
Abstract
Introduction
Invasive fungal rhinosinusitis is a challenging condition that can be found mostly in immunocompromised patients. Failure to diagnose and treat this entity promptly usually results in rapid progression and death. The purpose of this study was to determine clinical presentation, complication and morbidity in patients with acute versus chronic invasive fungal rhinosinusitis.
Setting and design
Case-control study at Srinagarind Hospital, Khon Kaen University between January 1998 and May 2008.
Methods
The patient's data with the diagnosis of invasive fungal rhinosinusitis was included. Demographic data, underlying diseases, presenting symptoms, histologic sinonasal tissue evaluations, sinonasal tissue cultures, CT scan findings, surgical interventions, morbidity, and mortality were collected.
Results
Sixty-five patients were diagnosed as invasive fungal rhinosinusitis between January 1998 and May 2008. The data of six patients were unable to obtain. Fifty-nine patients were included in this study. Patients with immunocompromised status have significant greater risk for acute than chronic IFS, OR = 6.5 (P = 0.004). Patients with mucosal necrosis have the significant higher risk for acute IFS, OR = 5.5 (P = 0.01). There was no significant difference in orbital complications proportion between acute and chronic invasive fungal rhinosinusitis, OR = 2.42 (P = 0.15). Sinus wall erosion have found significantly in chronic IFS group, OR = 0.24 (P = 0.02). The average hospital stayed was 30.58 ± 26.43 days with no difference between groups (P = 0.50). Fourteen patients in acute IFS group were dead (31.11%) while all patients in chronic IFS group were survived.
Conclusions
Invasive fungal rhinosinusitis continues to present a challenge to the otolaryngologist. Acute IFS was found most commonly in immunocompromised patients. The most consistent finding of acute IFS was mucosal necrosis and black crust/debris. The CT finding of sinus wall erosion may help in diagnosis of chronic IFS.
Introduction
Invasive fungal rhinosinusitis (IFS) is a challenging condition that commonly seen in immunocompromised patients. Diagnosis of invasive fungal sinusitis requires histopathologic evidence of fungi invading nasal tissue; hyphal forms within the sinus mucosa, submucosa, blood vessels, or bone. Invasive fungal sinusitis can be subdivided into acute and chronic invasive sinusitis. Some authors further subdivided chronic invasive sinusitis to granulomatous invasive sinusitis1,2 but clinico-pathological distinctions between these conditions are still not clear.
Acute invasive rhinosinusitis results from the rapid spread of fungi from the nasal and sinus mucosa by way of vascular invasion into the orbit, vessels, and parenchyma of the brain. Less than 4 weeks duration separates the acute stage from the chronic stage of the disease. 3 Chronic invasive fungal rhinosinusitis results from a slowly progressive fungal invasion. As opposed to the neutrophil-rich, highly necrotic, and angiotrophic process seen in acute invasive fungal rhinosinusitis, there is a low-grade mixed cellular infiltrate in affected tissues.4,5
Aspergillus and Rhizopus species are most common isolated fungal pathogen.6,7 However, fungal culture or pathological results take days to weeks. This makes for a challenge in the diagnosis of invasive fungal rhinosinusitis. The initial diagnosis is usually made solely by patient's symptoms and clinical examination.
The most consistent physical finding is an alteration in the appearance of the nasal mucosa. Mucosal discoloration can be variable, and may be gray, green, white, or black. Discoloration, granulation, and ulceration typically replace the normal pale-pink mucosa. The black discoloration is a late finding of tissue necrosis. 8 Radiological studies can be helpful in advanced cases, showing extrasinus extension and bone erosion. 9
Treatment of invasive fungal rhinosinusitis consists of surgery and antifungal therapy. Acute invasive fungal rhinosinusitis needs more aggressive debridement due to high recurrence, mortality and morbidity rate. Amphotericin B 1–1.5 mg/kg/day for a total dose of 2 grams or more is the gold standard antifungal therapy. Voriconazole is the treatment of choice for invasive aspergillosis rhinosinusitis. 10
The incidence of morbidity and mortality of invasive fungal rhinosinusitis ranged from 20 to 80 percent. 11 Failure to diagnose and treat this entity promptly, usually results in rapid progression and death. The purpose of this study was to determine clinical presentation, complication and morbidity in patients with acute versus chronic invasive fungal rhinosinusitis.
Materials and Methods
Study design and setting
We conducted a case-control study of invasive fungal rhinosinusitis at Srinagarind Hospital, Khon Kaen University, Thailand between January 1998 and May 2008. The hospital is the largest tertiary hospital in north east region of Thailand. Most of invasive rhinosinusitis patients were referred to our hospital.
Case and control definition
Cases were patients with acute invasive fungal rhinosinusitis (acute IFS). Acute IFS was defined as histopathological evidence of fungi invading nasal or sinus mucosa or deeper tissues with clinical symptoms onset of 30 days or less. Controls were patients with chronic invasive fungal rhinosinusitis (chronic IFS). Chronic IFS was defined as histopathological evidence of fungi invading nasal or sinus mucosa or deeper tissues with clinical symptoms onset of more than 30 days.
Data Collection
Cases and Controls were identified through the hospital registry system and rhinosinusitis registry between June and December 2008. The outpatient and inpatient data was reviewed. A data collection form detailing demographic data, underlying diseases, presenting symptoms, histologic nasal tissue evaluations, nasal tissue cultures, CT scan findings, surgical interventions, morbidity, and mortality were completed. If the data was missing, we will call or mail to the address that patient provided.
Statistical Analysis
A statistical analysis was conducted using Stata (version 9, StataCorp LP, Texas, USA). Continuous variables were analyzed using the unpaired t test or Mann-Whitney U test for continuous variables vs. the Pearson's χ 2 -test for categorical variables, as appropriate to analyze statistical significant difference of the potential risk factors between the two groups: those who had acute invasive fungal rhinosinusitis (acute IFS) and those who had chronic invasive fungal rhinosinusitis (chronic IFS). The odds ratio and 95% confidence intervals (CI) were calculated to compare the risk factors among the two groups. For all tests, P < 0.05 was considered to be statistically significant.
Ethics
Approval was sought from the Khon Kaen University Ethics Committee for Human Research before initiating the study. As this was a retrospective study, the need for an informed consent was waived by the ethics review board.
Results
Sixty-five patients were diagnosed as invasive fungal sinusitis between January 1998 and May 2008. We were unable to obtain the data of six patients. Fifty-nine patients were included in this study.
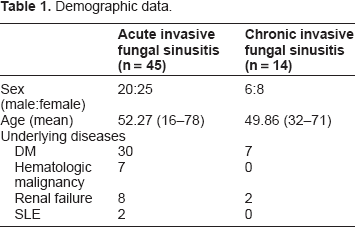
Forty-five patients were diagnosed with acute IFS (76.3%) and fourteen patients with chronic IFS (23.7%). There were 26 males (44.1%) and 33 females (55.9%). The average age of patients was 51.69 years (range, 16–78).
Demographic data.
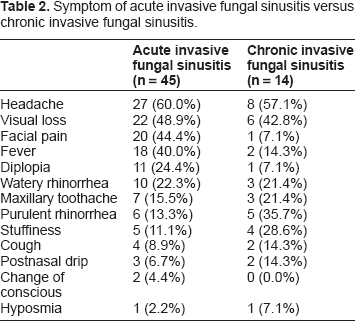
Symptom of acute invasive fungal sinusitis versus chronic invasive fungal sinusitis.
Rhinologic signs of acute invasive fungal sinusitis versus chronic invasive fungal sinusitis.

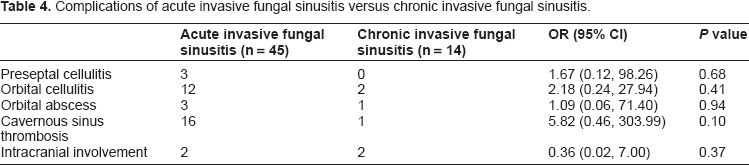
Complications of acute invasive fungal sinusitis versus chronic invasive fungal sinusitis.
The CT scan of paranasal sinus was performed in 53 patients and MRI of the paranasal sinus was performed in 4 patients. The CT findings were sinus wall erosion, mucosal thickening and air-fluid level. Sinus wall erosion was found to be significant in the chronic IFS group, odds ratio = 0.24 (95% CI 0.06 to 1.02, P = 0.02).
Five different fungal pathogens were isolated from nasal tissue cultures. Rhizopus spp. was the most common isolated organism, followed by Aspergillus spp.
The histopathology findings shared the same results, Rhizopus spp. was the most common organism followed by Aspergillus spp.
All patients underwent endoscopic debridement or external approach and received amphotericin B. The average hospital stay was 30.58 ± 26.43 days with no difference between groups (P = 0.50). Fourteen patients in acute IFS group were dead (31.11%) while all patients in chronic IFS group were survived.
Discussion
The phagocytic system is critically involved in protecting the individual from invasive fungal disease. Patients, who have had qualitative or quantitative abnormalities such as hematologic malignancy disease, AIDS, hematologic disease, organ transplantation and diabetes mellitus are particularly susceptible to fungal infections. 12 We found that the immunocompromised host has the higher risk for acute IFS (P = 0.004). The immune system may play a role in slowing the invasion process of fungus as appeared in chronic IFS.
An increase in the prevalence of invasive fungal rhinosinusitis is thought to be secondary to increasing numbers of immunocompromised patients.13–15 Medical advancements have prolonged the survival of immunocompromised patients, which has in turn increased the population at risk for developing invasive fungal rhinosinusitis. 16 Acute invasive fungal sinusitis has the highest morbidity and mortality rate. Immunocompromised patients have up to twice the mortality rate, compared to immunocompetent patients. 11 Survival is dependent on the early detection of the disease, followed by aggressive surgical and medical management. 14
The symptoms of invasive fungal rhinosinusitis are often subtle and initially difficult to diagnosis. We found that the common presenting symptoms were headache, visual loss, facial pain and fever. Up to 90 percents of patients had fever of unknown origin that was non-responsive to 48 hours of appropriate broad-spectrum intravenous antibiotics. 17 The absence of fever does not rule out this condition, especially in patients with localizing symptoms such as facial, periorbital pain, nasal congestion, rhinorrhea, and headache, which are present between 20 to 60 percents of patients.16,18 The physician should keep in mind of this condition especially in immunocompromised patients.
The physical examination is an important step to diagnosis of invasive fungal rhinosinusitis. Black crust/debris was the hallmark in the rhinologic findings of IFS, and this finding is consistent in many studies. The conventional anterior rhinoscopy and posterior rhinoscopy may not be adequate to visualize some parts such as middle meatus. We encourage the endoscopic nasal examination in all patients. A thorough head and neck examination should be performed on all patients in addition to the endoscopic nasal evaluation. Prompt diagnosis and treatment has a positive impact on patient survival rates.
Acute IFS had more severe rhinologic manifestations, such as mucosal necrosis (P = 0.01). There was no difference in orbital complication rates across the two groups (P = 0.15). The CT scan of paranasal sinus is the essential tool for diagnosis of invasive fungal sinusitis. Our CT findings were consistent with other literature. Mucosal thickening and absence of bone erosion are features of acute invasive fungal sinusitis19,20 while sinus wall erosion was found to be significant in the chronic invasive fungal sinusitis group (P = 0.02).
Treatment of invasive fungal rhinosinusitis included the combination of antifungal antibiotics and aggressive surgical debridement.13,15,18,21–25 Amphotericin B total dose of 2 grams or higher is an important adjunct in the treatment of invasive fungal rhinosinusitis.
This study has the limitation of being a retrospective case-control study. Limitations arising from sample selection and data collection, this analysis cannot reflect every aspect of IFS. Although our series was relatively large, the sample size was not adequate to perform the regression analysis.
Conclusion
With a high mortality rate, the diagnosis and management of invasive fungal sinusitis continues to present a challenge to the otolaryngologist. Acute invasive fungal sinusitis is found commonly in immunocompromised patients, with the highest incidence in patients with diabetes mellitus. The most consistent finding of IFS was mucosal necrosis and black crust/debris. The CT Finding of sinus wall erosion may help in diagnosis of chronic invasive fungal sinusitis.
Funding Sources
None.
Competing Interests
The author(s) declare that they have no competing interests.
Author Contributions
PP designed the study protocol, collected the patient's data, analyzed the data and wrote the first draft of manuscript. ST designed the study protocol and revised the manuscript. All authors read and approved the final manuscript.
Footnotes
Acknowledgements
The authors thank the staff and nurses at Srinagarind Hospital for their excellent care of the patients enrolled in this study.
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.