
Abstract
This case report describes the presentation of new onset of worsening bilateral proximal and distal upper and lower limb weaknesses for the past three months in a 48-year-old man. His past medical history includes only essential hypertension. He denied any fever, diarrhea, or recent vaccination prior to the onset of his symptoms. He had vague patchy sensory loss in both right upper and lower limbs with no clear dermatomal distribution. The magnetic resonance imaging (MRI) of the cervical spine revealed features consistent of partial transverse myelitis. Cerebrospinal fluid (CSF) analysis showed raised opening pressure with evidence of yeast cells on gram stain examination on three different occasions. His neurological symptoms and signs responded to a two-week course of intravenous amphotericin B and oral flucytosine, but there remained minimal residual neurological deficit.
Introduction
Acute partial transverse myelitis is an incomplete or patchy involvement of at least one spinal segment with mild-to-moderate weakness, asymmetry, or dissociated sensory symptoms. It may also be defined as asymmetrical or mild loss of spinal function. 1 It is an acute disorder that presents a wide array of clinical presentation and has multiple causes. An attack of acute partial transverse myelitis may be the beginning of multiple sclerosis (MS). The clinical features, diagnostic investigations, and treatment modalities differ between the different underlying etiologies of partial transverse myelitis. Therefore, elucidating the exact cause of this disorder is important as it may affect its prognosis.
Case Presentation
A 48-year-old gentleman presented with worsening weakness of his bilateral proximal and distal upper and lower limbs for the past three months. The progression of the weakness over the three months was gradually worsening. The muscle weakness began with the proximal and distal lower limbs simultaneously and moved to the bilateral proximal and distal upper limbs. There was no clear trend of ascending or descending weakness in a particular limb.
This was the first such presentation for him. He had never sought medical treatment for these symptoms before. The weakness was associated with patchy numbness of both upper and lower limbs. He did not complain of any wasting of his limbs. He had on and off headache, which he described as generalized throbbing pain in character that occasionally woke him up from sleep in the mornings. It was not associated with vomiting. He complained of on and off constipation. He denied any bladder or bowel incontinence. He also complained of easy fatigue and reduced effort tolerance for the past three months. No palpitations occurred. Initially, he was able to ambulate but decided to seek hospital treatment when he progressively became wheelchair bound. He denied any back pain. He had no history of respiratory or gastrointestinal symptoms. He denied any recent fever or vaccination. He had not travelled recently. He denied any bulbar or pseudobulbar symptoms. He did not complain of any neck pain/stiffness, truncal rigidity, or diplopia. He denied any history of sexual promiscuity or intravenous drug usage. There was no recent usage of steroids.
His only significant past medical history was essential hypertension, which was treated with 5 mg of oral amlodipine daily. He had a history of fall at his workplace because of slippery floor a year ago, where he fell backward but was able to ambulate immediately afterward.
He worked previously with the Royal Malaysian Army until his compulsory retirement. Currently, he works as a van chauffeur. He is a nonsmoker and a teetotaler. This patient has a family history of hypertension and ischemic heart disease.
Clinically, on examination, he had obvious weakness of his upper and lower limbs. The power of the bilateral upper limb muscles (shoulder abduction and adduction, elbow flexion and extension, wrist flexion and extension, finger flexion and extension, and finger abduction and adduction) was 3/5. The power of the bilateral lower limbs (hip adduction, hip abduction, knee extension and flexion, and ankle dorsiflexion and plantarflexion) was 3/5. The tone of all four limbs was normal with brisk reflexes and clonus of the right upper limb (biceps, triceps, and supinator jerks) and lower limb (knee and ankle jerks). There was no obvious muscle wasting or fasciculations. The reflexes were normal on the left upper and lower limbs. Extensor plantar was upgoing on the right. There was patchy sensory loss of the right upper and lower limbs with no clear sensory level. His proprioception and vibration sense were absent in the right upper and lower limbs but preserved in the left upper and lower limbs. No cerebellar signs were seen. Fundoscopy revealed no abnormalities. All 12 pairs of cranial nerves were intact.
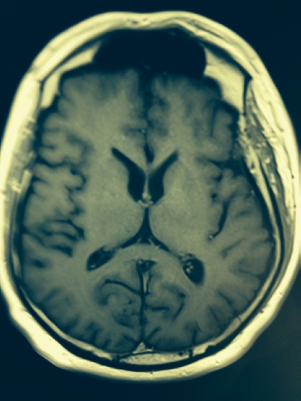
MRI of the brain. Lacunar infarction at the left frontal lobe is adjacent to inferolateral aspect of the frontal horn of the left lateral ventricle. There are slightly prominent ventricles, and rest of the CSF could suggest early cerebral volume loss. No obvious demyelinating plaques or cerebral edema is seen. There is no focal enhancing mass lesion in the brain parenchyma. Gray white matter differentiation appears to be preserved.
His blood pressure was 114/80 with a pulse rate of 88 bpm–-regularly regular. He was afebrile with a bedside dextrostix of 8.3 mmol/L.
The cardiovascular system revealed normal heart sounds with no murmurs. The lungs and abdomen were unremarkable on physical examination.
An urgent T2-weighted magnetic resonance imaging (MRI) of the brain and cervical spine was done, which revealed features consistent with C4/C5 partial transverse myelitis and a left frontal lacunar infarct. The MRI of the thorax, lumbar, and sacrum was done a month later, which did not reveal any significant findings except for mild posterior bulges from L3/L4 to L5/S1.
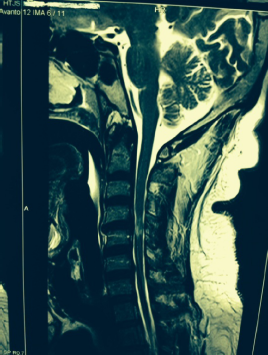
T2-weighted MRI of the cervical spine.
Lumbar puncture was performed, which revealed persistent presence of yeast cells on the cerebrospinal fluid (CSF) gram stain on three different occasions. The CSF protein level was elevated at 0.98 g/L (normal value: 0.1–0.45 g/L). His CSF glucose level was normal. CSF for acid fast bacilli direct smear and culture/sensitivity were negative. Testing for Lyme antigen was not performed as this test was not widely available. The cryptococcal antigen and India ink were negative. There were no oligoclonal bands seen. The opening pressure was elevated at 41 cm H2O.
The blood bacterial and fungal cultures failed to grow any organism. His Venereal Disease Research Laboratory test (VDRL)/Treponema Pallidum Haemagglutination Assay test (TPHA), anti-HIV1,2 serology, and rapid test were all nonreactive.
His full blood count revealed normal hemoglobin of 12.2 g/dL. The total white cell count was 10 × 109/L with normal platelet count. The renal profile and liver function test parameters were within the normal range. His fasting and random blood glucose were 5.9 and 7.5 mmol/L, respectively.
There was no nerve conduction studies done.
Full ophthalmological examination, which was carried out by the ophthalmologist, showed normal fundus bilaterally.

CEMR of the cervical spine. Same as notes in Figure 2.
In view of the presence of CSF yeast cells and MRI findings, he was treated for fungal partial cervical transverse myelitis. He was given intravenous amphotericin B 0.7/mg/kg/day and oral flucytosine 100/mg/kg/day for a duration of two weeks. The lumbar puncture was repeated every other day until there were three negative gram stain CSF samples. The opening pressure was normal, subsequently falling in between 10–20 cm H2O. He also underwent intensive limb physiotherapy.
His upper and lower limb weaknesses improved significantly with power 4+/5, albeit not to totally normal power. He was then reviewed at the neurology clinic for follow-up care.
Discussion
Fungal partial transverse myelitis of the cervical spine is rare in an immunocompetent individual without any significant risk factors. It should be considered as one of the probable differential diagnoses in a patient who presents with both upper and lower limb weaknesses with asymmetrical upper motor neuron involvement. Acute complete transverse myelitis may be defined as an idiopathic inflammatory disorder causing symmetrical spinal cord dysfunction below a specific level of cord function. 2 The ensuing disability may be moderate to severe, and there is often a clear sensory level. However, partial transverse myelitis is a term used in which only one side of the cross-section of the spinal cord is inflamed. Complete or partial transverse myelitis can appear for several reasons. Sometimes, the disorders classified as such can be referred to as transverse myelitis spectrum disorders. 3 Commonly, the exact cause of partial transverse myelitis may be unknown, leading to the term idiopathic partial transverse myelitis.
However, in this patient, his CSF showed yeast cells on three different occasions, which clearly revealed to the infective cause of his partial transverse myelitis.
Differential diagnoses for partial transverse myelitis include neuroinflammation; infectives such as tuberculosis, syphilis, cytomegalovirus, and schistosomiasis; and some vaccinations, including those for varicella zoster and polio. Other probable differentials include vascular causes, structural causes, neoplasm, a slow growing intraspinal tumor, and arachnoiditis (eg, following meningitis or intrathecal administration of medication). The latter may need to be considered in the context of a fungal arachnoiditis.
Acute myelitis accounts for 4–5% of all cases of neuroborreliosis. 4 Vascular insults usually present within hours to days, and demyelinating/inflammatory presentations evolve over days or weeks, while in this case, the evolution was over months.
In infectious cases of acute partial transverse myelitis such as in this case, the immune-mediated inflammation could have been as a result of exposure to the fungal antigen.
Fungal infection in an immunocompetent patient requires further immunological workup, such as immunoglobulins, specific antibodies to vaccination, and T-cell function. The CSF IgG index and immunoelectrophoresis would be helpful.
The treatment of this patient was based on an empirical basis and not on culture and sensitivity of the CSF. Therefore, such a diagnosis of a rare fungal cause was better achieved through culture, sensitivity, and PCR if available. Gram stain is acceptable as a primary step for diagnosis of fungal infection, but such a case needs further steps to reach a precise diagnosis of the cause of the infection. In addition, knowing the sensitivity of this agent to antifungal treatment is mandatory, as there is the possibility of resistance. A search for the source of infection in such an immunocompetent patient is recommended.
In some individuals, partial transverse myelitis might represent the initial symptom of a demyelinating disease of the central nervous system such as MS, acute disseminated encephalomyelitis (ADEM), or neuromyelitis optica (NMO) or Devic's syndrome. In one of the earlier studies on acute partial transverse myelitis, it is clearly shown that in a majority of patients presenting with asymmetric and patchy spinal cord dysfunction, the disease converted to clinically definite MS (CDMS) within three years. 2 From the literature there is a suggestion that partial transverse myelitis is more likely related to demyelination with a high chance of evolving into MS compared to complete transverse myelitis. In this case, there was clearly a different cause for the presentation.
A total of 13 out of 15 patients (87%) in whom the conversion had taken place had abnormal brain MRI at the onset of the disease. 2 When the initial brain MRI was normal, over a five-year follow-up period, in approximately 20–30% of patients, it had converted to definite MS. 2
This patient also had a lacunar infarct. This is probably unrelated to the clinical presentation with partial transverse myelitis.
A careful examination of medical history and a complete neurological examination may help to differentiate between a patient with idiopathic partial transverse myelitis and one who has an underlying condition. 5 MRI with gadolinium contrast is the preferred imaging modality, but to help rule out other structural causes of symptoms (such as abscesses, hematoma, or acutely herniated disk), CT myelography is a reasonable alternative although it does not visualize the whole spinal cord. 3 It is of critical importance not to miss a compressive myelopathy as this ought to be treated by emergent surgical decompression. 6 Recovery from partial transverse myelitis usually begins within two weeks to three months of the onset of symptoms and may even continue for up to a few years. However, if there is no improvement within the first few months, complete recovery is unlikely. Appropriate initial treatment aimed at treating the underlying cause combined with physical therapy has been shown to improve outcomes.
Conclusion
In conclusion, partial transverse myelitis should be considered as a probable differential diagnosis for sudden onset of bilateral upper and lower limb weaknesses. It is a clinical syndrome associated with multiple etiologies. Complete history taking, thorough neurological physical examination, appropriate imaging, CSF studies, and serological analysis may determine the etiology of this clinical syndrome, which provides targeted treatment resulting in better outcomes for patients.
Informed Consent
Informed consent was obtained from the patient for the publication of the study.
Footnotes
Author Contributions
Conceived and designed the experiments: GK. Analyzed the data: GK. Wrote the first draft of the manuscript: GK. Contributed to the writing of the manuscript: GK. Agree with manuscript results and conclusions: GK. Jointly developed the structure and arguments for the paper: GK. Made critical revisions and approved final version: GK. Author reviewed and approved of the final manuscript.