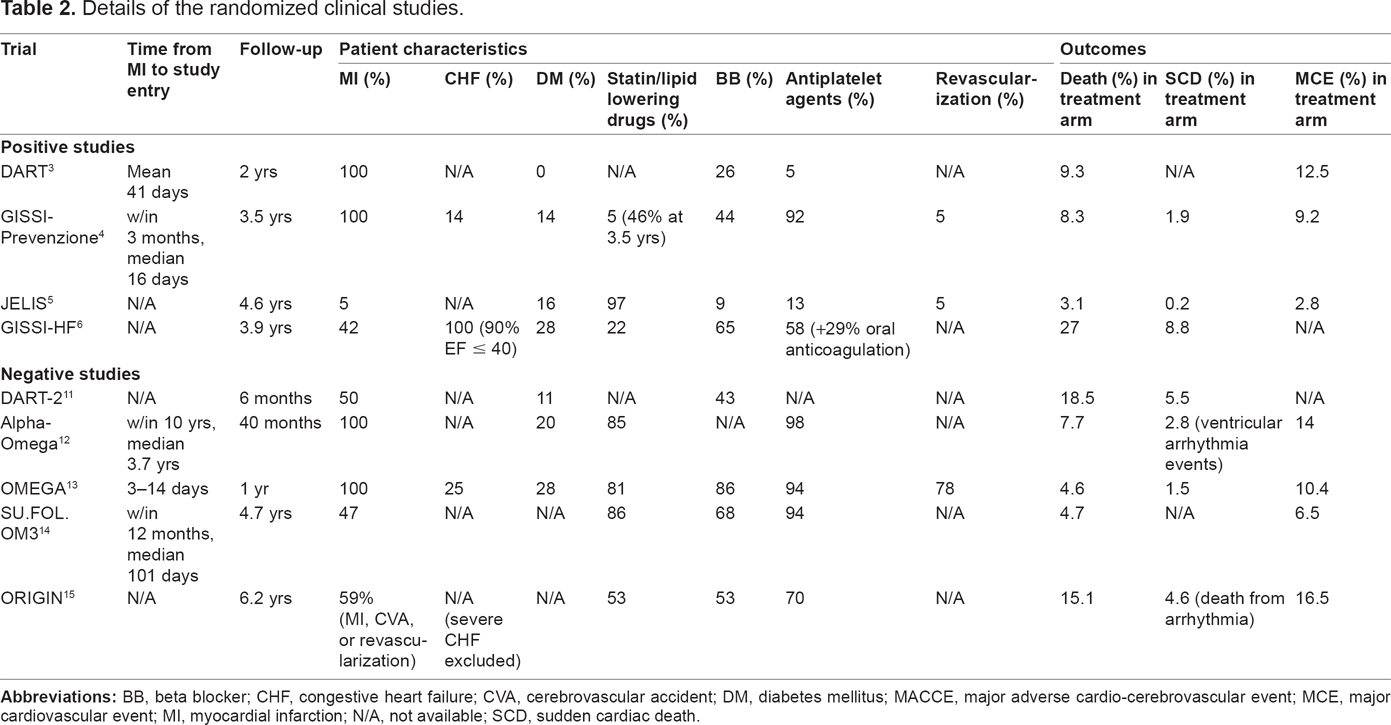
The Alpha Omega 12 and OMEGA 13 trials enrolled patients following MI and both failed to show any benefit of omega-3 PUFA supplementation in reducing cardiovascular events. Among patients randomized to omega-3 PUFAs in the Alpha Omega trial, the use of lipid-lowering drugs was high at 85%, as was the use of antithrombotic agents at 98%, and blood pressure-lowering drugs at 91%. In the OMEGA trial, 81% in the treated group were on statins, 86% on a beta-blocker, 94% on aspirin, and 88% on clopidogrel. In the GISSI-Prevenzione trial, 4 which enrolled patients following a recent MI and did show a benefit of omega-3 PUFAs in reducing total mortality and sudden death, the use of cholesterol-lowering drugs at baseline and beta-blockers was low at 5% and 44%, respectively. In addition, in GISSI-Prevenzione coronary revascularization was low at 5%, while in the OMEGA trial, 94% of patients underwent acute coronary angiography and 78% underwent coronary intervention. It may be difficult to detect a benefit in reducing CHD events for any intervention in a patient who has been treated aggressively with medical and interventional therapy in short-term follow-up. The duration of the Alpha-Omega study was just over 3 years and OMEGA followed patients for only one year.
The differences in omega-3 PUFA dose in treated patients may also explain the different outcomes among the RCTs. The JELIS trial 5 randomized patients to 1800 mg of EPA a day and showed a reduction in CHD events. This dose of omega-3 PUFA was much higher than in other RCTs and a high dose may be needed to reduce CHD events, while the benefit of reducing mortality and sudden death with omega-3 PUFAs may occur at lower doses. In GISSI-Prevenzione 4 and GISSI-HF 6 a dose of 1 g of prescription formulation omega-3 PUFAs was used and both studies showed a significant reduction in total and cardiac death. In addition to dose, the time period between randomization to active treatment following MI may also have influenced outcomes. Re-analysis of the GISSI-Prevenzione data show that the reduction in sudden cardiac death, which was the major component of total mortality reduction, occurred very early in the course of treatment, with the reduction in sudden death being statistically significant by 4 months. 19 A recent study using data from the General Practice Research Database from over 700 general practices in the United Kingdom identified 2446 patients who had a first MI and had received 1 g of prescription formulation omega-3 PUFA within 90 days of their event. 23 In a matched-cohort analysis, despite most patients being treated with lipid-lowering, antihypertensive and antiplatelet drugs, the authors found a 22% lower death rate for those patients prescribed omega-3 PUFAs within 90 days of their MI when compared to the control group. The death rate was 32% lower if the omega-3 PUFA supplements were started within 14 days of their MI. The findings from this study confirm the findings in GISSI-Prevenzione and may explain why some of the RCTs did not show a reduction in sudden death with omega-3 PUFAs following MI.
Few of the RCTs enrolled patients with heart failure. Patients with heart failure are at the highest risk of sudden cardiac death and, in addition to their anti-arrhythmic effects, omega-3 PUFAs have favorable effects on cardiac function and on the progression of heart failure.24,25 In a post-hoc analysis of the GISSI-Prevenzione trial the reduction in sudden cardiac death was isolated to those patients with systolic dysfunction. 17 The smaller number of patients with heart failure in some of the RCTs may also explain their negative results.
Unresolved issues
Omega-3 PUFAs lower triglycerides and have many favorable cardiovascular effects. Despite the conflicting results among the RCTs, the evidence remains strong for benefits of omega-3 PUFAs in reducing mortality and CHD events, especially in those individuals with congestive heart failure, MI, and diabetes, as well as in those patients not optimally treated for their CHD. However, several unresolved issues remain and ongoing study is needed. Some areas to be considered include whether higher doses of omega-3 PUFAs prove more effective, if EPA alone is better than EPA in combination with DHA, whether lowering triglycerides with omega-3 PUFAs will improve CHD outcomes, and if omega-3 PUFA supplementation in patients whose CHD is not well treated or in those patients with a poor intake of dietary omega-3 PUFAs show benefit. Before physicians stop recommending that their patients increase their intake of oily fish, or stop prescribing omega-3 PUFA supplements, they should await the results of several ongoing large RCTs (Table 3).
Ongoing randomized clinical trials.

Conclusions
Current guidelines recommend at least 2 to 3 helpings of oily fish a week to maintain good health and reduce cardiovascular risk. This is especially important given the low consumption of fish in most Western diets. Although the guidelines also recommend 1 g of combined EPA and DHA for individuals with CHD, this recommendation has now been challenged by recent large RCTs that have shown no benefit of low dose omega-3 PUFA supplementation in patients with a history of MI. However, the evidence is strongest for a protective effect of lower doses of omega-3 PUFA supplements in those patients with CHD who have heart failure or a low ejection fraction, diabetes, are not receiving optimal treatment for their CHD, or have elevated levels of triglycerides. Physicians should consider using omega-3 PUFA supplements in these patients. When omega-3 PUFAs are used they should be started as soon as possible after the patient's MI. Higher doses of omega-3 PUFA of approximately 4 g of EPA and DHA daily can lead to significant reductions in triglyceride levels and should be a central therapeutic option for patients with high and very high levels of triglycerides.
We need to inform our patients of the benefits of omega-3 PUFAs and recommend that they increase their dietary intake of oily fish. For those patients where higher doses of omega-3 PUFAs are needed, supplements should be used. More research is required in this area and as we await the results of ongoing clinical studies we recommend that physicians continue to recognize the benefits of omega-3 PUFAs to reduce cardiovascular risk in their high risk patients.
Footnotes
Author Contributions
Conceived and designed the experiments: LMK, DGK. Analyzed the data: LMK, DGK. Wrote the first draft of the manuscript: LMK, DGK. Contributed to the writing of the manuscript: LMK, DGK. Agree with manuscript results and conclusions: LMK, DGK. Jointly developed the structure and arguments for the paper: LMK, DGK. Made critical revisions and approved final version: LMK, DGK. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests. Provenance: the authors were invited to submit this paper.