
Abstract
There are some inevitable risk factors of patient exposure to problems arising from human errors, including missed subtle radiological findings, early identification of which may alter the patient outcomes. Here we are discussing a patient who presented with a prior diagnosis of seasonal allergic rhinitis with symptoms assumed to be bronchial asthma. A second review of chest radiograph after discussion over an online platform (Tabula Rasa group on Facebook) revealed some subtle findings which we missed initially. Further workup of the case revealed some astonishing findings. This case illustrates the importance of discussing unsolved cases on online platforms with peers and also to proceed for higher imaging to detect what has been missed on plain radiography.
A 60-year-old man with a prior diagnosis of seasonal allergic rhinitis along with symptoms assumed to be bronchial asthma since the last 25 years presented with cough, fever, and breath-lessness for five days. There was no history of orthopnea, loss of appetite, and loss of weight. Physical examinations were normal except diffuse rhonchi present all over the chest. Skiagram chest posteroanterior (PA) view done by computed radiography (CR) system showed no abnormality that was obvious to the authors at the first instance (Fig. 1). All blood investigations were within normal limits except increased leukocyte counts (15,000/mm3) with predominant neutrophils. The patient was put on symptomatic treatment but got no relief, and his chest findings were persistent. There was something in his chest X-ray that bothered us, and we decided to radiologically work him up further.

Apparently normal chest skiagram–-PA view.
Further workup using contrast-enhanced computed tomography (CECT) (by Siemens SOMATOM Sensation 40 machine) of the thorax with high-resolution sections revealed collapse consolidation of the right middle lobe with some cystic changes in the right lower lobe and ground glass haziness in both lower lobe posterior segments (left side >> right side), suggestive of infective pathology (Fig. 2). There was a gross disparity between our initial clinical and radiological impression where the chest X-ray was apparently thought to be normal with some lingering doubt and a gross pathology was found on CECT. The patient responded well to culture and drug sensitivity-guided antibiotic and supportive therapy. Here, we address the importance of radiological disparity in the first encounter with chest X-ray (CXR) and review again the post-CECT interpretation (including high resolution [HR] sections).
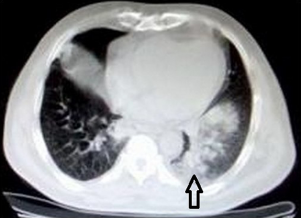
CECT of the thorax with high-resolution sections showing collapse consolidation of the right middle lobe (arrow) with some cystic changes in the right lower lobe and ground glass haziness in both the lower lobe posterior segments (left side >> right side), suggestive of infective pathology.
Discussion
Radiological interpretation is not an exact science. It involves the decision making guided by the clinical data provided, and a certain degree of error is inevitable and is well recognized. 1 A study by experienced radiologists found an overall 23% error rate when no clinical information was supplied, falling to 20% when clinical details were available, while reporting a collection of normal and abnormal X-rays. 2 Early identification of diagnostic errors is important because of their connection to the outcomes and the wide variability observed with modalities. 3 In a busy outpatient department, subtle findings can be missed while interpreting a radiograph in a few seconds as in our case. 4 After this evaluation, a lateral chest X-ray (Fig. 3) was done, and the findings in the lateral radiograph as well as revisiting the PA radiograph pointed toward two signs that were actually pointed out by other members of our online network tabula-rasa (http://www.facebook.com/groups/tabularasa/permalink/915103451850535.) where we discussed this case.

Chest skiagram (lateral view) showing a hyperdense opacity in the left lower zone superimposed on thoracic vertebra just behind the heart along with a gradual increased lucency down the thoracic vertebral bodies and less soft tissue attenuation in the lower chest wall as compared to the upper chest wall/shoulders.
The first sign on the lateral radiograph that was pointed out was the thoracic spine sign–-an interruption in the progressive increase in lucency of the vertebral bodies from superior to inferior.
A finding in a plain lateral chest film consisting of a paradoxical increase in radiologic opacity over the lower spine/vertebra suggests the presence of lower lobe pneumonia. The sign is generally regarded as helpful when evaluating the left lower lobe for pathology, as it may be obscured by the heart on PA chest films. 5 During ultrasonography of chest, the thoracic spine sign is visualized when anechoic or hypoechoic fluid is present in the pleural space. Fluid serves as a medium through which the thoracic vertebral bodies are visualized above the diaphragm. 6 Ely et al have further elaborated on the formation of spine sign:
Increased lucency as progress down thoracic vertebral bodies.
Less soft tissue attenuation in lower chest wall as compared to upper chest wall/shoulders.” 7
Prompted by one of the members in our online discussion forum, we took another relook at the initial chest X-ray PA view where we had wondered what was it that had bothered us about it, and we realized that in PA view, the left hemidiaphragm was also silhouetted with no clearly visible margins of the diaphragm outlines that itself could have suggested a retrocardiac consolidation.
In all specialties of medicine, there are some unavoidable factors of patient exposure to problems arising from human error. 4 For radiological investigations, the use of the term error is often inappropriate; it is more appropriate to describe it as discrepancies between a report and a retrospective review of a film or an outcome. 8 Discrepancy is described as a difference in opinion between the original interpretation and the interpretation at review, representing a significant difference in diagnosis/relevant findings, which may affect the patient outcome. Previous studies have identified potential causes of reporting discrepancy, including inadequate, misleading, or incorrect clinical data provided; excessive workload with poor working conditions; interobserver variation; and ambiguity of the wording or summary of the report. 9
The level of error varies from 2 to 20% for clinically significant or major error depending on the radiological investigation used. 10 The majorities of discrepancies are due to false-negative interpretation and occur primarily in the plain film as in our case.
Plain chest radiography is the most commonly used imaging tool that can rapidly demonstrate the presence of pulmonary abnormalities in respiratory symptomatics because of its wide availability and an excellent cost-benefit ratio. 11 However, it has low sensitivity for the detection of early infection, being normal in up to 10% of patients with proven pulmonary disease.12,13 Conventional CXR has a low diagnostic yield in early detection and monitoring of early infectious process, but the high-resolution computed tomography (HRCT) scan of the thorax can reveal lesions that were undetected on a standard CXR. 14 Also, not only radiographs can under diagnose, they can also over diagnose, particularly the interstitial processes. This may be due to a host of issues, including technical factors, obesity, smoking, and emphysema. Usually computed tomography (CT) is not recommended for the initial evaluation of patients with suspected pulmonary infection, and it is much more sensitive and specific than chest radiographs for detecting subtle pulmonary abnormalities and may prove a valuable adjunct to chest radiography in patients with nonrevealing or nondiagnostic imaging findings as in our patient.15,16 CT is significantly superior to CXR in the evaluation of infectious pulmonary disease. Therefore, an unremarkable CXR can be followed by a CT scan to reliably detect or to accurately exclude early pulmonary infection. 17 Similarly, Maughan et al also advocate HRCT as the further modality of choice to evaluate symptomatic patients with an otherwise normal chest radiograph. 18 The HRCT has the greatest value in excluding lung pathology when the radiographic findings are equivocal and in confirming the presence of clinically suspected disease even when the radiograph is normal, especially in the cases of suspected interstitial lung disease. 19
Learning Points
Errors are inevitable in clinical science in the form of missing subtle imaging finding on chest radiography; sometimes, second review may help, and even then, undiagnosed cases with persistent clinical and laboratory finding in favor of lung pathology can undergo higher imaging in the form of HRCT thorax.
The lateral chest radiograph provides a perspective that may significantly enhance the evaluation for thoracic disease. An awareness of routinely visualized anatomic structures and spaces should facilitate improved interpretation of conventional chest radiographs.
The silhouette sign with the absence of normal diaphragmatic outline on the left base can indicate a left lower lobe consolidation and can be missed if one has never had the occasion to see it before. The thoracic spine sign was noted in our patient in retrospect.
Online learning forums can serve to add collective learning inputs to individual physician, learning experiences around their patients.
Footnotes
Acknowledgment
We would like to acknowledge all the staff involved in the care of the patient.
Author Contributions
Conceived and designed the experiments: RPT, RK, MLB, RB. Analyzed the data: RPT, RK, MPS, KG. Wrote the first draft of the manuscript: RPT, MLB, RB. Contributed to the writing of the manuscript: RPT, RK, MLB, MPS, KG, RB. Agree with manuscript results and conclusions: RPT, RK, MLB, MPS, KG, RB. Jointly developed the structure and arguments for the paper: RPT, MLB, RB. Made critical revisions and approved final version: RPT, RK, MLB, MPS, KG, RB. All authors reviewed and approved of the final manuscript.