
Abstract
Background
Students' perception of their educational environment has a significant impact on their behavior and academic progress. The recent worldwide usage of innovative problem-based learning (PBL) medical programs requires major changes in medical schools and their environments. Therefore, measuring students' perceptions of the complex PBL environment has become a critical necessity as a determinant of students' academic success and as a part of attaining the quality standards of education. Ours being a new medical college employing the PBL curriculum, it was important to measure the students' perception of the educational environment in order to identify the strengths and weaknesses of the curriculum and to plan for any future improvements.
Aim and Objectives
The aim of this study was to evaluate students' perceptions in the preclinical phase of the PBL educational environment in the College of Medicine, Sharjah Medical College, United Arab Emirates, and to recommend remedial procedures.
Material and Methods
In this cross-sectional study, the English version of the Dundee Ready Education Environment Measure (DREEM) inventory was submitted to 250 students in years 1, 2, and 3. The data were analyzed using the SPSS 20 software, and significance was taken at
Results
Two-hundred and fifty students responded to the questionnaire (100% response rate). The overall DREEM score was 113.4/200 (56.7%). First-year students expressed higher overall significant level of perception (119.4/200) than second-year (107.4/200) and third-year (112.7/200) students. In addition, first-year students perceived their learning, teaching, and academic climates as more significant than the other two batches. The scores obtained in the five domains were as follows; 28/48 in perception of learning, 26/44 in perception of teaching, 18/32 in academic self-perceptions, 27/48 in perceptions of atmosphere, and 15/28 in social self-perceptions. First-year students achieved the highest score (18.7/32) in the academic self-perception, and second-year students achieved the lowest (16.5/32). The total score was significantly higher in female students than in male students (115.9 vs 108.1).
Conclusions
The present study revealed that the PBL environment is generally perceived positively by our medical students. Female students exhibited higher perception than male students. Nevertheless, areas such as curriculum overload and inadequate student support still require further fine-tuning and remedial measures.
Keywords
Introduction
Educational environment (EE), climate, or milieu, is everything that is happening in the classroom, department, faculty, or university, and it is vital in determining the progress of undergraduate medical education.1,2 EE is a key component of the curriculum, 1 and its measurement should be part of curriculum evaluation. 3 Although EE has been less studied in the literature than content, teaching methods, or assessment, it is, nevertheless, of equal importance. 3 Medical students experience a variety of learning activities in the environs of the medical college, which are usually complex and unique. 4 Modern strategies in learning methodology and innovative curricula are shifting more toward student-centered learning approaches. 5 Consequently, the organizational and educational environments are likely to be altered and become more complicated. This might explain the recent growing interest in measuring students' perceptions of EE 6 in many medical schools, 7 particularly those adopting integrated and problem-based learning (PBL) programs. According to Vygotsky's theory of social cognitive development, 8 EE is the “culture” that determines students' learning development. In classrooms, clinical wards, and community health centers, students' learning scaffolding and development take place when interactions between students and teachers, peers, and other health care professionals occur. With the existence of friendships (high affiliation) and teacher support in classrooms, students' level of learning would be improved. In other words, EE is the “culture” that teaches students how to think and acquire knowledge, skills, and attitudes through the classroom environment.
The quality of the EE has been recognized to be vital for effective learning in terms of students' achievement, happiness, motivation, and success.4,9–11 Additionally, EE is one of the most important factors determining the effectiveness of the curriculum, 12 and its role has been stressed as being the curriculum's most significant manifestation and conceptualization.13,14 Gender differences in perceptions of the EE might well emerge in particular academic or cultural contexts, with particular curricula. A comparative study of data from a Nigerian undergraduate medical school and a Nepalese health professional institution reported that female students seem to be significantly less pleased with the EE in these institutions.15,16 In addition, it is important to monitor students' perceptions of EE at different stages and in different forms of curricula. The UK Standing Committee on Postgraduate Medical Education 17 highlighted the importance of EE by stating that “A working environment that is conducive to learning is critically important to successful training”. Furthermore, the World Federation for Medical Education (WFME) singles out the “learning environment” as one of the “targets” for what it terms “the conduction of the evaluation of medical education programs”. 18 For measuring such an environment, Roff et al (1997) 19 developed the Dundee Ready Education Environment Measure (DREEM) inventory, which has been used diagnostically to identify areas of the strength and weakness in a medical EE.12,15 In addition, it has been used to compare different medical educational institutions,15,20 students at different stages of the course,15,21,22 and male and female students.15,16,20,21 It has been used to measure the existing EE as a precursor to curriculum change, to identify priority areas for change, and to act as a baseline for comparison after curriculum change.21,23
Organizational context
Sharjah Medical College (SMC) is one of the 13 colleges of the University of Sharjah, United Arab of Emirates, and was founded in 2004. It offers a six-year MBBS program in three educational phases. Phase 1 is the foundation year and phase 2 is the preclinical phase, which includes years 1–3 and is followed by a comprehensive exam. Students in years 4 and 5, ie, the clinical phase 3, undergo rotational clinical trainings in public hospitals in Sharjah. Since its foundation, SMC has adopted an innovative PBL with integrated, student-centered, competency-based, and community-based curriculum in all phases of the program. Students of SMC are from mixed nationalities; although the majority is from the United Arab Emirates and Arab countries, they have diverse cultural backgrounds and come out of different educational systems. Moreover, male and female students undergo coeducation without segregation within the classrooms. Though the individual components of our curriculum are periodically monitored, EE has not been assessed since the first implementation of its curriculum 10 years ago.
Therefore, the aim of the current study was to monitor the perceptions of students about their EE in the PBL-based curriculum in SMC using DREEM. We assume that both the strengths and weaknesses would be identified. The results might offer a starting point for implementing measures toward curricular reform. The objectives of the study were as follows:
How students perceive the educational environment in the PBL curriculum;
Whether there is any gender difference in the students' perception;
How students at different levels (years) perceive the educational environment;
The perceived strengths and weaknesses of the curriculum.
Subjects and Methods
Population and samples
All undergraduate medical students of years 1–3, ie, the preclinical phase of the SMC, were invited to participate in this cross-sectional study. The total number of enrolled students in the three batches was 301, with 111 in the first year, 97 in the second year, and 93 in the third year. The current study obtained ethical clearance from the SMC.
Instrument for data collection
The DREEM inventory is a widely used, culturally nonspecific, and generic instrument developed to analyze undergraduate EE in the health profession.16,19,21 It has been found to be a validated tool19,24 with proven high reliability15,19,24,25 and has been applied in a variety of cultural contexts in various countries worldwide. With its help, medical institutions can identify the deficient areas in the learning process and then effect the required changes in curriculum.4,19,26–28
DREEM was developed at the University of Dundee in 1997; 19 and was universally tested in Europe, Africa, Asia, Australia, and America. 15 The inventory consists of 50 items categorized under five domains, namely Students' Perception of Learning (SPL, 12 items with a maximum score of 48), Students' Perception of Teachers (SPT, 11 items with a maximum score of 44), Students' Academic Self-Perception (SAP, 8 items with a maximum score 32), Students' Perception of the Atmosphere (SPA, 12 items with a maximum score of 48), and the Students' Social Self-Perception (SSP, 7 items with a maximum score of 28). The maximum score for all domains is 200, indicating the ideal EE. Each item is scored using a 5-point Likert scale with 4 for strongly agree, 3 for agree, 2 for uncertain, 1 for disagree, and 0 for strongly disagree. However, 9 out of 50 items, ie, items 4, 8, 9, 17, 25, 35, 39, 48, and 50, were negatively phrased statements and have scores 0 for strongly agree, 1 for agree, 2 for uncertain, 3 for disagree, and 4 for strongly disagree. Taking into account these maximum scores, the data are converted into percentages of their respective domains. 29 The approximate interpretation of the DREEM overall score is as follows: 0–50: very poor; 51–100: plenty of problems; 101–150: more positive than negative; and 151–200: excellent. An approximate guide for interpreting the five DREEM domains is summarized in Table 1. To pinpoint more specific strengths and weaknesses within the EE, items with a mean score >3 are considered positive, while items with a mean score of ≤2 are considered as problem areas, and were identified in the study population. Items with a mean score between 2 and 3 are considered as aspects that could be improved.30,31
Approximate guide for the interpretation of the five DREEM Domains.30,31

Data collection
Data collection was done in March 2014. A mid-semester week was selected for the survey in order to avoid the dominant effect of stress of the pre-final exams on student responses. The English version of DREEM inventories was submitted to 250 students in the first, second, and third years personally on three separate occasions in their classrooms. Before starting the survey, the author briefly explained the objectives and importance of the study and cleared the doubts about the questionnaire items with special emphasis on the importance of voluntary participation and the anonymity of the process. All students responded positively, and returned the questionnaires after about 30 minutes, thereby avoiding discussions among them. A separate consent form was collected along with survey. No ethical issues were encountered during the course of this process. Although the total number of the registered students in all three years was 301, only 250 students were available at the time of data collection (83%). The valid questionnaires collected and analyzed were 250, ie, 100% response rate.
Data management and analysis
The returned questionnaires were examined for completeness and consistency. Data were entered in MS-EXCEL, and were analyzed using IBM SPSS PC + statistical software (version 19). As the study outcome variables (scores of five domains and total score) are continuous variables, they were quantified by their mean and standard deviation. Student's
Results
The mean age of the participants in the study was 20.3 (±0.04) years, in the range 17–23. Two-hundred and forty-five students specified their genders, while five did not. The study included 170 women (69%) and 75 men (31%). The total number of the analyzed questionnaires was 250, distributed as 98, 91, and 61 from years 1, 2, and 3, respectively.
The overall mean DREEM score of this study was 113.4/200 (56.7%), which was interpreted as “more positive than negative”. Regarding the five domains of the DREEM inventory, ANOVA test revealed significant differences among the three groups in the overall mean scores as well as in the SPL, SPT, and SAP domains (Table 2). When compared to those in years 2 and 3, year 1 students exhibited the highest level in their total perception of EE as well as in SPL and SPT domains. However, in the SAP domain, year 1 students revealed a significantly higher perception than year 2 students.
ANOVA between means (±SD) with percentage of the different years for the differing DREEM domains, along with the interpretation of the total values (n = 250).
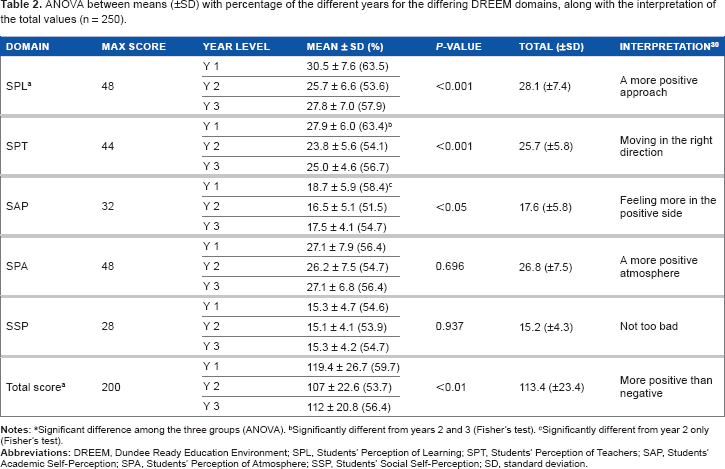
Significant difference among the three groups (ANOVA).
Significantly different from years 2 and 3 (Fisher's test).
Significantly different from year 2 only (Fisher's test).
Neither the SPA nor the SSP domain showed significant difference among the three years. For assessing the weaknesses and strengths of the EE, the guide of Mcaleer and Roff 30 was used to interpret the mean scores of the five domains of DREEM (Table 2). Figure 1 shows that the majority of SMC students (72.1%) exhibited excellent and positive perceptions e.g. scored 50% and above to the overall DREEM inventory.
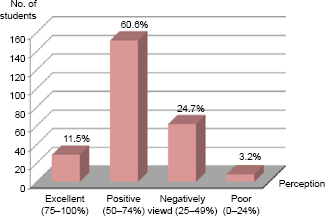
Percentage of overall SMC students' perception of the educational environment (n = 250). Abbreviation: SMC, Sharjah Medical College.
Table 3 shows the detailed scores of DREEM's individual items. The overall mean score (±SD) was 2.26 (±0.39), which is interpreted as “educational aspects that could be improved”. Out the 50-item scores, one item, ie, item 15
Mean (±SD) of the DREEM item scores (Max = 4).
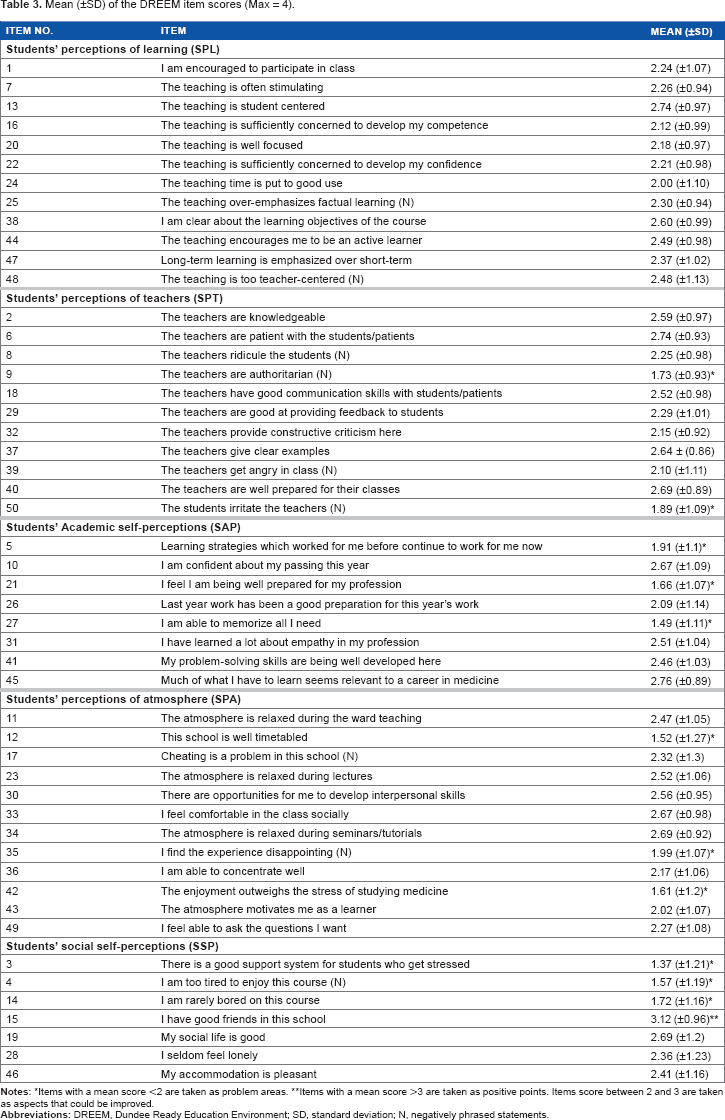
items with a mean score ≤2 are taken as problem areas.
items with a mean score >3 are taken as positive points. items score between 2 and 3 are taken as aspects that could be improved.
Demographic differences
Statistical analysis showed that female students exhibited a significantly higher perception of EE than male students in the overall DREEM score as well as in the SPL and SPT domains (Table 4).
Comparison of DREEM domain mean scores (±SD) for male and female students.

Significantly different (
Discussion
It has been reported that assessing EE should be a part of an institution's good educational practice. 34 Considerations of EE in the medical school along the lines of continuous quality improvement and innovation are likely to further the medical school as a learning organization with the attendant benefits. 1 As SMC is a new medical college with an innovative PBL curriculum, it was essential to assess the EE of the SMC in order to implement the required reforms. Students' perceptions of the EE may be influenced by their expectations about the educational program, diversity of the student population, variations in the style of teaching of the faculty, educational facilities and equipment, and other circumstances of the university. 35 Review of the literature shows the wide use of DREEM inventory in medical9,16,36 and dental schools.37, 38
The response rate in the preset study was 100%, which is a perfect indicator about student's interest in completing the survey and their interest to develop their institution. This is likely due to using face-to-face methodology rather than using an online survey. In the current study, the overall DREEM total mean score was 113.4/200, indicating that the SMC students' perception of the EE is more positive than negative. On the other hand, it indicates that there is vast room for improvement, as there is no curriculum without weaknesses.
SMC adopts a student-centered educational model where students are the center of the learning process and an integrated PBL curriculum with team-based teaching methodology. The teacher's role changes to a facilitator of learning rather than an information giver. This model is in contrast to the traditional teacher-centric norms. Therefore, it would be useful to explore the different perceptions of EE in PBL versus traditional curricula. The overall score of DREEM inventory of the current study (113.4/200) was not very much different from those of other studies carried out regionally and internationally. In comparison with other studies conducted in PBL medical curricula, the score of this study was similar to the scores of 113.8/200 in Egypt 39 and 114.4/200 in Pakistan. 40 However, it was higher than that in KSA, 41 Kuwait, 42 and Sri Lanka, 43 which reported mean DREEM scores of 111.5/200, 105/200, and 107.4/200, respectively. On the other hand, our mean score was lower than the scores of 143/200 in a dental school with an enquiry-based curriculum in the UK, 37 137/200 in Australia, 44 and 139/200 in the UK. 45 In comparison with the scores reported from traditional and teacher-centered curricula, our DREEM score was higher than that in King Saud University (90/200), 9 King Abdul Aziz University (102/200), 23 and Umm Al-Qura University (107/200) in KSA; 46 Sana'a University (100/200) in Yemen; 20 and Iran (99/200). 47 Some studies have reported a more positive EE mostly after making some educational reforms toward innovative curricula, such as in UAE 48 and Chile. 49 Furthermore, comparable studies performed in different institutions with traditional versus PBL curricula concluded that students of PBL curricula would evaluate their EE more positively than their counterparts in primarily conventional curricula.20,26 This highlights the importance of the positive influence of the new educational strategies in the innovative curricula on students' perceptions of EE rather than traditional programs. It seems that the integrated and student-centered curricula stimulate and provoke students to be active learners; also, they develop and evolve their skills. 50
The scores of our study show that year 1 students displayed a higher positive perception of EE than year 3 students. However, year 2 students exhibited the lowest mean scores of perception. These findings are consistent with the results of in King Saud University. 9 In addition, this is similar to the finding in a previous report that students who had enrolled at the school for a longer period became less satisfied with the teaching and with the support system for stressed students. 19 Al Ayed and Shiek 9 suggested that this might simply mean that first-year students were not too stressed (yet) by their studies. It became clear that students lost some of the neutrality that they exhibited in the first year and became more critical of the EE as they progressed through the program. It could also be explained by the enthusiasm and excitement of first-year students on successfully gaining entry into the medical college. 9
In the current study, the scores of the domains were SPL 28.1/48, SPT 25.7/44, SAP 17.6/32, SPA 26.8/48, and SSP 15.2/28. Most of the items, ie, 38 items, received mean scores between 2 and 3, which could be enhanced.
30
On the other hand, the problem areas, or the DREEM items that scored ≤2, were 11 items; none of them was in the learning domain. Out of the 11 items, 2 are related to the teachers domain
The results showed that the whole groups exhibited the highest level of perception in the SPL domain, which is perceived as a positive approach. The agreement of all students groups on the SPL is crucially important for the PBL curriculum of the new SMC.
On the basis of the scores of the individual items of the DREEM inventory of the present study, attention will be paid to the areas that need improvements, and recommendations would be made for rectification. In the SPT domain, the majority of our students agreed that
Although year 1 students achieved the highest score in the SAP (18.7/32), year 2 students achieved the lowest (16.5/32) score in the same domain. Such a difference might be related to the heavy load and timetabling in year 2, which need considerable attention. Reorganization of the timetable and well-communicated, explicit learning objectives with pre-class preparation material are the need of the hour in this concern.
Item 5
Item 27 (
Regarding the SSP domain, all the participating students in this study shared the lowest perception (1.37) of item 3
Our results revealed a significantly higher perception of the overall score among female students than male students (115.9 vs 108.1). This is in agreement with the results reported in the studies from Trinidad, 12 Argentina, 16 India, 35 the UK, 56 Malaysia, 61 and Australia.44,53 On the contrary, gender showed no statistically significant difference in Canada, 22 India, 13 and King Saud University, Saudi Arabia. 9 Additionally, female students' responses were statistically significantly in their positive perception of learning when compared with those of males (28.8 vs 26.6). This might be explained by the differences observed in learning styles between male and female undergraduates. 62 Female students generally spend more time studying compared to males, 36 and are more critical about the quality of teaching and the general climate of the school, especially in the areas of student participation in class and the authoritarian attitudes of teachers. 16 Within the context of the current research, where the conservative and traditional culture of the Middle East countries dominate, females have less chance for spending time in extracurricular activities than males. However, the studies performed in Saudi Arabia and Yemen medical universities20,23 revealed less perception of EE among females than males. This contrast might be due gender segregation in these universities. Furthermore, female students demonstrated more positive perceptions toward teaching than male students (26.4 vs 24.2). Research findings show that female students develop more trust toward their lecturers when compared with males. 63
Conclusion
On the basis of the results of the present study, it can be concluded that the overall perception of SMC students of the EE is more positive than negative. The ultimate outcome was that the integrated PBL curriculum of the newly established institution is moving in the right direction. Gender differences and year level of students showed significant variations regarding the perception of the EE. Nevertheless, as identified by the DREEM inventory, many problem areas need to be critically investigated and remedied. Therefore, DREEM inventory is an effective tool in identifying the strengths and weaknesses of the curriculum. The message our students try to convey to us is that we need a support system for the stressed students, more motivating teaching instructions, reducing the curriculum overload, and better timetabling in order to enjoy the atmosphere and attain better outcomes. Consequently, the study strongly suggests presenting these results to the relevant educational and administrative authorities and decision makers for utilizing them as the basis for strategic planning and resource utilization. In addition, the results should be used as guidance to institutional corrective actions regarding the students' perception of areas of concern.
Limitation and Recommendations
As there is no comparable data from previous studies performed in the context of SMC, the results of the current study could be accepted as a baseline for further studies. The sole use of the questionnaire as a quantitative method of data collection might be a limitation of the current study with the possibility of leaving out some specific components of the context. 64 Another limitation is that the individual items were not analyzed by parallel qualitative data. Therefore, future qualitative studies may help confirm the current findings and more deeply address the specific problems or highlight strengths within the college.
Author Contributions
Conceived and designed the experiments: RMM. Analyzed the data: EN. Wrote the first draft of the manuscript: RMM and EN. Contributed to the writing of the manuscript: EN and RMM. Agree with manuscript results and conclusions: EN, RMM, and ZM. Jointly developed the structure and arguments for the paper: EN and ZM. Made critical revisions and approved final version: EN, RMM, and ZM. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgment
We are extremely grateful to all SMC students who took part in this study.