
Abstract
A 45-year-old man with a history of untreated diabetes mellitus had a persisting fever, back pain, and diarrhea. The primary care physician diagnosed the patient with the flu and gastroenteritis. The patient developed paraplegia for two weeks and was admitted to another hospital. The physician in this hospital suspected infectious meningitis and myelitis, and administered piperacillin and steroids without cerebrospinal fluid (CSF) examination. On referral to our hospital, he presented a high fever and complete paraplegia. The lumbar puncture revealed a yellowish CSF, polynucleosis, and hypoglycorrhachia. Bacteria were not detected on Gram's staining and were not confirmed by CSF culture. Magnetic resonance imaging (MRI) showed no thoracolumbar lesion and suggested a cervical epidural abscess without any spinal cord compression. He was diagnosed as having osteomyelitis with meningitis and thoracic myelitis. The infection subsided with broadspectrum antibiotics. After two weeks, bilateral sensorimotor disturbances of the upper extremities appeared. MRI findings showed the epidural abscess compressing the cervical spinal cord. We performed debridement of the epidural abscess. The infection was clinically controlled by using another antibiotic. One month after the infection subsided, a 360° reconstruction was performed. In this case, the misdiagnosis and the absence of CSF examination and culture to detect the pathogenic bacteria at an earlier stage in the patient's disease course might have led to the exacerbation of the pathology.
Introduction
Osteomyelitis of the cervical spine accounts for approximately 3–6% of vertebral osteomyelitis cases.1,2 Osteomyelitis typically results from the hematogenous spread of microbial organisms. Progression of osteomyelitis may result in an epidural abscess, subdural abscess, and paraspinal abscess. 3 Moreover, osteomyelitis results in destruction of the vertebral body and intervertebral disc, and leads to spinal deformity, instability, and neurological deficits. 4 The primary risk factor of osteomyelitis is diabetes mellitus. 5
The common neurological complication of osteomyelitis is cord compression secondary to an epidural abscess. Moreover, meningitis and myelitis are complications of osteomyelitis. However, it is difficult to diagnose osteomyelitis in cases where meningitis is present. We describe a case of cervical osteomyelitis and epidural abscess that exacerbated after conservative therapy of thoracic myelitis and meningitis in a diabetic patient. In the present case, the cervical osteomyelitis and discitis insidiously spread to an epidural abscess and progressed to meningitis from the cervical dura mater. This case also demonstrates that the misdiagnosis by the primary care physician and the absence of cerebrospinal fluid (CSF) examination and culture by the secondary physician to detect the pathogenic bacteria at an earlier stage in the patient's disease course might have led to the exacerbation of the pathology. This study was approved by the Ethics Committee of the Osaka University Medical School in Osaka, Japan.
Case Report
History and examination
A 45-year-old man with a history of diabetes mellitus had a persisting fever, back pain, and diarrhea. His medical history included an open fracture of his left lower leg caused by a traffic accident nine years ago. His primary care physician diagnosed the patient with the flu and gastroenteritis and prescribed an oral analgesic. He still presented back pain and subsequently presented bilateral leg motor weakness and sensory disturbance. He developed paraplegia for two weeks and was admitted to another hospital. With regard to consciousness, he did not seem disoriented. The physician in this hospital examined the patient's blood, but not the CSF. The leukocyte count and C-reactive protein level were 28,300 cells/μL and 39 mg/dL, respectively. Thoracolumbar computed tomography displayed no cord compression or lesions. The physician suspected the presence of infectious meningitis and myelitis, and administered piperacillin and steroids.
On referral to our hospital, he presented a high fever (39 °C), stiff neck, complete paraplegia, and no sensation below T5, and was disoriented (Glasgow Coma Scale, E4V4M6). His laboratory tests suggested lack of adherence to antidiabetic medication (HbA1c, 12.0%; blood C-peptide, 0.4 ng/mL; urine C-peptide, 15 ng/mL). The leukocyte count and C-reactive protein level were 32,000 cells/μL and 40 mg/dL, respectively. The lumbar puncture revealed a yellowish and cloudy CSF, polynucleosis, and hypoglycorrhachia. A magnetic resonance imaging (MRI) scan did not indicate any thoracolumbar lesion (Fig. 1C) and suggested an epidural abscess at C5–6 (Fig. 1A and B). MRI also showed a right intradural mass spreading to the epidural space at C6–7 (Fig. 3). He was diagnosed as having osteomyelitis with meningitis and thoracic myelitis. We could not perform fluorodeoxy-D-glucose positron emission tomography. We noted that the epidural lesion did not cause cord compression. Furthermore, he had no bilateral upper motor weakness or sensory disturbance. Bacteria were not detected on Gram's staining and were not confirmed by CSF culture. Therefore, we treated this patient conservatively without the biopsy of cervical lesions to detect the pathogenic bacteria.
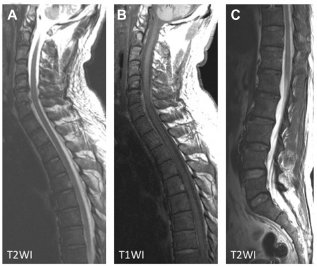
Cervicothoracic spinal MRI on admission indicated an epidural abscess with iso–high intensity on T1Wl (
The patient was initially treated with meropenem and vancomycin to broadly resolve the Staphylococcus aureus infection, and insulin was intravenously administered. He was also administered micafungin for five days. On day 3 in our hospital, MRI findings revealed a decrease in epidural fluid collection (Fig. 2A-C). On day 6, the CSF examination findings had improved, but C-reactive protein levels persisted at 5–6 mg/dL. We could not detect the pathogenic bacteria in arterial and venous blood, urine, and CSF. His neurological symptoms partially improved, but paraplegia was still noted.

Cervicothoracic MRI on day 3 and 18 showed an epidural abscess with iso-intensity on T1WI (
On day 18, he complained of neck pain and presented with fever again (39.5 °C). Moreover, bilateral sensorimotor disturbances of the upper extremities appeared. An MRI scan showed that the epidural fluid compressed the spinal cord at C4–7 (Fig. 2D–F). The right intradural mass was still present at C6–7 (Fig. 3). In addition, the cervical osteomyelitis and discitis at C5–6 and dorsal epidural abscess at C4–7 were exacerbated.

Cervical MRI at day 1, 3, and 18 on T1WI and T2WI at C6–7. The right intradural mass exhibiting low intensity on T1WI and T2WI is shown (yellow arrow).
Surgery
On day 18, we performed C4–7 laminectomy and debridement of the epidural abscess. The surface of the C6–7 dura mater was yellowish in color, indicating the infectious changes (Fig. 4). However, we could not detect the pathogenic bacteria in surgical samples. We changed the antibiotic therapy and achieved clinical control of the infection by using garenoxacin and cephalosporin, as confirmed by the presence of a normal leukocyte count and C-reactive protein level. In addition, his symptoms in the upper extremities were improved. Hence, treatment with garenoxacin and cephalosporin was stopped on day 60 and day 32, respectively. His blood sugar level was controlled by the subcutaneous injection of insulin. The patient received rehabilitation therapy at another institution for two months. He used a Philadelphia collar up to three months after the second surgery.

Intraoperative view. The left side in the picture represents the rostral side. The upper side in the picture is the right side. The right dorsal dura mater at C6–7 has a yellowish surface.
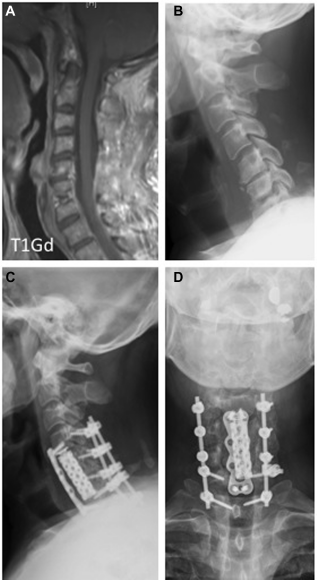
One month after the infection subsided, a second surgery was performed. A cervical roentgenogram revealed the destructive changes in the C5–6 vertebral body and a kyphotic alignment (Fig. 5B). Intraoperative and MRI findings revealed destruction of the anterior and posterior columns of spinal support elements (Fig. 5A). Thus, we performed debridement of all necrotic bone and soft tissues, anterior stabilization of C4–7, and posterior reconstruction and stabilization of C4–T1 (Fig. 5C and D). An expandable cage was implanted in the C4–7 intervertebral space (ADD plus, Ulrich Medical). Expandable cages were used because of the presence of rigid posterior stabilization, which impeded anterior distraction that was necessary to implant the rigid cages. Posterior lateral mass screws (C4–6) and pedicle screws (C7–T1) were implanted.
Postoperative cervicothoracic MRI. (
Postoperative course
Oral antibiotic therapy was continued for three months post surgery. The patient was followed up for one year, and there was no recurrence of osteomyelitis and the abscess. He had paraplegia and required the use of a wheelchair. There were no major or minor complications. The postoperative cervical roentgenogram revealed an almost normal lordotic alignment and no shifting of the instrumentation.
Discussion
The presentation of osteomyelitis may be insidious.1,6 Therefore, the diagnosis of osteomyelitis is often delayed because it is often disguised by other infectious symptoms. Our diabetic patient developed cervical osteomyelitis and an epidural abscess after conservative therapy for thoracic myelitis and meningitis. MRI findings revealed a right intradural mass at C6–7. Intraoperative findings showed infectious changes in the C6–7 dura mater. In this case, the primary care physician misdiagnosed the disease, and the physician in the referral hospital did not perform CSF examination and culture. Moreover, we could not detect the pathogenic bacteria at an early stage in the patient's disease course. These factors led to the misdiagnosis and distracted from appropriate antimicrobial use.
The most common pathogen of spinal osteomyelitis is S. aureus, which accounts for 40–80% of all spinal osteomyelitis cases. 7 Inadequate antibiotic treatments before surgery or biopsy result in the inability to cure the infection. In the present case, we could not identify the pathogen because of the partial therapy with tazobactam/piperacillin that was administered for a few days in the referral hospital.
The use of instrumentation for internal fixation raises concerns of secondary infection and remains controversial.8–10 Thus, we decided to perform a two-stage procedure.11–14 First, we performed debridement and laminectomy, and thereafter, we performed anterior and posterior reconstruction and stabilization. During the second surgery, after posterior reconstruction and stabilization, anterior stabilization with an expandable cage was performed. Delayed secondary infection after instrumentation has been reported in cases at more than one year post surgery. 15 Hence, long-term antibiotic therapy after instrumentation for cervical osteomyelitis is recommended.15,16 Therefore, we administered oral antibiotics for three months post surgery in the present case.
MRI is a sensitive and specific imaging study in the assessment of osteomyelitis, discitis, and epidural abscess.17–19 Enhancement with gadolinium diethylene triamine pen-taacetic acid is useful in the evaluation of disk space infections, osteomyelitis, and epidural abscess. 20 However, early diagnosis of osteomyelitis is often difficult with MRI. Bone scintigraphy is effective for the early diagnosis of osteomyelitis.21,22 In the present case, cervical MRI revealed an epidural abscess with iso–high intensity on T1WI and low intensity on T2WI. During the antibiotic therapy withdrawal period, the iso-intensity of the epidural abscess on T1WI had changed. During the exacerbation period, the epidural abscess was detected by iso-intensity on T1WI. Moreover, the C5–6 vertebral body presented iso-intensity on T1WI and high intensity on T2WI and T1Gd. Hence, the early diagnosis of osteomyelitis requires the presence of clinical signs.
Conclusion
In the present report, we describe the manner in which cervical osteomyelitis and discitis insidiously spread, leading to the development of an epidural abscess, which then progressed to meningitis from the cervical dura mater. The case also indicates that severe cervical osteomyelitis in a diabetic patient could be cured with staged anterior and posterior instrumentation surgery. However, in the present case, the primary care physician misdiagnosed the disease and the physician in the referral hospital did not perform CSF examination and culture. Moreover, we could not detect the pathogenic bacteria at an earlier stage in the patient's disease course. These factors led to the misdiagnosis of the condition and hindered appropriate antimicrobial use.
Author Contributions
Conceived and designed the experiments: YO, KI, TY. Analyzed the data: YO, KI, TY. Wrote the first draft of the manuscript: YO. Contributed to the writing of the manuscript: YO, KI, SI, TY. Agree with manuscript results and conclusions: YO, KI, SI, TY. Jointly developed the structure and arguments for the paper: YO, KI, SI, TY. Made critical revisions and approved final version: YO, KI, SI, TY. All authors reviewed and approved of the final manuscript.