
Abstract
Osteoporosis is associated with compromised quality of life (QOL), to which pain has the most important contribution. Elcatonin, a derivative of calcitonin, is widely used in the treatment of osteoporosis in two ways. One is as the inhibitor of osteoclastic bone resorption. The other is for osteoporosis-related pain based on the unique analgesic effects of elcatonin. Since pain is subjective in nature, and QOL is the only clinical outcome representing the patients’ subjective perception of health status, pain associated with osteoporosis would be best evaluated based on QOL assessment. Evidence based medicine gives the highest remarks to the double-blinded, randomized controlled trial, which, however, cannot be free from methodological problems on some occasions. For example, it is practically impossible to remain blinded in the trial of a potent analgesia, which in turn causes biases. Thus, the significance of taking the patients’ preference into account is increasingly acknowledged. In this study, 45 osteoporotic patients were given brochures describing the pros and cons on the three treatment choices; calcium and alfacalcidol, additional use of elcatonin, and additional use of bisphosphonate. Those who favored elcatonin were older, had more vertebral fractures, and lower QOL scores. QOL was evaluated before and three months after the treatment using SF-8; the most widely used generic questionnaire, and RDQ; a lumbago-specific measure. Elcatonin treatment improved physical function, general health, and vitality of SF-8, and RDQ score. Although this is a preliminary study, our results suggest that patients with vertebral fracture(s) have impaired QOL and more likely to favor elcatonin treatment expecting analgesia.
Introduction
Calcitonin is a hormone secreted from the para-follicular cells of the thyroid gland. It is involved in calcium homeostasis by inhibiting osteoclast-mediated bone resorption and decreasing serum calcium levels. It is clinically used in various clinical conditions. For example, it is prescribed to osteoporotic patients,1–3 especially those with enhanced bone resorption. Additionally, it is a therapeutic drug in the treatment of malignancy associated hypercalcemia. 4
Elcatonin is a derivative of calcitonin 5 with potent analgesic action. 6 Therefore, it is clinically administered to osteoporotic patients with pain.7,8 Japanese guidelines for the prevention and treatment of osteoporosis have given grade A, the highest possible mark, to the analgesic action of elcatonin. 9
Of the various measurement scales clinically available, QOL (Quality of Life) is the only clinical outcome representing the patients’ subjective perception of health. 10 Pain is subjective in its nature, and could be evaluated only by subjective index: QOL. It follows that the analgesic effect of elcatonin would be best evaluated with QOL as the outcome. A theoretical problem arises, however, if one attempts to evaluate the analgesic effects of a certain drug based on QOL scores.
Recently, the concept of evidence based medicine (EBM) has been advocated in which, a hierarchy of evidence exists, with double-blinded randomized controlled trial (hereafter in this paper, abbreviated as DB-RCT) given the highest remark. DB-RCT is considered to be least affected by various biases. In some types of trials, however, double-blindness or randomization cannot be strictly guaranteed with DB-RCT, and even DB-RCT cannot be free from such biases. As will be detailed in the “Discussion, some forms of bias” to skew the results is known to take place in studies in which blindness or randomization is disrupted.11,12 Thus in this paper, we have attempted to study the effects of elcatonin treatment on the QOL of osteoporotic patients taking the patients’ preference into account.
Subjects and Methods
Subjects
Forty-five (42 females, 3 males) osteoporotic patients with back pain or lumbago were encouraged to participate in the study. The diagnosis of osteoporosis was made based on the diagnostic criteria for primary osteoporosis in Japan. 13 The purpose of the study was explained, and written consent was obtained. Ethical approval was obtained for the use of humans in this research
The exclusion criteria were as follows. Patients receiving bone-active drugs were excluded unless they were drug free for 48 weeks for bisphosphonates and for 8 weeks for other drugs. Patients under sustained analgesic treatment were also excluded unless the analgesics were halted for at least 2 weeks. Patients were also excluded when the attending physician made a judgment that the patient was not eligible for entry based on the clinical condition.
Vertebral fractures were diagnosed based on a plain roentgenogram. The diagnosis of compression fracture was made by one of the authors (KY) before obtaining the information on QOL.
Intervention Protocol
The study design was an open-labeled one based on the patients’ preference, further details of which will be described below. There were three treatment groups; group (1): calcium lactate 1 g or calcium aspartate and 1 μg of alacalcidol daily, group (2): once-weekly injection of elcatonin in addition to the regimen in group (1), and group (3): alendronate 5 mg daily or risedronate 2.5 mg daily in addition to the regimen in group (1). Patients were given brochures describing the pros and cons of each treatment, and asked to select the treatment of their preference. Six, twenty-seven, and twelve patients chose group (1), group (2), and group (3) treatment, respectively.
QOL (Quality of Life) Evaluation
QOL was evaluated with two questionnaires; SF-8 and RDQ (Roland Morris Disability Questionnaire). SF-36 is a generic (non-disease specific) QOL questionnaire, and one of the most widely used worldwide. SF-8 is an abridged edition of SF-36. According to the authorized instruction, the data were transformed to the deviation value adjusted by Japanese national norms.14,15 Eight subscales were obtained: PF (physical function), RP (role physical), BP (bodily pain), GH (general health), VT (vitality), SF (social function), RE (role emotional), and MH (mental health). These scores are further summarized into two summary scores: PCS (physical component summary) and MCS (mental component summary). These subscales and summary scores are interpreted as follows: 50 corresponding to the national norms, and 40 indicating one standard deviation lower than the norm.
RDQ is a questionnaire specifically targeted to lumbago. It is composed of 24 questions. The subjects are asked to give “yes” or “no” to each question. Total number of questions given “yes” is calculated. Thus higher number is associated with more severe lumbago.16,17
QOL evaluation was made before and three months after initiating the intervention.
Statistical Analyses
Data were analyzed using SPSS 17.0J for Windows. Comparison of three independent groups was done with one-way analysis of variance (ANOVA) followed by Tukey's test as the post-test. Contingent tables were analyzed by the chi-square test. Statistical significance was judged based on P < 0.05.
Results
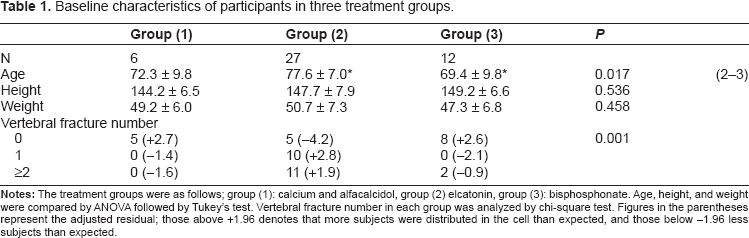
Table 1 shows patients characteristics. Patients in group (2) were significantly older than those in other groups, but there was no significant difference in their height or weight. All patients in group (1) and most in group (3) had no vertebral fractures. In contrast, most patients in group (2) had vertebral fracture(s). These differences were statistically significant based on chi-square test.
Baseline characteristics of participants in three treatment groups.
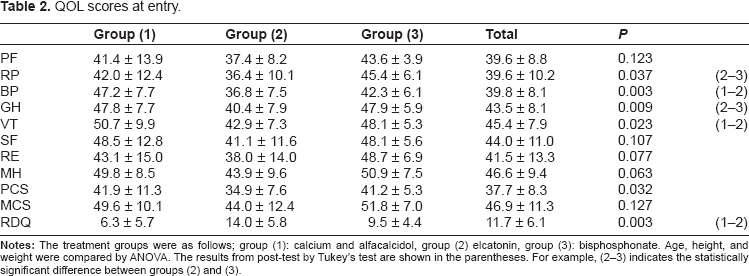
Baseline QOL scores are shown in Table 2. There was a significant difference between the three groups in four of the eight subscales of SF-8; RP, BP, GH, and VT and total scores of RDQ. Patients in group (2) had worse QOL scores. Although not statistically significant, those in group (2) had worse QOL scores in practically all scales.
QOL scores at entry.
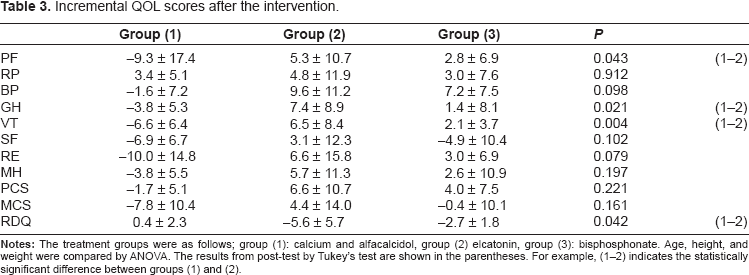
In Table 3 is shown the post-intervention changes in the QOL scores. Elcatonin treatment markedly improved in several subscales of QOL score.
Incremental QOL scores after the intervention.
Discussion
Osteoporosis is defined as a skeletal disorder characterized by compromised bone strength predisposing a person to an increased risk of fracture including vertebral, hip and wrist fractures. 18 Hip fracture is associated with high mortality and markedly impaired activity of daily living (ADL). It is not only a tragedy for the elderly individual, but also a great burden to society. 19 Vertebral fracture is the most prevalent osteoporosis-related fracture. 20 Recent studies have clarified that it is a fracture of great clinical importance associated with increased mortality, co-morbidity, and compromised ADL.21–23 Nevertheless, vertebral fracture has not received much attention until recently. One of the reasons for the ignorance of the importance of vertebral fracture is that approximately two-thirds of patients are without overt clinical signs. Its lack, however, does not necessarily mean that the patients are symptom free or subjectively well. Since QOL is the only index representing the patients’ subjective status, QOL would be quite suitable in the evaluation of patients with vertebral fracture.
Recently, many questionnaires for QOL evaluation have become available. They are classified into two major categories; generic and disease-targeted. Generic ones, by their definition, only consist of questions related to the subjects’ general status, and do not include questions related to the features which are specific to a certain disease. Therefore, they are applicable to such studies as comparing the impact of various diseases on QOL, or even to the evaluation of healthy subjects. In contrast, disease-targeted ones include items specific to a certain disease. They can be more sensitive than the generic ones in detecting the QOL impairment closely related to a certain disease state, but are not applicable to the evaluation of patients with other diseases. The most widely used generic QOL questionnaire is SF-36 and its abridged form, SF-8. 14
Roland-Morris Disability Questionnaire (RDQ) is rather different from the above-mentioned questionnaires, and unique in that it is specific to lumbago. 16
We have recently shown that patients with vertebral fracture(s) had compromised quality of life (QOL) and elcatonin treatment remarkably improved it. 7 In the course of the study, we have noticed a challenging problem. QOL evaluation could be done by giving the questionnaire to the subjects and asking them to mail it back. In this study, however, the patients’ QOL was evaluated by the interviewers considering that most subjects are elderly osteoporotic patients. The attending physician only obtained the consent to participate in the study without participating in the interview. The interviewers were blinded about the treatment regimen for each patient to minimize bias. Nevertheless, the blindness could not be maintained, since elcatonin treatment markedly relieved pain in some patients, whereas such marked improvement occurred in none of the subjects in the control groups.
Recently, such phenomena have been reported to be a challenging problem to DB-RCT, and the importance of patients’ preference has been recognized.11,24,25 Clinical studies are performed based on the assumption that subjects both in intervention and control arms are randomly sampled from a single population. In RCT, patients are conceptualized as relatively passive recipients of intervention. In reality however patients are far from passive, and in fact are quite active participants in the research. Therefore, patients often have preferences for a certain intervention, and will prefer one over the others where they are given the opportunity to choose.
In RCT, the possible interference is minimized by blinding. In some cases, however, participants know which intervention they have received. Then it is possible that patients not allocated to the intervention of their choice have lower compliance to the therapy, which will impair the validity of the study. Several theoretical frameworks have been developed to take the patients’ preference into account. 24
In this paper, we have attempted to study the analgesic effects of elcatonin considering the participants’ preference. When the patients were given brochures describing the benefit and possible side effects of each treatment, and asked which treatment regimen they would like to receive, those who preferred elcatonin were significantly older and more likely to have vertebral fracture(s). Those in the calcitonin group had lower SF-8 scores and higher RDQ scores, indicating more compromised QOL. Thus subjects with vertebral fracture(s) have impaired QOL, and are more likely to prefer elcatonin treatment expecting its analgesic effects.
Elcatonin treatment resulted in more pronounced improvement in the subjects’ QOL scores, although statistically significant in only some of the scores probably due to the limited number of patients studied.
This is a preliminary study to identify the analgesic effects of elcatonin taking the patients’ preference into account. Despite the limitations described above, patients with vertebral fracture(s) have compromised QOL, and are more likely to prefer elcatonin treatment, and more likely to be benefited by its treatment due to its potent analgesic effects.
Disclosures
Author(s) have provided signed confirmations to the publisher of their compliance with all applicable legal and ethical obligations in respect to declaration of conflicts of interest, funding, authorship and contributorship, and compliance with ethical requirements in respect to treatment of human and animal test subjects. If this article contains identifiable human subject(s) author(s) were required to supply signed patient consent prior to publication. Author(s) have confirmed that the published article is unique and not under consideration nor published by any other publication and that they have consent to reproduce any copyrighted material. The peer reviewers declared no conflicts of interest.