
Abstract
Background
Intensive care has become very important in the management of critically ill children who require advanced airway, respiratory, and hemodynamic supports and are usually admitted into the pediatric intensive care unit (PICU) with the aim of achieving an outcome better than if the patients were admitted into other parts of the hospital. It becomes important to audit admissions and their outcome, which may help to modify practices if necessary following thorough introspection, leading to better patient outcomes.
Objective
To evaluate the morbidity pattern and outcome of admissions into the PICU of a tertiary care center in India.
Methods
A retrospective study in which records of admissions (from August 2012 to June 2013) were obtained from the PICU records. Information retrieved included age, sex, diagnosis, duration of stay in the unit, and outcome.
Results
Mean age of the studied 341 patients was 40.01 ± 45.79 months; 50.7% were infants and 59.8% were males. The three most common disease categories admitted were cardiovascular disease (41.1%), neurological disorders (12.0%), and respiratory disease (10.0%). The mean duration of stay in PICU was 3.2 ± 4.5 days. The overall mortality rate was 2.1%.
Conclusion
Mortality is low in our PICU. We conclude that a well-equipped intensive care unit with modern and innovative intensive care greatly facilitates the care of critically ill patients giving desirable outcome. An expansion of the pediatric wards is advocated to enhance cost–-effective management of patients and avoid unnecessary stretch of the PICU facilities.
Introduction
Intensive care has become very important in the management of critically ill children. The pediatric intensive care unit (PICU) is a part of the hospital where critically ill pediatric patients who require advanced airway, respiratory, and hemodynamic supports are usually admitted with the aim of achieving an outcome better than if the patients were admitted into other parts of the hospital. 1 The care of critically ill children remains one of the most demanding and challenging aspects of the field of pediatrics. The main purpose of the PICU is to prevent mortality by intensively monitoring and treating critically ill children who are considered at high risk of mortality. This, however, comes at a huge cost to all the parties involved–-the hospital, the personnel, and the care givers of patients. 2 It is usually only offered to patients whose condition is potentially reversible and who have a good chance of surviving with intensive care support. Since these patients are critically ill, the outcome of intervention is sometimes difficult to predict. In critical care medicine, intensive care unit (ICU) results can be assessed on the basis of outcomes such as “death” or “survival” by means of indicators such as mortality rates. Evaluation of the outcomes of medical interventions can assess the efficacy of treatment, making it possible to take better decisions, to further improve quality of care, to standardize conduct, and to ensure effective management of the high-level resources needed to deliver intensive care services thereby optimizing resource utilization. 3 Although mortality in patients depends on many factors such as demographic and clinical characteristic of population, infrastructure and non-medical factors (management and organization), case mix, and admission practice, it is also affected by ICU performance. 4 This study is, therefore, conducted to audit the pattern of cases being admitted into our PICU and their outcome. The term “audit” implies a professional commitment to improvement and involves a systematic approach highlighting opportunities for improvement and positive change in clinical practice. 5 It becomes important to audit admissions and their outcome with the aim of modifying practices if necessary following thorough introspection, leading to better patient outcomes.
Patients and Methods
This retrospective study reviewed the admissions into the PICU of a tertiary care center in India from August 2012 to June 2013. The hospital is an accredited residency training center and operates a well-equipped seven-bed modern PICU (with an isolation room), which admits pediatric patients ≤18 years of age, from both medical and surgical subspecialties. Patients undergoing cardiac surgery are admitted to a separate pediatric cardiothoracic intensive care unit (PCTICU) for immediate postoperative care, and are sometimes transferred to the PICU only when they are stable.
PICU records of all admissions, transfers out, discharges, and deaths were utilized for the purpose of this study. Data extracted from the records included age, sex, diagnosis, duration of stay in the unit, and outcome as far as the unit is concerned. Outcome is classified as transfers to step-down PICU or to the main pediatric wards, discharges, discharges against medical advice (DAMA), and death. Ethical approval was waived by the Ethics Committee of the hospital as this is a retrospective observational study.
The data obtained were entered into the Statistical Package for Scientific Solutions (SPSS) version 16.0 spreadsheet and analyzed. Means, standard deviations, percentages, and ranges were used as appropriate to describe continuous variables.
Results
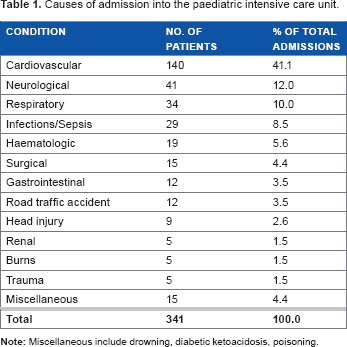
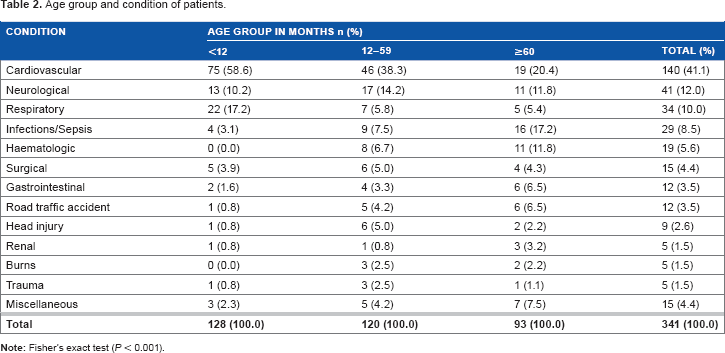
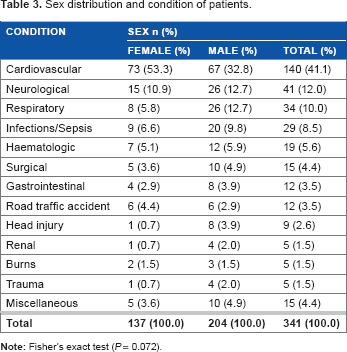
During the period of the study, a total of 341 patients were admitted into PICU. Of them, 173 (50.7%) were infants and 247 (72.4%) patients aged <5 years (infants included) (Fig. 1). Their ages ranged from one month to 15 years with the mean age being 40.01 ± 45.79 months. There were 204 (59.8%) male and 137 (40.2%) female patients giving an M:F ratio of 1.49:1. The three most common disease categories admitted were cardiovascular disease (41.1%), neurological disorders (12.0%), and respiratory disease (10.0%) (Table 1). “Miscellaneous” in Table 1 include drowning, diabetic ketoacidosis, and poisoning. The mean length of stay (LOS) in the PICU was 3.2 ± 4.5 days (range, 0–28 days). The majority of the patients (60.7%) were admitted for up to two days. Cardiovascular disorder was the commonest condition in children of all age groups (P < 0.001) (Table 2). A higher proportion of both females (53.3%) and males (32.8%) presented with cardiovascular diseases (Table 3). This relationship was, however, not statistically significant (P = 0.096).
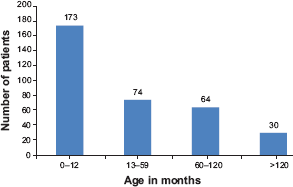
Age distribution of patients.
Causes of admission into the paediatric intensive care unit.
Age group and condition of patients.
Sex distribution and condition of patients.
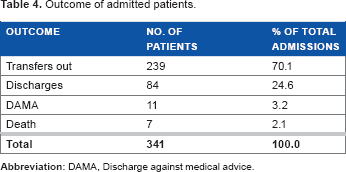
Two hundred and thirty-nine (70.1%) patients improved and were transferred to the pediatric wards for further management, 84 (24.6%) were discharged, and 11 (3.2%) left against medical advice (Table 4). Seven (2.1%) patients died during the period, consisting of five (71.4%) males and two (28.6%) females, with their mean age being 53.71 months (range, one month to 10 years). Two (28.6%) patients died of cardiovascular diseases, two (28.6%) of renal disorders, one (14.3%) of neurological problem, one (14.3%) of respiratory disease, and one (14.3%) of hematologic concerns. The overall mortality rate was 2.1%.
Outcome of admitted patients.
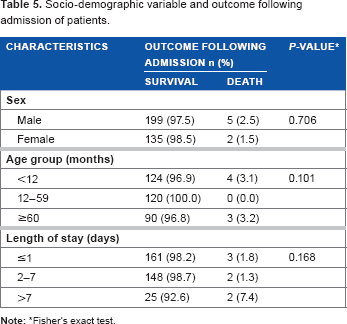
A higher proportion of males, 5 (2.5%), died following admission compared to females, 2 (1.5%). This relationship was not statistically significant (P = 0.706) (Table 5). The children in the age group 12–59 months had no deaths while those less than 12 months and those ≥60 months had higher proportion of deaths, 4 (3.1%) and 3 (3.2%), respectively. This relationship was not statistically significant (P = 0.101). Mortality among patients who stayed for one day or less was 1.8%, while it was 7.4% for those who stayed for more than seven days. A higher proportion of the children who stayed more than seven days in the PICU died. This relationship was also not statistically significant (P = 0.168) (Table 5).
Socio-demographic variable and outcome following admission of patients.
Discussion
This study revealed that cardiovascular, neurological, and respiratory diseases were the major causes of admission into the PICU of the tertiary care center studied. Criteria for admission into the unit include patients needing technological support such as mechanical ventilation and/or invasive monitoring. 6 It also includes patients who are critically ill but recoverable who need care other than that available in the general wards and post-surgical patients needing critical care. The fact that cardiovascular disease entity was the commonest (41.1%) cause of admission is not surprising as the healthcare center is a specialized pediatric cardiothoracic surgery center catering for all forms of congenital heart diseases pre-operatively, surgically, and post-operatively.
The PICU is a special unit primarily concerned with the care of patients with critical illness and demands a broad-based knowledge to cater for all aspects of management of these patients to achieve good outcome. 1 The main purpose of PICU is to prevent mortality by intensively monitoring and treating critically ill children who are considered at high risk of mortality. Although our patients included the entire spectrum from low to high risk ones, our retrospective study could not objectively determine the severity of our patients' conditions using tools like the Pediatric Risk of Mortality (PRISM) and the Pediatric Index of Mortality (PIM), 7 since they were not applied from the onset and so was not a part of the medical records. The ability to assess patient risk of death is very important since such estimate would be beneficial in realizing many different goals such as assessing patient's prognosis, ICU performance, and ICU resource utilization, and also evaluating therapies, controlling, and matching severity of illness in clinical studies. 7 Quantitative clinical scoring systems have been developed to overcome the lack of consistency, reliability, and accuracy in physician's subjective opinions concerning patient status as well as in response to increasing emphasis on the evaluation and monitoring of health services.
Seven (2.1%) patients died during the course of admission, giving an ICU survival rate of 97.9%. This value is in consonance with the mortality rate (2.6%) documented by Choi et al 8 for a five-bed PICU in a general hospital in Hong Kong. It is, however, less than an overall mortality of 6.7% and 16.7% recorded in India by Khilnani et al 9 and Bellad et al, 10 respectively, and 15% mortality rate was documented in Brazil by Costa et al 11 in 2010 for a tertiary care 15-bed PICU that receives both clinical and surgical cases but does not attend to trauma patients. Although Haque and Bano 12 documented similar average LOS in PICU with that of the present study, their overall mortality rate (14%) was higher. In this study, mortality among those who stayed for more than seven days (7.4%) was less than that (11.9%) recorded by El Halal et al 13 in the year 2012. ICU mortality rate varies depending on the case mix, age, LOS, and organisational aspects of the unit. 14 Although some studies reveal that there is correlation between LOS and outcome of pediatric patients, 15 others show no relationship. 16 Among those with significant relationship, there are contradictory findings as to how LOS affects outcome. 17 Klem et al 18 in their study documented that patients who died stayed approximately twice as long as survivors. Deaths use more resources in terms of bed days and diagnostic tests than survivors. 7 However, Kapil and Bagga 19 recorded lower mortality (9.8%) in long-stay patients (patients who stayed for more than 13 days) than in short-stay patients (24.6%). In this study, there was no significant relationship between LOS and outcome as was documented by Patil 16 in the year 2012. The severity of illness before ICU admission and presence of co-morbid conditions are also significant factors in patient survival. Our observed mortality rate was low. Important factors that may have contributed to survival in these patients include adequate manpower and equipment and provision of continuous medical education on pediatric critical care from time to time for staff by the institution.
Trauma-related cases constitute a sizeable proportion of admissions into our PICU and were made up of road traffic accidents (3.5%), head injuries (2.6%), burns (1.5%), and other forms of trauma (1.5%). Although trauma has been described as a disease of diverse nature and grades of severity recorded since antiquity, industrialization, technological advancement in means of transportation, and wars have resulted in alarming morbidity and mortality from trauma in recent times. Fortunately, no death was recorded for the trauma-related cases. Other than the trauma care protocols for the management of trauma victims in ICUs to reduce their mortality, measures to prevent road traffic accident (RTA) and other major causes of trauma in children must be employed. There is clearly a need for road safety education and it should be directed toward road users and those who are frequently involved and injured in RTAs. 20 An integrated program of road safety education is suggested. These include health education aimed at increasing understanding of child traffic accidents among parents, teachers, elected officers, and others interested in road safety; giving the facts about how, when, and where children have accidents and how these can be prevented.
The duration of stay in the PICU is an index of severity of morbidity, although this cannot be interpreted in isolation. Morbidity is broadly defined as the health-related quality of life in or out of hospital. 21 It is affected by previous health status and residual disability. In this study, the mean duration of stay in PICU was 3.2 ± 4.5 days, which is similar to the records of Haque and Bano 12 in Pakistan, but in contrast, a mean duration of 4.52 ± 2.6 days was reported by Khilnani et al. 9 Our facility upholds the international standard of one intensive care nurse/bed/shift producing high quality of care with a high intensity physician staffing resulting in lower mortality and shorter hospital and ICU stays. 22
Some patients remained in the unit for as long as 28 days either because they required critical care for the period or for logistic reasons in which case there may be no bed space at the step-down ICU or main pediatric wards to enable their transfer. This resulted in full recovery of some patients in PICU necessitating discharge home directly from the ICU amounting to an improper use of the ICU as not only a high-dependency unit but also as a general ward with full recovery of patient. The absence of a high-dependency unit at our center led to the admission of some patients who were not ill enough to require ICU admission into PICU. The aforementioned situations need to be checked to enhance cost–-effective management of patients and avoid unnecessary stretch of the ICU facilities. This trend is changing following reorganization of the facilities.
An effective ICU goes a long way in reducing morbidity and mortality. With low mortality rate, we would say that total quality management of our PICU patients was optimal. We conclude that a well-equipped ICU with modern and innovative intensive care greatly facilitates the care of critically ill patients giving desirable outcome.
Footnotes
Author Contributions
Conceived and designed the experiments: BIA-I and NKKV. Analyzed the data: BIA-I. Wrote the first draft of the manuscript: BIA-I. Contributed to the writing of the manuscript: SKP and NKKV. Agree with manuscript results and conclusions: BIA-I, SKP, and NKKV. Jointly developed the structure and arguments for the paper: BIA-I, SKP, and NKKV. Made critical revisions and approved final version: BIA-I, SKP, and NKKV. All authors reviewed and approved of the final manuscript.