
Abstract
Dengue hemorrhagic fever (DHF) is a spectrum of disease ranging from uncomplicated febrile illness to various devastating hemorrhagic manifestation and refractory shock. Cardiac complication in dengue fever (DF) is not common. Myocarditis has been a known complication of dengue fever. We report the case of myocarditis complicating DHF in a 34 years old female at 36 weeks of gestation with probable fetal myopericarditis.
Introduction
Dengue fever (DF) is caused by the dengue virus which belongs to the family Filoviridae. The clinical spectrum of DF ranges from an uncomplicated febrile illness to devastating hemorrhages and refractory shock. Cardiac complications of DF are not common. We report a case of myocarditis complicating dengue hemorrhagic fever (DHF) in a pregnant woman with probable fetal myopericarditis.
Case Presentation
A 34 years old female G5P(3+1) presented at 36 weeks and 5 days of gestation with a prodrome of fever for four days and dyspnoea for one day. There was no history of chest pain, palpitations or cough. There was no history of hematamesis, hematochezia, hematuria, vaginal bleeding, gum bleeding, or petechae. All her previous pregnancies were uneventful. She did not give any history of significant ailments in the past. On examination she was conscious and fully oriented with mild pallor and generalized erythematous blanching of the skin. Her pulse was 96/min, blood pressure (BP) was 130/80 mm of Hg, and she was tachypnoeic. There were no petechae or mucosal bleeding. Respiratory system examination revealed bilateral crepitations. Cardiovascular examination was unremarkable. Uterus size on abdominal examination was corresponding to gestation.
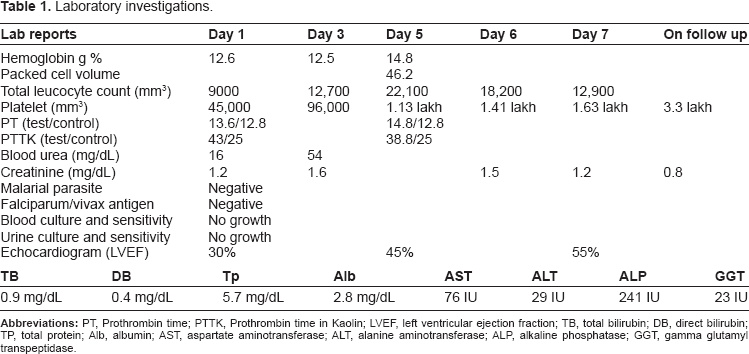
The initial investigation (Table 1) revealed thrombocytopenia (45,000/mm3) with mild rise in serum creatinine (1.6 mg/dL). Dengue IgM was positive in her serum. Serial ECG's revealed ST-T changes in the chest leads. The initial Echocardiogram revealed global hypokinesia with reduced ejection fraction of 30%. Cardiac chambers were not dilated. Chest X-ray revealed bilateral non-homogenous opacities suggestive of pulmonary edema. Ultrasonography (USG) for fetal wellbeing revealed pericardial effusion and ascites.
Laboratory investigations.
After admission into the hospital her BP gradually dropped to 90/80 mm of Hg, which responded to inotropes. She was monitored in the cardiac care unit. Fetal wellbeing was monitored daily by USG. On the second day it was noted that there was no fetal cardiac activity. She was electively induced and the fetus was delivered vaginally.
Her serial platelet counts (Table 1) revealed a gradual rise and by the seventh hospital day, platelet levels were 1,63,000/mm3. The rise in creatinine could be attributed to the hypotension or due to the direct effect of the infection. However it returned to normal with conservative management (Table 1).
Serial echocardiogram revealed left ventricular ejection fraction (LVEF) of 45% on the 5th day. She had normal left ventricular function on echocardiogram (LVEF 55%) and normal ECG recordings by the seventh hospital day. There was complete resolution of pulmonary shadows on Chest X-ray. She was discharged in a satisfactory condition and has been doing well subsequently.
Discussion
Dengue infection is a self limiting infection. DHF manifests as a spectrum of disease ranging from an uncomplicated febrile illness to various hemorrhagic manifestation and refractory shock. The various pathogenic mechanisms involved are thrombopathy, vasculopathy and coagulopathy. Cardiac manifestations, though recognized in DF, are not very common. Myocarditis is the most common documented cardiac pathology in DF. Only a very few cases have been reported.
Wiwanikit postulated the low incidence of dengue myocarditis be due to the rarity of cases or under diagnosis and under reporting. 1 Horta Velosa et al noted cardiac rhythm disturbances including atrioventricular blocks and ventricular ectopics that appear during infection and attributed them to viral myocarditis. 2 Dengue endocarditis has never been reported. Dengue pericarditis may be seen but is very rare and in the form of myopericarditis, the pathogenesis of which may be due to the extension of myocarditis. 3
Wali et al, in a study of 17 patients with DHF/ DSS, noted that acute reversible cardiac insult may be present in DHF/DSS and which may be responsible for hypotension or shock seen in some of these patients. 4 Mendez et al, in a study of 913 children with DHF, mentioned cardiac involvement in 8% of the children. 5
The various possibilities considered in this patient were peripartum cardiomyopathy and valvular heart disease in addition to viral myocarditis. Echocardiogram did not reveal any dilation of chambers or evidence of valvular heart disease. Points favoring myocarditis were the clinical picture of fever, cardiac failure, and hypotension. However global hypokinesia with low ejection fraction which reverted to normal along with dengue IgM, being positive favored the etiological diagnosis.
Raised creatinine observed in this patient was supported by the previous studies, where acute kidney injury was noted in DHF. 6 This patient's creatinine reverted back to normal with conservative management.
Various studies have looked into the effect of DF on pregnancy. There are several pregnancy-related issues that might confuse the unsuspecting obstetrician. These include common alterations in the immune, coagulation, and cardiovascular systems as well as hepatic enzymes and the febrile response to illness during pregnancy. 7 During pregnancy the white blood cell count is typically elevated with a shift to the left. Thus, such a minor change due to DF might be overlooked. Similarly, pregnancy results in an increased tendency toward coagulopathy while at the same time the platelet count is normally low. How these factors might interact with the course and laboratory finding in a case of DHF is unclear. The hemoconcentration that occurs with DHF may also be masked by the normal hemodilution of pregnancy. 8
Carles et al in their review of 38 cases in French Guiana indicate a significant increase in prematurity and fetal death in severely ill hospitalized patients.9,10 They noted that if they had included patients with milder disease, the incidence of fetal death and prematurity would have been less. Ismail et al in a recent review reported three maternal deaths out of 16 cases with prematurity in 50% neonates. 11 In the Perret study, there appeared to be no fetal effect from the maternal dengue infection. 12 Sharma et al reported an increased incidence of neural tube defects following dengue infection, but as this defect has been demonstrated following other febrile illnesses, it may well have been due to the fever rather than to any teratogenic effect of the dengue virus per se. 13
Sixteen of the 17 (94%) infants with vertical transmission reviewed by Sirinavin et al survived without sequelae, with one (6%) neonatal death due to intracerebral hemorrhage. 14 Perrett et al came to the conclusion that serious dengue disease occurs only when the mother is at or near term as there is insufficient time for the maternal production of protective antibodies. 12
Conclusion
DHF can have non hemorrhagic manifestations like myocarditis. Adverse fetal outcome can be expected if mother has dengue infection nearing term and if the mother is severely ill. This is possible the first report in medical literature of both maternal myocarditis and fetal myopericarditis complicating DHF.
Footnotes
Author Contributions
Conceived and designed the experiments: KJM. Analysed the data: KJM. Wrote the first draft of the manuscript: KJM. Contributed to the writing of the manuscript: KJM, JM. Agree with manuscript results and conclusions: KJM, JM. Jointly developed the structure and arguments for the paper: KJM, JM. Made critical revisions and approved final version: KJM, JM. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.