
Abstract
Background
The emerging role of vitamin D in immunology and autoimmune disorders has been a worldwide interest in the last decade. Systemic lupus erythematosus (SLE) patients are particularly at a delicate position predisposing them to suffer from vitamin D deficiency due to the multiple risk factors accompanying the disease. Whether vitamin D deficiency is also involved as a risk factor for developing SLE and affecting its course is a considerable concern.
Objectives
The objective of this study was to estimate the prevalence of vitamin D deficiency in SLE patients and its relation to disease. MATERIALS AND METHODS: In our observational cross-sectional study, serum levels of vitamin D [25(OH)D] in 60 SLE patients and 30 age- and sex-matched healthy controls were assessed and estimated for deficiency and insufficiency at 10 and 30 ng/mL, respectively. Disease activity was evaluated by SLE disease activity index (SLEDAI), irreversible organ damage by Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index (SLICC/ACR DI), and severity by Severity of Disease Index. Fatigue was measured by visual analog scale.
Results
Significantly lower levels of 25(OH)D were found in SLE patients (17.6 ± 6.9 ng/mL) in comparison to controls (79.0 ± 28.7 ng/mL), with a statistically high significant difference (t = -11.2, P < 0.001). High prevalence of vitamin D insufficiency and deficiency was detected as 73.3% and 23.3%, respectively. Vitamin D had a highly significant negative correlation with SLEDAI (r = -0.495, P < 0.001), SLICC (r = -0.431, P < 0.05), and fatigue (r = -0.436, P < 0.05).
Conclusion
Vitamin D deficiency and insufficiency were found to be prevalent in SLE patients in our study and related to disease activity and fatigue. If needed, routine screening and consequent repletion of vitamin D are recommended in SLE patients. Restoring adequate vitamin D levels in SLE patients should be more explored as a potential yet simple measure to their usual management to improve their condition.
Introduction
Vitamin D has a crucial role in calcium metabolism. Nowadays, a new era for vitamin D has emerged since it has been involved in immune modulation1,2 and in the risk for developing autoimmune diseases such as rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE).3–5
The conversion of 7-dehydrocholesterol into previtamin D3 in the skin, by the solar ultraviolet B radiation, is considered the main source of vitamin D, whereas only a smaller amount is obtained from food. 6
Vitamin D receptors (VDRs) have been identified on immune cell membranes, thus, together with existing 1α-hydroxylase in these cells, clearly underlining the importance of vitamin D for immune regulation.7,8 In addition, VDR genetic polymorphisms may affect their functionality and have an impact on immune regulation in autoimmunity. 9
Newly identified targets for vitamin D reveal multiple molecular pathways of anti-inflammatory actions for 1,25(OH)D3 in several immune cells. These include inhibition of prostaglandin (PG) synthesis and biological actions; inhibition of p38 stress kinase activation; inhibition of nuclear factor kB (NF-kB) signaling, which results in the attenuation of the synthesis of pro-inflammatory cytokines such as interleukin-8 (IL-8) via upregulation of the expression of insulin-like growth factor binding protein-3 (IGFBP-3); and inhibition of angiogenesis due to suppressive effects on the expression of pro-angiogenic factors such as hypoxia-inducible factor 1 (HIF-1) and vascular endothelial growth factor. 10
Vitamin D deficiency has been implicated in various rheumatic disorders. The risk of developing RA was found to be inversely related to vitamin D intake. 11 RA cases with low plasma 25(OH)D were found by some researchers to have higher risk of disease activity, 12 while others found no associations of serum 25(OH)D levels with disease activity. 13
SLE is a chronic inflammatory multisystem disease mainly affecting women of childbearing age. It is characterized by a very large spectrum of clinical manifestations accompanied by prototypic abnormalities of the immune system. 14
One aspect that is particularly pronounced is fatigue and musculoskeletal symptoms, which is experienced by up to 90% of SLE patients and is considered their most disabling disease symptom by ∼50% of patients. 15 This is often multifactorial in origin and can be mediated through disease-related factors, comorbid conditions, or environmental factors. 16
Commonly frequented SLE musculoskeletal symptoms and pain can be caused by vitamin D deficiency. Hence, the concomitant presence of such deficiency might be overlooked in these patients in spite of having multiple risk factors for its occurrence. Chronic steroid use may alter vitamin D metabolism, by reducing the level of dihydroxyvitamin D3, although there is contradictory evidence about it. 8 Additionally, hydroxychloroquine, often used in SLE, is suspected to decrease vitamin D2 conversion into the more biologically active vitamin D3. 17 Renal involvement is common in SLE, which can interfere with 1-hydroxylation that is essential to make 25-OH vitamin D active. 18 SLE photosensitivity and the resultant avoidance of sun exposure also contribute to such deficiency. 19 Moreover, antivitamin D antibodies were observed in an SLE patient's subset and in antiphospholipid syndrome and were particularly associated with anti-dsDNA antibodies. 20
Regardless of the fact that vitamin D deficiency is a cause or consequence or both in SLE, its prevalence has been an addressed issue in many studies. Its presence is almost undeniable though it is expected to differ in prevalence between various populations. Its effect on disease course in terms of activity and severity represents an interesting area of research as it might allow a simple way to ameliorate disease.
We aimed to estimate the prevalence of vitamin D deficiency in SLE Egyptian patients and its relation to various disease parameters.
Materials and Methods
This is a cross-sectional study that included 60 patients with SLE, fulfilling the updated American College of Rheumatology (ACR) criteria. 21 The patients were selected from the inpatients of Internal Medicine, Rheumatology, and Rehabilitation departments and outpatient clinics. A total of 30 age- and sex-matched healthy subjects were also included in this study and served as the control group. All the patients were on steroids and (immunomodulator) drugs. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the Declaration of Helsinki (1964) and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study.
Group I (patients):
This group was further subdivided according to the presence of nephritis into two subgroups:
40 patients without lupus nephritis (LN).
20 patients with LN.
Group II (control):
A total of 30 normal healthy subjects were also included as a control group; they were matched for age and sex with SLE patients.
Patients were clinically assessed through both general and local examinations. Fatigue scale was performed where patients were asked to reflect in a 0–10 visual analog scale (VAS), the degree of fatigue ranging from 0 = no fatigue to 10 = intense fatigue. SLE disease activity index (SLEDAI) was done within the last 10 days. The activity categories are no activity (SLEDAI = 0), mild activity (SLEDAI = 1–5), moderate activity (SLEDAI = 6–10), high activity (SLEDAI = 11–19), and very high activity (SLEDAI20). 22 Also disease-related damage (Systemic Lupus International Collaborating Clinics/American College of Rheumatology Damage Index [SLICC/ACR DI]) was performed, where there are 41 items covering 12 systems. It includes specific comorbidities with SLE, to be scored as damage. 23 In addition, Lupus Severity of Disease Index (Lupus SDI) was calculated to assess 10 items, where each of the first four receives one point and each of the following six items receives two points with possible maximum score being 13. The severity is considered high if ≥ 4. 24
The statistical analysis was performed by IBM SPSS Statistics (V. 19.0, IBM Corp., 2010), which was used for data analysis. Data were expressed as mean ± SD for quantitative measures.
The following tests were performed:
Comparison of two independent mean groups for parametric data using Student's t-test.
Comparison between two independent groups for non-parametric data using Wilcoxon rank-sum test.
Ranked Spearman correlation test to study the possible association between two variables among each group.
Regression analysis.
Results
All patients (100%) had different forms of skin affection. Eighteen patients (30.0%) presented with vasculitis rash in the form of pitting of finger bulbs. Six patients (10.0%) presented with lung affection. Twenty patients (33.3%) had CNS affection in the form of headache, cognitive dysfunction, and peripheral neuritis, another 34 patients (56.7%) had joint affection in the form of arthralgia or arthritis. 20% of patients had serositis in the form of pericardial or pleural effusion. 26.7% of patients had ophthalmic affection in the form of retinal vasculitis or papilledema. Twenty-two patients (36.7%) had renal symptoms in the form of lower limb edema, puffy eyelids, loin pain, and hypertension.
Among 60 patients, 16.7% of patients had leukopenia (<4000/cmm), 56.7% of patients had anemia (<12 g/dL), 13.3% of patients had thrombocytopenia (<150,000/cmm), and 66.7% of patients had CRP > 6 mg/dL, while 90% of patients had ESR > 12 mm/hour. All patients had positive ANA and 90% had anti-dsDNA (>75 IU/mL); 33.3% of patients had C3 < 75 mg/dL, while 36.7% of patients had C4 < 12 mg/dL. Serum creatinine was >1.3 mg/dL in 8 patients (13.3%), and BUN was >20 mg/dL in 16 patients (26.7%).
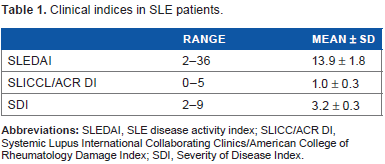
Among 60 patients, according to SLEDAI, there were 6 patients with mild grade (10%), 26 patients with moderate grade (43.3%), 14 patients with high grade (23.3%), and 14 patients with very high grade (23.3%). Other clinical indices are presented in Table 1.
Clinical indices in SLE patients.
All patients were on steroid and hydroxychloroquine. The other drugs received by patients were as follows: azathioprine by 28 patients (46.7%), cyclophosphamide by 14 patients (23.3%), and mycophenolate mofetil by 4 patients (6.7%). No significant correlation was found between any of the drugs and serum vitamin D levels.
Comparison between SLE patients and controls showed a highly significant difference with regard to serum level of 25(OH)D as presented in Table 2, whereas comparison between patients with LN with a mean ± SD of 16.6 ± 7.3 and those without LN 18.5.7 ± 7.1 showed no significant difference (t = 0.696 and P > 0.05).
Comparison between patients and control regarding vitamin D.
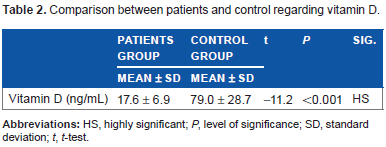
In our study, only two patients (3.3%) had normal levels of vitamin D in serum, 44 had insufficiency (73.3%), and 14 had deficiency (23.3%).
Significant inverse correlations between serum vitamin D and disease activity, severity, and fatigue were found as shown in Figures 1 and 2.
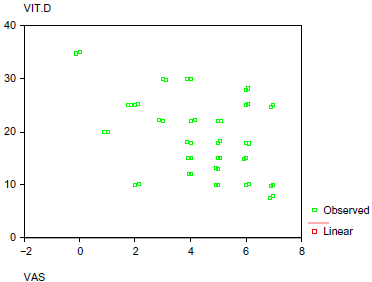
Correlation between vitamin D and VAS.
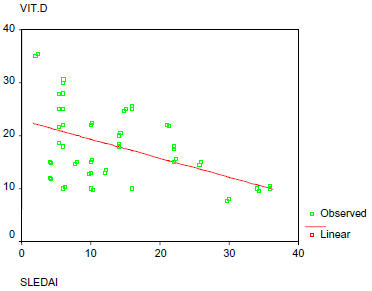
Correlation between vitamin D and SLEDAI.
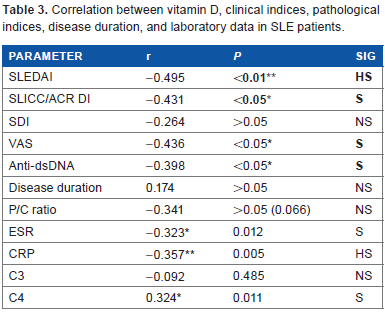
In this study, there was a highly significant positive correlation between vitamin D and fatigue, SLICC (r = 0.502, P < 0.005), and CRP (r = 0.357, P < 0.005). There was a significant positive correlation with ESR (r = 0.323, P < 0.05), C4 (r = 0.324, P < 0.05), SDI (r = 0.419, P < 0.05), and anti-dsDNA (r = 0.413, P < 0.05) and a significant negative correlation with vitamin D level (r = -0.436, P < 0.05), while there was no significant correlation between fatigue with SLEDAI, disease duration, and P/C ratio as presented in Table 3.
Correlation between vitamin D, clinical indices, pathological indices, disease duration, and laboratory data in SLE patients.
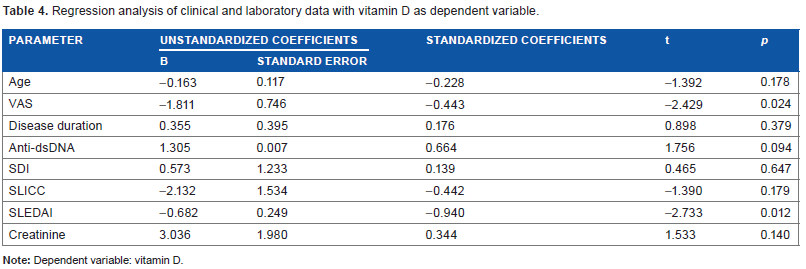
After standardization of all clinical variants, regression analysis study showed a significantly inverse correlation between vitamin D and VAS and a highly significant correlation between vitamin D and SLEDAI score (Table 4).
Regression analysis of clinical and laboratory data with vitamin D as dependent variable.
Discussion
Vitamin D deficiency has been an interesting area to explore in autoimmune disorders since the discovery of its involvement in immune system. SLE patients in particular have a list of multiple risk factors predisposing them to this deficiency. On the other hand, many researchers suggested it as a risk factor itself for developing SLE. Numerous previous studies analyzing its prevalence in SLE patients and its relation with disease activity and severity and finding positive versus negative results made it even more interesting to investigate it in our current study.
In this study, we found a prevalence of vitamin D insufficiency in 73% and deficiency in 23% of our Egyptian patients. Abou-Raya et al. 27 conducted a study on Egyptian SLE patients and found that at baseline the overall prevalence of suboptimal and deficient 25(OH)D serum levels among patients with SLE was 69%. However, Hamza et al. 28 studied Egyptian pediatric SLE patients and found that 60% were insufficient and 13.3% were deficient. Moreover, our results agree with the study by Ruiz-Irastorza et al. 19 , who reported that 75% of SLE patients had vitamin D levels <30 ng/mL and 15% had <10 ng/mL, despite the fact that their population resides in a south European country with plenty of sunny days. The difference between our results might be due to vitamin D supplementation in some patients in the previous study while none in the current study received any at the time of entry. Similarly, Kamen et al. 18 found vitamin D insufficiency and critical deficiency in 67% and 17.8%, respectively, of the SLE patients in their study. These baseline results within a cohort of newly diagnosed SLE patients suggested vitamin D deficiency as a possible risk factor for the development of the disease. Short disease duration in that study decreased the likelihood that vitamin D deficiency could have resulted from the disease and hence suggesting its presence as a cause rather than a consequence. This provided guidance for future investigations looking at a potential role for vitamin D in the prevention and/or treatment of SLE. 19 A remarkable note is that the same ethnic disparities seen in vitamin D deficiency prevalence are also seen in the prevalence of SLE. 29
Since the specific impact of vitamin D deficiency or insufficiency on SLE is more important than just its presence, it was a main scope in our work. Our present cross-sectional study showed important correlations with various studied parameters.
In the current study, an inverse relationship was found between vitamin D level and SLE activity measured by SLEDAI (r = -0.495, P < 0.001). This is in accordance with other cross-sectional studies such as the studies by Borba et al. 30 , reporting a strong negative correlation (P = 0.0005), and Yeap et al. 31 (P = 0.033), both using SLEDAI. The former reported SLEDAI to be associated with low vitamin D levels and high cytokines levels such as IL-6 and TNF and also suggested bone remodeling infection consequent to decreased vitamin D, whereas the latter suggested better BMD response to treatment in patients with higher levels of vitamin D. On the other hand, Ruiz-Irastorza et al. 19 failed to report this relation. Several other studies were concomitant to our finding though measuring activity was slightly different by SLEDAI-2 K like Amital et al. 6 , who concluded that there is an inverse relationship between level of vitamin D and disease activity in SLE and further questioned whether to routinely supplement those patients with vitamin D. 32 This relationship can be explained by the inhibitory effect that vitamin D was found to exert on Th1 immunity and autoantibodies production in basic studies.33,34
An inverse correlation was also found between serum vitamin D level and irreversible organ damage measured by the SLICC/ACR DI (r = -0.431, P < 0.05). Such a relationship could not be verified in two studies that used the same index. In spite no correlation was observed by those researchers, the most recent study of the two highlighted that vitamin D insufficiency is highly prevalent among SLE patients and that sunscreen use and obesity increase the risk. They further stated that clinicians should be aware of these factors and supplement SLE patients at risk for vitamin D deficiency accordingly.19,35
On the other hand, Lupus SDI and vitamin D showed negative correlation but did not reach significance.
Fatigue was found to be prevalent in 97.7% of our studied SLE patients. When measured by VAS, it showed significant negative correlation with vitamin D (r = -0.436, P < 0.05) and significant positive correlations with SLICC, SDI, and antidsDNA antibodies (r = 0.502, P <0.001; r = 0.419, P < 0.05; and r = 0.413, P < 0.05, respectively). In accordance with the current work, Ruiz-Irastorza et al. 19 stated the association between vitamin D deficiency and fatigue in SLE patients and highlighted it as a predictor for higher values of VAS. They further explained that by the fact that vitamin D deficiency is a well-identified cause of myalgia and weakness. 19 Another interesting work in 2010 studied the relationship between changes in 25(OH)D levels from baseline (after supplementation) and changes in fatigue (measured by VAS) and found inverse significant correlations between 25(OH)D levels and the VAS (P = 0.001) at baseline and between changes in 25(OH)D levels and changes in the VAS in patients with baseline vitamin D < 30 ng/mL (P = 0.017); they hence suggested that increasing 25(OH)D levels may have a beneficial effect on fatigue. 36
In the study by Carvalho et al. 20 , antivitamin D antibodies have been observed in a subset of SLE patients and showed a strong association with anti-dsDNA antibodies. We did not study antivitamin D antibodies, but in our study, we found a negative correlation between serum levels of vitamin D and anti-dsDNA (r = -0.398, P < 0.05), which could be explained by the antibodies against vitamin D in SLE demonstrated in the former mentioned study.
Although some studies found a negative relation between vitamin D levels and corticosteroids in terms of dose 28 and cumulative dose, 37 in our study no significant correlation was found between dose and 25(OH)D levels. This is in accordance with the study by Fragoso et al. 38 , who found no correlation between vitamin D level and neither steroid use nor antimalarials in SLE. We also did not find any significant correlation with any of the drugs used by our patients, including antimalarials. On the other hand, the role of HCQ in vitamin D metabolism is relatively complex. Ruiz-Irastorza et al. 19 found that patients on antimalarial treatment had higher levels of 25(OH)D and were less likely to have critically low vitamin D levels; they further explained that it inhibits the 1α-hydroxylation of 25(OH)D, thus decreasing the levels of the most active form of vitamin D. 39
Patients with autoimmune diseases such as multiple sclerosis, RA, and SLE show low 25-OH vitamin D serum levels. Some studies suggested that adequate vitamin D levels diminished the risk for developing various autoimmune diseases.3,40,41 Others proposed “preventive” treatment using vitamin D for high-risk individuals for developing autoimmune diseases. 42 In particular, SLE patients have multiple risk factors for vitamin D deficiency and disease activity and severity might be correlated with lower 25-OH vitamin D serum levels. Treatment of vitamin D deficiency could be particularly important in SLE patients, especially in view of the possible immunomodulatory effects exerted by vitamin D.
The major limitation of this study was the sample size, as well as the duration of the study. Another difficulty was the inability to study the influence of vitamin D supplementation on various clinical manifestations and disease activity.
In conclusion, we found high prevalence of vitamin D deficiency in SLE Egyptian patients. It is associated with higher degree of fatigue and disease activity in those patients. Its effect on disease severity (organ damage) still needs further studies. Also, since the replenishment of adequate level of vitamin D is considered as an easy therapeutic measure (if proven to be both needed and efficient), it may provide a relatively low cost, simple, and safe approach to improve outcome in SLE patients.
So, it is time to routinely give vitamin D supplementation to SLE patients after periodic measurement of its level. Our next step is to subcategorize the patients according to age, sex, and their vitamin D level and to study the effect of vitamin D supplementation on their disease activity and fatigue over a period of time.
Author contributions
Conceived and designed the experiments: NMA, RME-M, AS, RHE-k. Analyzed the data: NMA, RME-M, AS. Wrote the first draft of the manuscript: NMA, RME-M, AS. Contributed to the writing of the manuscript: SAM. Agree with manuscript results and conclusions: NMA, RME-M, AS. Jointly developed the structure and arguments for the paper: KFA-h, AAAZ. Made critical revisions and approved final version: SAM, KFA-h, AAAZ. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgment
A preliminary version of this research was the basis of a poster presentation at the Eular Congress 2015, and the abstract was subsequently published in the Annals of the Rheumatic Diseases.