
Abstract
We present the case of a 67-year-old man with a three month history of right sided facial nerve palsy reporting to our clinic for evaluation of a recently seen suspicious mass in the right lung. Subsequently he was diagnosed with advanced NSCLC right lung and started on palliative chemotherapy. Furthermore, temporal bone metastasis was discovered on radiological imaging while investigating symptoms of acute mastoiditis and persisting facial neuralgia, a symptom completely overlooked at first as Idiopathic Bell's palsy. This presentation is exceptionally unique, although temporal bone metastasis arising from established primary lung or other malignancies is itself rare, and predilect to a later onset in the natural history of the disease, as reported in the literature. None of the published literature report neither addresses the optimal management course nor its subsequent impact on quality of life of patients with temporal bone metastasis.
Introduction
Lung cancer is one of the most common solid tumors to develop bone metastases that occur in 19%–44% of patients during the course of their disease 1 with a significant adverse impact on quality of life and survival. Temporal bone metastasis, however, is a rare phenomenon2–4 that commonly arises from breast (24.8%) and lung (11.3%) cancer. Temporal bone metastasis may be associated with trivial discomfort or even be asymptomatic resulting in an ominous delay in diagnosis. 3 Isolated facial paresis may be a subtle, yet, early sign of such metastasis with few published reports in the indexed medical literature.5–7 Persistent facial palsy, otalgia, bleeding, otorrhoea, deafness, tinnitus, and peri-auricular swelling usually represent overt metastatic disease that occurs late and is associated with dismal prognosis. 3 We report on a case presenting with isolated facial nerve palsy due to temporal bone metastasis eventually resulting in the detection of a lung primary and review the relevant literature.
Case Report
A 67-year-old man, known smoker for over 30 years, first consulted an otolaryngologist at his native place (prior to an appointment with our hospital) with complaints of recent onset right sided earache. A detailed clinical examination at that time was unremarkable. The otalgia was progressive and gradually became associated with ipsilateral facial weakness. An initial MRI brain advised by the same physician did not reveal any positive findings, while a pure-tone audiogram was suggestive of mild senile bilateral sensorineural hearing loss. An electrophysiological evaluation viz. facial nerve motor conduction study showed prolonged latency and reduced amplitude on the right side suggestive of right facial nerve dysfunction, proximal to stylomastoid foramen, and a working diagnosis of right sided idiopathic Bell's palsy and trigeminal neuralgia was entertained. He was prescribed a course of oral steroids, gabapentin, and neural growth factors along with physiotherapy, without much symptomatic relief. After a period of three months from the onset of facial palsy, he subsequently presented to our hospital clinic with mild cough and expectoration. An initial chest X-ray and a Computed tomography (CT) of the thorax, showed a spiculated and irregularly marginated 5.6 × 4.3 cm mass peripherally in the right lower lobe of lung with minimal pleural effusion and large ipsilateral hilar and subcarinal lymphadenopathy (Fig. 1). Fibreoptic brochoscopy revealed an endobronchial lesion at right main bronchus. Bronchoalveolar lavage and post-bronchoscopy sputum cytology were suggestive of poorly differentiated squamous cell carcinoma. Detailed imaging of head and neck and abdomen were unremarkable. He was diagnosed as non-small cell lung carcinoma (NSCLC) of the right lung (cT4N2, stage IIIB). In view of inoperability, he was planned for neoadjuvant systemic chemotherapy. After receiving the first cycle of gemcitabine-carboplatin, he came back with complaints of blood-stained otorrhoea, persisting facial palsy, and post-auricular swelling on the right side. A subsequent CT scan revealed a well defined heterogeneously enhancing destructive lesion measuring 4.1 × 4 × 4.2 cm at the base of right mastoid and involved adjacent basiocciput showed destruction with minimal extra-dural extension (Fig. 2). Fine needle aspiration cytology from the post-auricular swelling suggested poorly differentiated metastatic carcinoma consistent with a lung primary. In view of proven overt metastatic disease and persistent symptoms, he was treated with palliative radiation therapy to the involved temporal bone to a dose of 30 Gy in 10 fractions over two weeks with good symptomatic relief (moderate pain relief and substantial reduction in otorrhoea), although the facial palsy persisited without any significant improvement. He was subsequently started on oral gefitinib and advised to continue further chemotherapy along with supportive treatment.
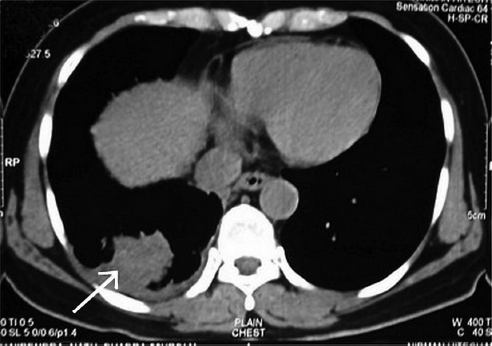
Computed tomography (CT) of the thorax depicts a mass peripherally in the right lower lobe of lung.
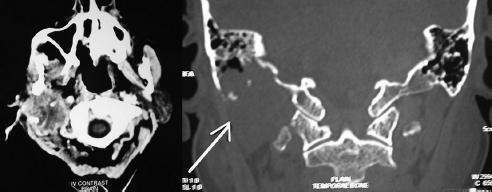
CT scan of the brain showing destructive heterogeneously enhancing lesion involving the right temporal bone with extension to the adjacent basiocciput.
Discussion
Bone metastases occur in 19%–44% of patients with lung cancer during the course of their disease, 1 with significant adverse impact on quality of life and survival. Early temporal bone metastasis may be relatively asymptomatic or associated with trivial discomfort. 3 It may present with subtle facial nerve paresis which can progress to persistent facial palsy. Peri-auricular swelling, hearing loss, tinnitus, dizziness, otalgia, otorrhoea, bleeding, mass in ear, and nystagmus are often signs of overt metastatic disease and are associated with a dismal outcome. The triad of otalgia, peri-auricular swelling, and facial palsy is seen in up to 50% of patients with temporal bone metastases. Petrous apex remains the commonest site of involvement followed by tegmen tympani, mastoid bone, and internal auditory canal3,4 in metastatic temporal bone lesions.
Idiopathic facial paralysis (Bell's palsy) is a clinical diagnosis that accounts for over 50% of all facial nerve palsies where no adjunct radiological investigations are indicated. Persistent, prolonged (over 4 months) or progressive facial palsy and emergence of other neuro-otologic symptoms warrant appropriate imaging to arrive at a definitive diagnosis. 8 High-resolution CT scan is generally the initial investigation of choice with a complimentary MRI if indicated. 8 The imaging findings in lesions involving the temporal bone are however generally non-specific, 9 with early lesions especially at the petrous apex at risk of being missed on a routine CT scan particularly in absence of bone destruction. In retrospect, persistent neuro-otologic symptoms seen in our patient must have been causally related to temporal bone metastases. However, in absence of an antecedent history of systemic cancer, it was misdiagnosed as idiopathic Bell's palsy resulting in a delayed diagnosis of the lung primary. It may be possible that the initial MRI failed to detect a very small lesion in the petrous apex which later on progressed to cause significant bone destruction and manifested as a post-auricular mass.
The overall prognosis of patients with metastatic tumors of the temporal bone is quite dismal, irrespective of treatment modality.3,9 It generally entails a multidisciplinary approach that addresses radiotherapy, surgery, chemotherapy, and medical therapy with analgesics and bisphosphonates. The choice of modality is largely dependent on factors like status of primary disease, performance status of patient, other sites of involvement, and available resources. In case of a solitary metachronous metastasis detected on surveillance imaging with controlled primary, metastasectomy followed by post-operative radiation therapy offers the best outcome. 10 External beam radiation therapy either alone or in combination with systemic chemotherapy offers good palliation resulting in improved quality of life, as was evident in this patient who achieved good symptomatic relief.
Disclosures
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.