
Abstract
Background
Training future healthcare profession students using interprofessional education (IPE) is critical to improve quality of health care and patient safety.
Objective
The objective of this study was to implement an IPE program and determine student satisfaction with each session, including a clinical case requiring teams with members from each profession addressing clinical scenarios.
Subjects
The subjects of this study were students from Athletic Training, Medicine, Nursing, Pharmacy, Physical Therapy, Physician Assistant, Social Work, and Speech-Language Pathology.
Methods
Evaluations, administered to all participating students, consisted of Likert-style responses, rating agreement with a series of questions, and space for descriptive comments. Score differences for each question were compared using independent group t-tests with a P-value of 0.05 to determine statistical significance.
Results
There were statistically higher satisfaction ratings for the problem-based learning case when compared to less interactive sessions (P < 0.0001).
Conclusion
Students perceived benefits of the IPE program. Perceptions improved when various students had the opportunity to work together on clinically relevant problems.
Keywords
Introduction
Interprofessional education
Interprofessional education (IPE) has been heralded as a critical foundational concept toward improving the quality, effectiveness, and efficiency of patient safety in the healthcare system by improving interprofessional attitudes, respect, and collaboration.1–3 As defined by the National Center for Interprofessional Practice and Education, adapted from the Centre for the Advancement of Interprofessional Education in the United Kingdom and the World Health Organization, IPE “occurs when two or more professions (students, residents, and health workers) learn about, from, and with each other to enable effective collaboration and improve health outcomes”.2,4 This collaboration affords future healthcare workers with experience engaging individuals from other backgrounds who possess the pertinent skills to produce a more comprehensive health service to individuals and the community. This type of collaboration also recognizes the concept of situational leadership. Based on the leadership theory of Hersey and Blanchard, situational leadership is a task-based approach where successful leaders adapt their leadership styles to suit the task at hand, the constitution of the team and, in the case of clinical encounters, the welfare of the patient. 5
Because of the responsibility of all health professions for the provision of high-quality health care to patients and communities, the quality and sustainability of health professions programs are monitored through a process referred to as accreditation. For all national undergraduate medical education programs, the accrediting body is the Liaison Committee on Medical Education (LCME). The LCME has identified the importance of IPE and has asked medical schools to supply evidence of compliance to the following accreditation standard:
The faculty of a medical school ensure that the core curriculum of a medical education program prepares medical students to function collaboratively on healthcare teams that include other health professionals from other disciplines as they provide coordinated services to patients. These curricular experiences include practitioners and/or students from the other health professions (LCME Standard 7.9). 6
Even with the documented and perceived benefits of IPE, not all health profession disciplines have integrated IPE into their curricula. Of those who have, there is great variety in the approaches to IPE. There is also a general lack of established, comprehensive metrics and evaluation tools to study the effectiveness of IPE.7–10 Health professions programs looking to initiate an IPE program in their curriculum are met with literature describing various IPE programs and activities, but very limited information on the achievement of student learning outcomes developed for these programs.
IPE at Central Michigan University College of Medicine
In 2013, the Central Michigan University College of Medicine opened its doors to the inaugural class of 64 students, with a subsequent recurring class size of 104 students. The College's mission is to prepare
diverse, culturally competent physicians focused on improving access to high quality health care in Central and Northern Michigan with an emphasis on rural and medically underserved regions. Our graduates will aspire to excellence in providing patient-centered and evidenced-based care to their patients and their communities. We will engage physicians in leading healthcare transformation, lifelong learning and team-based education.
11
In order to accomplish the mission of the College of Medicine, program faculty, administration, and community partners made the decision to design and deliver the medical education program in a manner that differed in important ways from traditional medical education programs. The traditional approach to medical education involves the teaching and learning of the foundational sciences and the clinical sciences as distinct entities. The foundational sciences are typically relegated to the first two years of the four-year program, followed by two years of hospital-based clinical education and training. The College of Medicine designed and implemented an integrated, team-based approach to teaching and learning of the foundational medical sciences and the clinical content throughout the four-year program, through the use of integrated curricular approaches such as problem-based and case-based small-group learning sessions. The College of Medicine faculty and community partners developed a framework of seven competencies that are used for all aspects of program development. The competencies, integrated throughout each teaching and learning activity, are Patient Care, Medical Knowledge, Systems-Based Practice, Population and Community Health, Professionalism, Practice-Based Learning and Improvement, and Interpersonal and Communication Skills. 12
The inclusion of a team-based approach to educational learning sessions was core to the creation of the medical education program and has served to promote the integration of the foundational medical sciences and clinical curricular content into each learning session, where appropriate. This approach, which has fostered the creation of a learning environment that values diversity and is supportive of lifelong learning for our graduates, faculty, staff, and community partners, was a core consideration in the creation of the medical education program. Also, aligning with our seven competencies, it was essential that the program find ways to promote interprofessionalism and team-based approaches in health care, inside and outside of the traditional classroom setting. Opportunities to support and serve community educational needs across the continuum of medical education was an important tenet of the development of the curriculum for all years of the program. With the seven competencies serving as a guiding framework, the school developed an IPE program that is innovative, student-focused, and engaged with community education partners. It is also one that utilizes highly interactive pedagogy including problem-based learning (PBL), case-based learning (CBL), and team-based learning (TBL). The result of this curricular planning is the Integrated Community Experience (ICE).
IPE within an ICE
The ICE is designed as a component of the longitudinal Essentials of Clinical Skills course delivered immediately in the first week of medical school curriculum and presented over the first two academic years. ICE helps prepare medical students to function collaboratively in healthcare teams and provides them with opportunities to develop an understanding of three key concepts that the school believes are fundamental to the current and future practice of medicine.
These concepts include:
understanding how medicine is practiced in a new era of medical education, medical research, and community engagement;
understanding a new model for patient-centered practice of medicine; and
understanding the services available to assist in patient care and the responsibility of physicians in training to engage these community services.
The ICE program is designed to provide students with opportunities to practice their clinical skills and apply medical knowledge in a primary care setting. Students are assigned in pairs to conduct visits to local physicians’ offices, where they learn about the functioning of the practice, and the role of various healthcare professionals in the office as part of the team providing patient care.
In both years of the ICE program, there is a focus on IPE, community engagement, and clinical practice. In Year 1, students are tasked with learning about the healthcare professionals in each of the physician practices by seeing firsthand how they function as members of the healthcare team. Students are required to examine and reflect on the ways in which the physician practices are organized and how they function through the eyes of the office staff, the physicians, and most importantly through the experiences of the patients in these practices. To accomplish this, students spend time with the patients hearing about how they became patients and why they stay with these practices.
In Year 1 of the ICE program, College of Medicine faculty and staff, in collaboration with the faculty of other medical professional programs, present a series of IPE sessions with students from allied health professions training programs including Athletic Training, Medicine, Physical Therapy, Physician Assistant, Social Work, and Speech-Language Pathology from programs at CMU, Nursing from Mid-Michigan Community College, and Pharmacy from Ferris State University.
In Year 2 of ICE, students are tasked with designing, developing, and implementing a service learning project so that students can build relationships with, and improve the wellbeing of, community members.
Introduction of PBL into IPE
The first iteration of the IPE component (2013/2014) included students from seven different health professions relying heavily on interactive large-group didactic-style sessions to increase their IPE knowledge and skill base. Student feedback on the initial IPE experience, coupled with our successes in integrating interactive small-group learning in other areas of our curriculum, led us to alter how we implement IPE during the second iteration. Student evaluations from our first two IPE events in 2014 indicated that students desired to work and problem solve with students from other professions, while getting to know each other. Because the College of Medicine successfully implemented a medical education curriculum rooted in PBL and CBL, and the College of Medicine faculty had experience writing and facilitating these educational sessions, the decision was made by the IPE leadership to create a case-based PBL session for the IPE experience that would foster feedback and collaboration from various health professions.
Literature, while limited, supports the effectiveness of PBL in IPE. As best summarized by Thompson, 13 a PBL IPE design fulfills an aim of IPE, which is to improve attitudes toward other professional groups. Our IPE clinical case incorporates all eight disciplines that are currently represented in the IPE program, and PBL teams are designed to distribute students into small interprofessional teams to better engage in the exercise.
Methods
Population and study samples
Participants in IPE sessions included students from eight health professions disciplines (seven in the first iteration) that spanned three Michigan postsecondary institutions. Programs included were as follows: Athletic Training, Medicine, Nursing, Pharmacy, Physical Therapy, Physician Assistant, Social Work, and Speech-Language Pathology (Table 1). Program participation in each session was informed by program schedules, transportation, weather, budget, and capacity of space. The number of participants ranged from 178 to 479 per IPE session with evaluation response rates ranging from 87% to 96%.
Session participation by program.

Total number of session participants (number who completed evaluations).
IPE session design
IPE iteration 1 (2013–2014 academic year)
Formal IPE instruction consisted of two sessions that took place in the first year of the College of Medicine's curriculum. Both sessions involved two interactive large-group IPE sessions. This first iteration included students and instructors from the following seven programs: Medicine, Nursing, Pharmacy, Physical Therapy, Physician Assistant, Social Work, and Speech-Language Pathology. Session 1 in January 2014 included students and instructors from the following six programs: Medicine, Nursing, Physical Therapy, Physician Assistant, Social Work, and Speech-Language Pathology, whereas Session 2 in April 2014 included students and instructors from the following five programs: Medicine, Nursing, Pharmacy, Physical Therapy, and Speech-Language Pathology. All faculty presenters were provided guidelines on specific points to cover education, licensing, scope of practice, etc. These sessions were aimed at providing students with informational content regarding various health disciplines and identification of misconceptions and stereotypes that commonly occur.
Large-group IPE Session 1 (January 2014–-1st IPE iteration)
This 90-minute session began with a short presentation introducing the importance of IPE, core interprofessional competencies, and characteristics of optimal teamwork collaboration and communication. In order to reinforce the importance of optimal interprofessional communications, the video recording by the University of Toronto's Center for IPE entitled “Student experiences in interprofessional education” 14 was shown with time reserved afterward for small-group and large-group discussions. The final exercise in this IPE session called for students listing words (representing preconceived biases) that they identified with each profession on a white board at the front of the room corresponding to each profession. Faculty representatives from each program then led a discussion about these biases, how they were formed, and why they were not necessarily accurate. These representatives then dedicated time to provide the whole group of students a brief overview of their profession using, in part, the aforementioned student-generated descriptions.
Session objectives, drafted by faculty, included the following:
examine the emerging importance of IPE and practice;
review the core fundamentals of IPE and care; and
explore the scope of practice for various healthcare professions and initiate dialog to improve teamwork communication and promote effective care delivery.
Large-group IPE Session 2–-collaborative practice (April 2014–-1st IPE iteration)
Faculty from various professions gave short presentations to the large group of students on the importance of communication between the healthcare provider and patient, and among health professionals themselves. The importance of collaborative practice in the patient-centered environment was also stressed. Two student learning activities focusing on the importance of communication and team building were included.
Session objectives, drafted by faculty, included the following:
further increase in understanding of the importance of interprofessional collaboration;
continue to increase knowledge about and respect for various healthcare professions and their contributions in healthcare delivery as members of the interprofessional team;
become comfortable with future professional collaborations through continued work with other students from various health fields; and
use language that is patient centered, nonambiguous, and can be recalled by the patient through teach-back strategies.
IPE iteration 2 (2014–2015 academic year)
The second iteration of the IPE program (2014–2015) consisted of a large-group session similar to the first interactive session from the inaugural year but included eight representatives of various health professions programs. Session 1 in January 2015 included students and instructors from the following seven programs: Medicine, Nursing, Pharmacy, Physical Therapy, Physician Assistant, Social Work, and Speech-Language Pathology, whereas Session 2 in April 2015 included students and instructors from all eight programs as follows: Medicine, Nursing, Pharmacy, Physical Therapy, Physician Assistant, Social Work, Speech-Language Pathology, and Athletic Training. A case-based small-group PBL session was included in the second iteration of the IPE program for the academic year.
Large-group IPE Session 1 (January 2015–-2nd IPE iteration)
In the second iteration of Session 1/introductory IPE (January 2015), prework assignments were added, which consisted of an interprofessional learning readiness questionnaire and a prereflection activity, which required the students to list at least five words or phrases describing their thoughts on each profession, who would be taking part in the program, their level of confidence in understanding each profession, and their perceived comfort level working with the different professions.
Prior to the second iteration of the IPE Session 1, some modifications were made based on previous student participation and at the suggestion of the IPE team. In addition to the Session 1 objectives used during the first IPE iteration (January 2014), students were required to generate their own learning objectives; however, guidance from faculty was provided. After completion of the session, students submitted their objectives along with a self-assessment of their success and achievement in meeting their stated objectives.
Small-group IPE Session 2–-PBL (April 2015–-2nd IPE iteration)
Based on student feedback from the first year of the program, and because of College of Medicine's reliance on CBL in the medical education curriculum, PBL was added as a method of delivering an IPE experience to students. This session was the first introduction of PBL as a method of delivering an IPE experience to students. Prior to the session, students were assigned readings and case guidelines, selected by participating IPE program faculty, to prepare for the experience.
Session objectives, drafted by faculty, included the following:
demonstrate professional behaviors by facilitating the practice of actively listening, engaging, and exchanging information with peers and other healthcare professionals;
work respectfully and effectively with others as a member or leader of a healthcare team, and identify major roles and responsibilities of each profession;
advocate for quality patient care and identification of ways to assist patients navigating system complexities;
identify the key personnel on the healthcare team who can advocate for the patient; and
discuss ways to provide care to patients who are unable to pay and advocate for access to health care for members of underserved populations.
The PBL case was written with input from all program faculty with the goal of fostering interprofessional communication and collaboration. To provide equal representation, the PBL case incorporated content from each of the eight disciplines that was represented in the IPE program. As can be seen in the example excerpt (Fig. 1), case questions were designed to allow each member the opportunity to discuss his/her knowledge of the case in the context of their specific profession. The faculty purposefully added case content to include examples of miscommunication or inappropriate interaction between health professions representatives in an effort to foster interprofessional dialog and problem-solving. This allowed for conversations relating to their role as a member of a healthcare team.

Excerpt from an IPE PBL case.
Students were divided into small interdisciplinary teams of approximately eight students each. Each group was facilitated by a faculty member from one of the eight participating professions. Prior to the session, facilitators from each profession were recruited and trained by an experienced PBL facilitator.
In their small groups, teams first established ground rules for the conduct of the session and designated specific roles for members of the team such as scribe and time keeper. The team spent 60 minutes working through the case, followed by a 10-minute debriefing and discussion on their group process and consensus on whether learning objectives were met.
Data collection and assessment
A session evaluation, specifically designed for each IPE session, was completed by students at the end of each session. The satisfaction survey consisted of a forced Likert-style response (four choices ranging from Strongly Disagree to Strongly Agree) and a comments section. The evaluation asked students to rate their level of agreement with the following questions about the IPE session: achievement of learning objectives, session usefulness, session organization, quality of presentation, and student interest in additional IPE sessions. Because small-group faculty facilitators were monitoring the IPE group PBL discussions, they were able to determine in real time whether students were meeting the session learning objectives. The case and facilitator guide were designed to prevent students from moving forward in the discussion unless learning objectives were attained. Facilitators were instructed about how to guide discussion to ensure completion of learning objectives. Because of this, students were not asked to formally evaluate their agreement with whether they met learning objectives for small-group IPE Session 2–-PBL (April 2015–-2nd IPE iteration). The percent of students strongly agreeing or agreeing with each of the evaluation statements is shown in Table 2. An average score for each question is also included in Table 3. Differences in scores for each question, between iterations of IPE sessions, were compared using independent group t-tests with a P-value of 0.05 used to determine statistical significance.
Percent of students who strongly agree or agree with IPE evaluation questions.

Question not asked as achievement of learning objectives was evaluated by group consensus and small-group facilitators.
Average score # (standard deviation) for each IPE evaluation question.
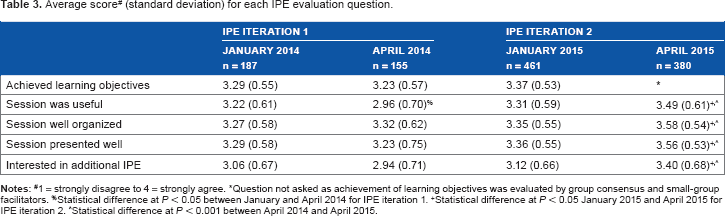
1 = Strongly disagree to 4 = strongly agree.
Question not asked as achievement of learning objectives was evaluated by group consensus and small-group facilitators.
Statistical difference at P < 0.05 between January and April 2014 for IPE iteration 1.
Statistical difference at P < 0.05 January 2015 and April 2015 for IPE iteration 2.
Statistical difference at P < 0.001 between April 2014 and April 2015.
The comment section requested feedback on the aspects of the session the students liked the most and identification of areas that could be improved upon. Additional space was provided for other descriptive comments.
Our study was reviewed by the Central Michigan University and Ferris State University Institutional Review Boards (IRB) and they determined that our research does not meet the federal definition of research on human subjects because it is measuring satisfaction and achievement of course outcomes. By definition, it does not require IRB approval or oversight.
Results
Large-group IPE Session 1 (Jan 2014–-1st IPE iteration and Jan 2015–-2nd IPE iteration)
Overall, students were satisfied with the Introductory IPE sessions from both iterations of the program (Table 2). For each of the Introductory IPE sessions in each IPE iteration, an overwhelming majority of students agreed or strongly agreed that learning objectives were achieved, the sessions were useful, well organized, and well presented, and they also expressed interest in attending other IPE sessions. There were no statistically significant differences in student satisfaction between the 1st sessions for each IPE iteration (Table 3–-January 2014 vs January 2015).
Students’ comments supported satisfaction with these IPE sessions and also provided us with more direction toward improving this and other IPE sessions. Narrative feedback indicated that students valued the expertise of the faculty from each profession, and there was a great interest in small-group interactions with more opportunity to get to know students from other disciplines, through working together. The following examples illustrate student satisfaction and areas for IPE program improvement:
[I liked] experts commenting on their respective professions.
[I liked] discussing the roles of each profession and talking about the misconceptions.
Make it more interactive.
More time to speak to students at the tables.
Large-group IPE Session 2–-collaborative practice (April 2014–-1st IPE iteration)
This second session of the first IPE iteration consisted of a series of didactics from IPE faculty from various professions, followed by student activities that were continued from the first session of the IPE program. Positive ratings were again obtained (Table 2). It was clear from the January session evaluations that the students were drawn to more group work and, while this session was popular, students felt they were not provided with the interactive experiences they felt were necessary to qualify as an interprofessional experience.
Average scores for each evaluation question (Table 3) between the January 2014 session and the April 2014 session indicate that there were no statistical differences in level of agreement with each evaluation statement with the exception of the score for the usefulness of the session, which decreased from January 2014 to April 2014 (3.22 vs 2.96, P = 0.003). This difference in perception about usefulness may have been reflected in some narrative comments from students.
Student feedback about this session indicated a preference to work together as teams, solving problems using more realistic scenarios:
[I liked] interacting with my team. I enjoyed the team building exercises
[I liked the] interactive activities–-real-world applications and examples.
Possibly [make] the team scenarios more health care related, ie, mock cases.
[I would like] hands-on case studies that could involve all disciplines (ie, stroke) then work out what each profession would do and how we would communicate together. It would be neat to do activities like a case study or a more real simulation so that we learn about how to work with other professions…
Small-group Session 2–-PBL (April 2015–-2nd iteration)
The introduction of a facilitated PBL session in April 2015 resulted in improved student satisfaction results (Tables 2 and 3). Although the second session of the first IPE iteration was well received (April 2014–-Table 2), a larger proportion of students rated the second session of the second IPE iteration (April 2015–-Table 2) higher. There was a higher satisfaction rating for the PBL format (April 2015) when compared to the less interactive session that focused on IPE introductory content held in the first iteration of April 2014. While there was generally no improvement between the first and second IPE sessions of the first IPE iteration (January 2014 vs April 2014–-and in fact, the students rated the usefulness of the second session in this IPE iteration as statistically lower than the first), students in the second IPE iteration rated each component of the second session (April 2015–-Table 3) as statistically higher than the first session of this iteration (January 2015–-Table 3). Score increases on each question of the evaluation from January 2015 to April 2015 were significant at the P < 0.0001 level. In addition, score increases on each question of the second session (April 2014 vs April 2015) of each IPE iteration were statistically significant at the P < 0.0001 level with the April 2015 PBL session being rated higher.
Students’ comments highlighted the importance of working together with equal opportunities for representatives from each profession to contribute and cited the benefit that a well-trained facilitator can add to the experience:
[I liked] problem solving as a group and hearing other students’ perspectives.
Every member had a chance to take lead on the case.
I liked having a facilitator[.] She encouraged us to go beyond what we would have otherwise.
Discussion
Based on student and faculty feedback, the incorporation of IPE into the ICE program was a rewarding and creative means of training students in essential interprofessional collaboration skills by first presenting students with real-world experiences during their ICEs in clinical settings where they were required to observe and evaluate the interactions of teams of healthcare professionals. The program data indicate that these experiences, coupled with the opportunity to learn with, from, and about other health professionals in the didactic sessions, were well received.
Our findings, as evidenced by student feedback, are clear that the students experienced the benefits of an IPE program through working with students in other health professions programs. As further evidence, the College of Medicine students cited in their Independent Student Analysis (a required component of LCME accreditation), the program's ability to “help students develop the skills for eventually working in healthcare teams and collaborating with fellow practitioners” as one area that has shown improvement over the past year. Students specifically identified the opportunity to have a chance to learn about other professions as being important and that these sessions provide a venue to help break down barriers between professions. Additionally, students implied that the inclusion of early and positive impressions is very important to prevent the proliferation of the stereotypes associated with various health professions:
I enjoyed interacting with students of different professions. I noticed that we were all very supportive of each other and acknowledge what each profession brought to the team. I was pleasantly surprised as I was told to expect arrogance from students of other professions. (Student feedback)
The data also supported the inclusion of an interactive PBL session. Evaluation data collected following this session indicated an increase in student satisfaction with their IPE learning in a small-group setting. This method of content delivery allowed each student in each group to contribute to the discussion in a meaningful way. This alone could account for the increase in student satisfaction.
Regardless of how early an IPE program is initiated in a curriculum, students may already hold misconceptions and stereotypes of other health professions; 15 thus, an IPE program must be aware of this issue and design approaches that minimize this influence on learning outcomes. A prevalent stereotype that any IPE curriculum can begin to address early is the “myth of the lone physician”. 16 This stereotype sets physicians apart from the rest of the healthcare team and characterizes them as completely independent and all-controlling entities. Implementation of an IPE curriculum can lead to the beginning of a paradigm shift away from this type of thinking by students in different health professions and has the potential for making great strides in opening up communication, thus creating a more accepting and comfortable IPE encounter.
In order to address this issue in part, the programs chose students from the different professions who were within the first two years of their respective graduate programs, or in the case of Social Work and Athletic Training in the final years of their undergraduate education. Offering IPE sessions to students early in their education, after at least one term, allows for the students to gain a better understanding of the scope of practice within their own profession, but hopefully also introduces them to other healthcare professions before negative impressions and stereotypes are ingrained.
In order to create a successful interprofessional experience, it is paramount that every profession is part of the design, development, and delivery of these sessions. Instructors at an IPE session need to be able to present an expert overview of their health profession discipline and should also have a solid foundation and knowledge of IPE in describing the importance of the other professions:
I enjoyed listening to the instructors of each profession. It cleared up misconceptions and brought a greater appreciation to each field. Each member of the interdisciplinary team is invaluable to patient care plan and quality care. I truly believe that. (Student feedback)
All instructors/facilitators need sufficient training in IPE and the pedagogy being used. The College of Medicine uses case-based PBL sessions, and the faculty are well trained in creating and implementing these sessions. Not all programs taking part in the IPE activities, however, use PBL or CBL in their curriculum. Many of the IPE PBL facilitators asked for more faculty development and training. A few students reported that their facilitator ran the group more like a lecture than a PBL session. This could be a limitation to the study in that the different approaches to PBL facilitation may affect student responses on the evaluations. We intend to address this in future IPE events by making the first session a prerequisite for participation in the PBL and additional PBL facilitator training to ensure consistency across groups.
One of the most important considerations for academic programs planning for the inclusion of IPE is to remain vigilant and avoid accidentally including a negative value or stereotype in their IPE sessions–-ie, avoid the negative hidden curriculum. During implementation of IPE sessions, it appears from student feedback that we were not immune from the hidden curriculum. We were especially surprised by some feedback regarding our PBL case. This case was primarily written by physician faculty with input from the other professions. The feedback we received from a medical student showcases just how difficult it is to avoid the phenomenon of the hidden curriculum:
[…] the whole theme was based around how arrogant and ignorant physicians were–-which I did not appreciate. Need more on what a physician can do.
This was certainly not the intent of the case authors and was not predicted to be a concern. The case was, however, written to contain information that could be judged by students as either a “mistake” or as areas for further discussion and dialog toward more appropriate or beneficial interventions. The PBL case also included instances of miscommunication that could have occurred between healthcare professionals, patients, or both. Students were expected to recognize these situations and subsequently discuss and suggest improvements in the delivery of care.
While it seems impossible to completely avoid the unintended hidden curriculum because it is dependent on the perceptions of the individual taking part in the program, a program can and should continually strive to minimize this by learning from feedback following each iteration of the session.
Inclusion of various healthcare professionals in the creation and development of IPE session content can help to minimize the hidden curriculum of negative stereotyping and misinformation. Opportunities to positively highlight the interaction and dependency of one profession on another would go a long way toward creating functional, effective, and collaborative healthcare teams in the future.
Plans for future collaboration and learning based on lessons learned
One of the most commonly encountered challenges is management of an IPE program. Each institution has its own unique challenges, depending on the accessibility and characteristics of each professional college, program, and site. Currently, the College of Medicine IPE program includes more than 400 students from 8 professions distributed between 3 schools. These schools are at distant sites and each has its unique curriculum calendar. We are actively engaged in improving oversight and management tools for development and implementation of the IPE curriculum that is equally distributed. Much of this will come from dedicated support shared between the programs. We are also considering decreasing the number of students who participate in an IPE session at one time, without decreasing the number of professions represented.
Student perceptions of the physician being negatively promoted as arrogant (ie, the hidden curriculum) was a surprise, but in retrospect should have been predicted. Because the case purposefully involved mistakes and miscommunication, the attitudes and biases about who caused these problems could have been directly addressed through discussion prompts. Additionally, external reviewers from the different professions may have been able to pick up on those biases that were not intended by the authors.
Sufficient training for PBL facilitators is invaluable to the success of a case-based PBL session. Training needs to be directed at both faculty facilitation and student participation. Continued facilitator training may be warranted, which emphasizes the ability to deal with high stress conditions or student anxiety that could arise when students, who tend to be competitive with trainees in their own programs, are tasked with speaking to the importance of their own disciplines to others outside of their discipline. In our experience, facilitators reported that students from different programs initially felt a need to outcompete their peers by defending their own discipline-specific approaches to patient care. This dynamic may be handled by better preparing our facilitators to recognize and preempt such approaches by the students. Finally, even though a guide to PBL was given to the students, along with step-by-step instructions on how a PBL session runs, students inexperienced in PBL could benefit from one or more practice PBL cases prior to the event.
A future goal is to direct more effort toward increasing the number of IPE opportunities in our program. This will include increasing the number of interactive IPE PBL sessions in the curriculum. Based on our positive curricular experience at the College of Medicine with an interactive student-centered team approach, the success of the PBL-based IPE sessions, and the findings that PBL and IPE work well together, 17 we are directing more of our efforts toward developing additional PBL-based IPE sessions. Our experience with CBL, PBL, and TBL suggests maintaining the same student teams in subsequent IPE sessions. A consistent team has the potential to further improve the outcomes of the IPE program by building more cohesive learning groups that can be tasked with completing progressively more challenging sessions. Our initial approach will be to maintain the same teams between the two IPE sessions we currently run, with the ultimate goal of expanding the program to at least four sessions extending over two years.
It is clear that our goal of holding more than two IPE sessions per academic year will make managing the program even more challenging. The medical professional programs have very different academic calendars with little room for additional sessions, thus escalating the challenge of getting students and faculty from the different professions together. Literature is limited on this topic but introducing more technology to allow for online team-based collaborative sessions could be one solution to this challenge. Our curricular experiences are similar to those of King et al, 18 where technology issues and limitations will need to be overcome before such an endeavor. An online program could be used as a way to continue opportunities for IPE with initial in-person sessions to allow for the start of relationships among the students of the different professions.
We are also currently developing and improving metrics for evaluating the success of IPE sessions and their effectiveness as part of the larger ICE program. Literature is limited on this topic in relation to developing metrics for measuring outcomes related to IPE events. However, Herge et al 19 provided tools for implementation in simulated clinical skills scenario to measure attitudes toward healthcare teams, and team observations of information sharing, communication, and team interaction. These may be adaptable to our own IPE efforts. A monumental challenge is creating an evaluation tool that identifies direct effects of the IPE program over time from those that are a result of our integrated curriculum.
Modification of current session evaluation tools will include the addition of more IPE focused questions. To capture the effectiveness of all of the sessions in meeting IPE competencies, we will use surveys that focus on attitudes and behaviors at the beginning and end of the ICE program, followed by the creation of tools for following and evaluating the students in their clinical years.
The development and implementation of quality IPE initiatives in student learning, no matter what the health discipline may be, is crucial toward meeting the needs of the patients we serve, and to that end, we believe it is worth the challenges we face.
Author Contributions
Conceived and designed the experiments: DPG and MCM. Analyzed the data: DPG and JMC. Wrote the first draft of the manuscript: DPG. Contributed to the writing of the manuscript: DPG, JMC, JJGR, MCM, LAB, EAP, and LAS. Agree with the manuscript results and conclusions: DPG, JMC, JJGR, MCM, LAB, EAP, and LAS. Jointly developed the structure and arguments for the paper: DPG, JMC, and MCM. Made critical revisions and approved final version: DPG, JMC, and MCM. All the authors reviewed and approved the final manuscript: DPG, JMC, JJGR, MCM, LAB, EAP, and LAS.
Footnotes
Acknowledgments
We are grateful to all of our colleagues and students at the three institutions who took part in our interprofessional education activities. We would also like to acknowledge the contributions of Janet Gabel, Coordinator of Clinical Education at Central Michigan University College of Medicine for data collection, and Dr. Barbara Wieszciecinski, Director of Nursing at Mid-Michigan Community College, for providing feedback on an early draft of this paper.