
Abstract
The treatment and prevention of influenza virus infection has been associated with two major challenges that are exemplified by 2009H1N1 as well as previous pandemics. The constant evolutionary pressure on the influenza virus can result in novel strains which may not be optimally protected by vaccines or currently approved antivirals. Selection for antiviral resistance mutations can occur over time. Prolonged virus shedding, selection for resistance mutations, and cross resistance, can be exacerbated and problematic in immunocompromised patients. This review will cover 2009H1N1 infection in immuno-competent and immunocompromised individuals. Influenza continues to be a major public health concern and these challenges make influenza a suitable area for new vaccine and antiviral approaches.
Introduction
The 1918–19 influenza (IFV) pandemic had an estimated mortality of 40–100 million deaths worldwide and is considered the one of the worst public health disasters of the twentieth century. 1 In 2009 a new influenza pandemic occurred with the emergence of a novel swine influenza strain 2009H1N1. 2
The counter-response to influenza includes both vaccines and antiviral drugs. Vaccines remain the primary approach to preventing influenza but require apriori understanding of the antigenic breath prior to influenza season. Antiviral drugs are an important therapeutic and preventative modality for influenza. This review will focus on 2009H1N1 and antiviral treatments in the immunocompetent as well as immunocompromised patients. Our search strategy included the National Library of Medicine (PubMed) and manufacturers trial data bases available on the internet.
2009H1N1
2009H1N1strain emanated from the viral evolution of the two influenza surface proteins Hemagglutinin and Neuraminidase. Hemagglutinin (HA) functions in the binding of the virus to the sialic acid receptors on respiratory epithelium. Neuraminidase (NA) releases progeny virus from the cell, thereby enabling them to infect additional cells and continue viral replication. Antigenic drift are relatively minor changes in the HA or NA amino acids that occur during viral evolution. Antigenic shift are more dramatic change occurs when components of different influenza viruses recombine in a host and form a novel strain. Typically there is limited pre-existing immunity to a new pandemic strain in most of the population. The emergence of 2009H1N1 was a result of both viral evolution and cross-infection between humans, birds, and pigs of previously circulating strains. 3 Human H1N1 influenza virus that circulated from 1918 to 1957 probably came from avian origin and then disappeared but reappeared in 1977. 4 Sporadic cross-species influenza infections from swine to humans had been noted since 1958. An outbreak of swine influenza occurred among military recruits in 1976 in Fort Dix, New Jersey. 5 In 1977 there was a re-emergence of H1N1 in humans. 6 Cross-species infection of human influenza H1N1 infection in pigs was confirmed in 1979. 7 The first avian origin influenza was described in European swine in 1981. A triple re-assortment swine influenza virus was identified in North America and had components of the swine influenza virus, but also had component of both avian and human influenza. 8 2009H1N1 appears to have components of Eurasian and North American Swine, North American avian, and North American human influenza viruses.9,10
Most recently in 2012, new variant influenza viruses have been described. These viruses have been designated as A(H1N1)v, A(H3N2)v and A(H1N2)v. These are novel influenza viruses that circulate in animals that may infect humans. In the second half of 2011, the US Centers for Disease Control (CDC) reported that twelve US residents have been found to be infected with A (H3N2)V. 11 As with 2009H1N1, these are novel viruses and there may be no preexisting immunity. 12 Genomic sequencing of some of these viruses has revealed the Matrix (M) gene from A (H1N1), with similar antiviral drug susceptibility as 2009H1N1. 13
Clinical Spectrum of 2009H1N1 in Immunocompetent Hosts
The clinical spectrum of 2009H1N1 so far has varied from asymptomatic cases to primary pneumonia resulting in respiratory failure, acute respiratory distress, multi-organ failure, and death. 14 Initial clinical reports of 2009H1N1 in hospitalized patients resulted in fears that the pandemic could have a very high mortality rate as high as 41%. 15 However, these reports may have overestimated mortality due to selection bias. Most clinical illness caused by 2009H1N1 were self limited with the highest attack rates among children, young adults, and certain high risk populations. 2009H1N1 resulted in typical influenza symptoms including fever, cough, sore throat, myalgia, malaise, chills, rhinorrhea, conjunctivitis, headache, and shortness of breath. However, in contrast to typical flu symptoms, up to 50% of those infected with 2009H1N1 presented with gastro-intestinal symptoms including vomiting and diarrhea. 14 The relative sparing of the elderly by 2009H1N1 contrasted with previous seasonal influenza infections. This major difference in epidemiology was presumably due to cross reactive immunological memory of older adults who had previously been exposed to related viruses and may have had some level of protection. Thus 90% of deaths occurred in the non-elderly individuals under 65 years of age. 16 The overall death rate for 2009H1N1 was estimated to be 0.5%. Although most patients who were hospitalized or died had no underlying risk factors, other risk factors have been identified. Pregnant women and women less than 2 weeks post-partum were identified at greater risk for more severe infection. 16 For example, although pregnant women represent approximately 1% of the population, they accounted for up to 10% of those hospitalized with influenza complications. 16 In addition, patients with neurologic conditions, or immune suppression were noted to have a greater risk for complications. 13 Patients with severe or morbid obesity were also represented higher rates of hospitalizations and deaths due to 2009H1N1 compared to the general population. 16 Other chronic conditions that were identified as risk factors for more severe disease of 2009H1N1 were cardiovascular disease, lung disorders, diabetes, Sickle cell disease, renal disease, and hepatic disease. 16
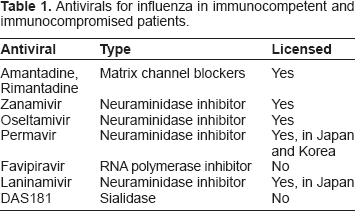
Approved Influenza Antivirals for Immunocompetent Individuals (Table 1)
Antivirals for influenza in immunocompetent and immunocompromised patients.
Clinical efficacy and safety adamantanes (M2 ion channel blockers) in immunocompetent individuals
The first antivirals developed for the treatment of influenza were a class of drugs called adamantanes (amantadine and rimantadine). 17 Amantadine was first approved for treatment and prophylaxis in 1967, while rimantidine was approved in 1993. These drugs are M2 ion channel blockers and are thought to interfere with viral un-coating inside the cell. These drugs are limited to activity against influenza A. Amantadine, and to a greater extent rimantadine, can be associated with nervous system side effects such as insomnia, confusion, hallucinations, ataxia, difficulty in concentration, depression, dizziness, and tremor. These drugs can also cause gastrointestinal side effects including anorexia, nausea and vomiting. 18
A meta-analysis review of published treatment studies suggests that amantadine was responsible for a relative reduction of 61% of influenza cases when used in the prophylaxis of influenza A and can shorten the duration of illness including fever by 1 day against susceptible strains. 18 Rimantidine appears to be equally effective for prophylaxis, preventing approximately 71% of influenza A cases and has also been shown to decrease the duration of fever by approximately 1 day. 18
Admanatane resistance in immunocompentent individuals
Adamantanes are limited in their clinical usefulness against influenza because of widespread resistance. Amantidine-resistant influenza A virus was first detected in 1981 with known genetic basis. 19 Resistance-associated amino acid substitutions have been well described in H3N2 (Ser31 Asn) and H1N1 (Val27 Ala) strains. Adamantane resistance develops very rapidly in influenza A viruses, and in particular for H3N2 strains. Adamantane resistance can occur as early as 2 days after drug treatment and can be found in up to 80% of some pediatric subjects after treatment. 19 On a population level, the incidence of resistance to the adamantanes has increased from less than 20% in 2003 to 92% in 2005 in the US. 19 Although this dramatic increase in resistance may have been due to increased usage of these drugs, it has also been noted in controls with low such as in Australia. 19 Resistant viruses appear to cause disease severity similar to wild type virus infection.
With regard to 2009H1N1, both approved adamantanes have no antiviral activity towards M2 channel, due to the mutation of Ser31.16,20 The M gene within this new pandemic influenza virus is reportedly similar to the M gene in the Eurasian Swine virus, which confers resistance to both amantadine and rimantidine. Thus these drugs are not useful for 2009H1N1.
Clinical Efficacy and Safety of NAI Inhibitors in Immunocompetent Individuals
The most common class of antivirals approved for the treatment and prophylaxis of influenza are Neuraminidase inhibitors (NAIs). NAIs interfere with the release of new influenza virus particles from infected cells preventing infection of new cells. In general, this class of antivirals is associated with less toxicity than the adamantanes. Also, unlike the adamantanes, the NAIs have activity against both influenza A and B.
The inhalant form of zanamivir (Relenza®) was the first NAI approved for the prophylaxis and treatment of influenza (July of 1999).21,22 The second drug in this same class, oral oseltamivir (Tamiflu®) was approved in October 1999.
Based on a meta-analysis of eight randomized controlled trials of zanamivir and nine trials of oseltamivir, both drugs are effective in reducing the median time to alleviation of influenza symptoms. 23 For zanamivir, the intent to treat analysis suggested a median time to alleviation of symptoms ranged from 0.78 days in healthy adults to 1 day in children. For oseltamivir analysis suggested a median reduction in time to alleviation of symptoms of 0.86 for healthy adults to 0.87 days for children in intention to treat populations.
Although the effects of NAIs on shortening the duration of symptoms is well documented, a recent review suggested that current data was insufficient to support claims that oseltamivir prevents secondary complications including those requiring hospitalizations from influenza including hospitalizations.24,25
For prevention, three trials of zanamivir and four trials of oseltamivir were examined in one meta-analysis. 23 For seasonal prophylaxis, a 69% relative reduction in the incidence of influenza was observed in the zanamivir treated group compared to controls. In post-exposure prophylaxis studies, an 81% relative reduction in infection was observed for zanamivir treated patients. For oseltamivir, a 74% relative reduction in the incidence of influenza infection was observed in seasonal influenza studies and a 90% relative reduction was observed in post-exposure prophylaxis studies. An investigational intravenous form of zanamivir has also been tested in a preventative virus challenge model and was shown to decrease shedding and infection. 25
A recent study investigated the use of combination therapy (zanamivir and oseltamivir) versus either oseltamivir or zanamivir monotherapy in 541 patients with confirmed 2009H1N1. 26 Combination therapy was less effective than oseltamivir monotherapy and not significantly more effective than zanamivir monotherapy in terms of the endpoints of viral load and time to alleviation of symptoms. Unlike other viral diseases, where combinations of antivirals have been successful, these results raise concern that such a combination antiviral approach may have limited utility to treat influenza.
As noted earlier, in general, the NAIs are well tolerated. However, post-licensing reports have indicated that zanamivir may cause cough, bronchospasm, or even death in patients with pre-existing pulmonary disease. This antiviral is contraindicated in patients with serious underlying respiratory diseases who have other treatment options. 27
NAI drug resistance in immunocompetent individuals
For 2009H1N, the recommended antiviral therapy in the normal host is oseltamivir, as the 2009H1N1 virus is typically resistant to the adamantanes. 28 This is in contrast to the 2008–2009 seasonal H1N1strain which was characterized by oseltamivir resistance and amantadine susceptibility. 29 The US Centers for Disease Control (CDC) has recommended that patients with suspected or confirmed oseltamavir resistant 2009H1N1 be treated with zanamivir. 30 If orally inhaled zanamivir is contraindicated or not well tolerated, then intravenous (IV) zanamivir is available for compassionate use from its manufacturer via an emergency Investigational New Drug (IND) application to the FDA.
The US CDC also recommends that patients infected with suspected or documented H274Y mutant virus should not be treated with peramivir because clinical isolates expressing the oseltamivir resistance-associated substitution H274Y in the neuraminidase gene have demonstrated reduced peramivir susceptibility in vitro. Of note, a recent report examined IFV strains from 2008–2010 and found 28 isolates that were resistant to both the adamantanes and oseltamivir. 31 In addition, a recent report in 2011 from the WHO has noted H274Y resistance in 14% isolates from Australia. 32 The emergence of resistant virus is of obvious great public health concern.
The Clinical Spectrum of 2009H1N1 in Immunocompromised Individuals
The impact of seasonal influenza on immunocompromised individuals has been characterized through case studies. Complications in this population include increased mortality, need for mechanical ventilation, progression to lower airway disease, high rates of secondary infection, and persistent viral shedding.33,34 There are a number of risk factors that result in an increased susceptibility to influenza infection in immunocompromised hematopoietic stem cell transplant patients (HCT) including myeloablative regimens, lymphopenia, and the intensity of immunosuppression are risk factors associated with respiratory infections including influenza. 35 IFV in the immunocompetent host usually results in viral shedding that is typically self-limited, lasting five to six days. By contrast, prolonged viral shedding of greater than 2 weeks can be common in immunocompromised hosts. In some reported cases, viral shedding in immunocompromised patients can last as long as six months.36,37 Prolonged viral replication and shedding may be associated with an increase in the selection of resistant virus. For example, in one small series of HCT subjects, the rate of NAI resistance was 67%. 38 Many other studies suggest that the incidence of resistance is much higher in immunocompromised patients compared to immunocompetent adults or children. 39 In addition to drug resistance, morbidity and mortality from influenza appears to be much higher in immunocompromised individuals compared to immunocompetent patients. 33 For example, the overall mortality after diagnosis of pneumonia can be as high as 30%. 33 Lymphopenia appears to be an important risk factor for developing influenza lower airway disease such as pneumonia. 41
A number of severe cases of 2009H1N1 infection resulting in significant mortality and morbidity have been described in both HCT and solid organ transplant (SOT) patients. In SOT, a large study examined 237 cases with 2009H1N1. 41 Thirty-two percent of these patients had pneumonia. Sixteen percent were admitted to intensive care and four percent died.
Outcome of 27 cases of 2009H1N1 was examined in a study from two centers after HCT. 42 Influenza-related 30-day mortality was 22% overall, but patients with lower respiratory tract infection (LRTI) had a 43% mortality rate. Progression from upper tract to lower tract disease therefore has an important impact on mortality. Chronic steroid use (≥20 mg/day of prednisone equivalent) at the time of presentation was a risk factor for LRTI and death.
The high mortality from lower track influenza disease in HCT was also observed in another small study of 2009H1N1. 43 Five of 13 patients had 2009H1N1 influenza-induced lower respiratory tract infection and only 1 survived. The authors noted that lower respiratory tract disease and poorer outcomes occurred in patients receiving intense immunosuppressive therapy who were neutropenic and had Graft Versus Host Disease (GVHD).
Clinical effficacy and safety of NAI's in immunocompromised patients
The antiviral treatment options for immunocompromised patients are empiric and dependent on the particular strain and its known sensitivity. Immunocompromised patients infected with IFV can experience prolonged infection and shedding, usually for longer than five days. Thus longer duration NAI treatment is usually required. However, the specific duration of treatment is often empiric and not standardized. There are no randomized controlled studies available that have examined the specific duration of treatment with NAI's in immunocompromised patients.
Therefore optimal therapy for severely immunocompromised patients with oseltamivir-resistant 2009H1N1 has not been clearly defined. Some severely immunocompromised patients with 2009H1N1 have been treated with a combination of Intravenous (IV) zanamivir and aerosolized ribavirin therapy 44 or IV zanamivir monotherapy although no controlled studies have confirmed the efficacy of these combination approaches. 45
NAI drug resistance in immunocompromised patients
Antiviral drug resistance has been a notable feature of case reports of 2009H1N1 infection in transplant patients. For example, a case report has recently described the viral kinetics of an immunocompromised patient infection with 2009H1N1. 46 In this case, resistance to oseltamivir was observed 10 days after initiation of antiviral treatment. The patient was then treated with zanamivir for 12 days. Viral loads remained high after 5 days of zanamivir but then declined with an additional 7 days of treatment.
The problem of drug resistance related to 2009H1N1 in immunocompormised patients was also highlighted by The US CDC who described two cases early in the 2009H1N1 pandemic in immunocompromised individuals. 47 The first patient developed influenza like symptoms approximately 30 days after HCT. The patient was treated for over six weeks with oseltamivir, due to persistent infection, as documented by Polymerase Chain Reaction (PCR). Mutant variants containing the H274Y mutation were detected in samples within two weeks after treatment was initiated with oseltamivir. A second patient developed respiratory symptoms after two cycles of chemotherapy. This patient was initially treated with oseltamivir and rimantadine. The mutation conferring oseltamivir resistance (H274Y) was detected and treatment with oseltamivir was discontinued. Treatment with inhaled zanamivir was also attempted but poorly tolerated. The patient was later treated with intravenous zanamivir, through an emergency Investigation New Drug, and ribavirin was also added. The patient's course was further complicated by neutropenic fever, and secondary bacterial pneumonia and she remained symptomatic at the time of the report.
The rapid selection for H274Y resistance mutation are exemplified by another report of two cases of HCT patients who developed rapid oseltamivir and peramivir resistance after becoming infected with the 2009H1N1. 48 The first patient developed respiratory symptoms and was treated for 30 days with antivirals. Sequence analysis revealed the presence of the H274Y mutation by day 9 post-treatment. A second patient developed mild upper respiratory symptoms and was treated with oseltamivir. Despite 24 days of continuous oseltamivir and 10 days of peramivir I V, the patient developed respiratory distress and bronchoscopy at the time revealed the presence of Influenza. The patient then received 10 days of inhaled zanamivir and had symptomatic improvement. Selection for the H274Y mutation had occurred by day 14 post-treatment in this patient.
Immunocompromised patients have been reported to develop cross resistance to other NAI's. In a case report, Influenza was confirmed by PCR and the patient was started on oseltamavir. 49 The H274Y mutation was detected 12 days after treatment had begun and the patient was switched to intravenous zanamivir. The viral load decreased following this treatment, and the patient was discharged home. However, the patient returned approximately 3 weeks later with lower respiratory symptoms and IV zanamivir was re-initiated. Because the virus persisted additional analysis was performed and by day 55 a new mutation, (I223R), was detected. These isolates exhibited decreased sensitivity to oseltamivir, zanamivir, and peramivir. This patient's respiratory status worsened, eventually leading to death. This patient illustrates the selection of multidrug resistance to all available NAI's such as oseltamivir, zanamivir, and peramivir in a transplant patient.
Similarly a report by Renuad et al illustrates the problems of cross resistance after treatment for 2009H1N1 in a HCT. 50 The patient was initially placed empirically on oseltamivir. His respiratory status declined and the broncho-alveloar lavage fluid revealed a high viral load for 2009H1N1. On day 6, a PCR showed >90% wild type virus at position 274Y. On day 7 the patient was switched to IV peramivir. On day 14 the patient developed hallucinations and one dose was held, because of the concern of the drug contributing to the psychiatric symptoms. The patient again developed respiratory distress requiring intubation and peramivir was re-started on day 16. On day 17, because of continued viral shedding, peramivir was discontinued and testing for H274Y was performed and confirmed by PCR. Thus this mutation emerged during the treatment course with peramivir. The patient was started empirically on oseltamivir, oral ribavirin, and rimantidine, pending emergency approval of IV zanamivir. On day 19, combination therapy was discontinued and the patient was started on IV zanamivir. His respiratory status continued to decline and the patient required inhaled nitrous oxide for hypoxia despite ventilator support. The clinical course included the development of ileus, cardiac arrhythmias, and he died on day 28. This case illustrates the concern that resistance to newer NAI's such as peramivir, can also be selected for in the transplant population.
As patients shedd virus, a major concern is transmission of resistant virus which has been described in immunocompromised patients. A recent report described 11 cases of 2009H1N1 in transplant patients, ten of which were shown to be related by genetic analysis of the HA and NA genes. 51 Eight of ten of these cases had H274Y mutation. Four of eight of the patients were infected by direct transmission of resistant virus. Fortunately all of these patients recovered with antiviral treatment. Thus, resistant virus can be transmitted even in the hospital setting after transplants.
Investigational or Limited Approved Treatments for Influenza (Table 1)
T705 or Favipiravir (Toyama Chemical) is an investigational antiviral drug that inhibits influenza virus RNA polymerase (PB1, PB2, and PA). 52 Preclinical studies by Itoh and colleagues suggest that favipiravir is active against 2009H1N1 strains both in vitro and in vivo. 53
Recent studies demonstrated that favipiravir was effective against oseltamivir drug resistant seasonal as well as oseltamivir resistant pandemic viruses in vitro.54,55 In addition, ths drug has shown potent activity against H5N1 in vivo. 56 Favipiravir, either alone or in combination with licensed NAIs, is being investigated in phase two clinical studies for the treatment of influenza. There are currently no reports of the use of favipiravir in immunocompromised patients.
Laninamivir (CS-8958) is a long acting NAI. In phase three trials a single inhaled dose of laninamivir was shown to be as effective as five-day dosing of oseltamivir in terms of time to symptom resolution. 57 This drug has shown in-vitro activity against 2009H1N1. 54 This drug has received marketing approval in Japan. Currently there are no case reports of the use of this drug in immunocompromised patients.
Peramivir (Biocyst Pharmaceuticals) is a NAI under development for the treatment and prevention of influenza. Early studies against human challenge virus using an oral peramivir showed some beneficial treatment effects on viral shedd for both influenza A and B viruses but failed to demonstrate effects as a prophylaxis, due to low peramivir concentrations with the oral form. 58 Further development of this antiviral drug focused on either an intramuscular formulation or an IV formulation. A 344 patient treatment study of the intramuscular formulation of peramivir in the treatment of acute influenza failed to show significant decreases in time to alleviation of symptoms compared to placebo. 59 A second study of this same intramuscular formulation in 405 subjects with acute influenza also failed to show significant decreases in the median time to alleviation of symptoms.60,61 In contrast, the IV formulations of peramivir have shown activity for treatment of influenza in certain populations. For example, in a study of 137 hospitalized patients IV peramivir showed activity defined as time to clinical stability, with activity comparable to oral oseltamivir. 62 In a phase 3 study of IV peramivir in 1099 subjects with acute influenza, non-inferiority to oseltamivir was demonstrated with regard to time to alleviation of symptoms. 63
In general, viruses that contain the H274Y mutation for oseltamivir are less sensitive to peramivir as well. For example, in a study of clinical isolates from Southeast Asia and Africa wherein 64% of H1N1 isolates had the H274Y mutation, this mutation resulted in an average reduction of sensitivity to oseltamivir and peramivir of 1466-fold and 527-fold respectively. 64
In the initial clinical isolates of 2009H1N1 pandemic, all cases were sensitive to NAIs including peramivir while they were consistently resistant to the adamantanes. 54 In summary, IV peramivir may have significant utility for hospitalized patients during current and future pandemics. However, its large scale use may be limited as the IM form has shown less activity.
On October 23, 2009 the FDA granted peramivir an EUA for IV administration for the treatment of certain adult and pediatric patients with 2009H1N1 pandemic.65,66 This drug has received marketing approval in Korea and Japan. 67
DAS181 (FludaseTM, NexBio Inc.) is a sialidase catalytic domain/amphiregulin glycosaminoglycan (GAG) binding sequence fusion protein. 68 It is a recombinant fusion protein composed of a sialidase and a cationic sequence tag on the C-terminus. This drug selectively cleaves sialic acids from host cells, thereby rendering them inaccessible to IFV, which require sialic acids as receptors. Given that it is directed towards the sialic acid receptors on the host airway epithelium, it also prevents the binding of other respiratory viruses which utilize this receptor, such as Parainfluenza Virus.
DAS181 has in vitro and in vivo preclinical activity against numerous seasonal IFV strains as well as highly pathogenic avian influenza strains (H5N1). 69 It has recently been demonstrated to have activity against viral clinical isolates with the H274Y mutation. 70 DAS181 has also shown activity in vitro, in vivo, and ex vivo against the 2009H1N1 pandemic strains. 71 A recent double blind placebo controlled study of 177 influenza infected otherwise healthy subjects documented a significantly shorter duration of viral shedding in subjects treated for three days with DAS181 compared to control subjects. 72
In summary, the treatment and prevention of influenza infection presents major challenges, which are exemplified by the recent 2009H1N1 pandemic. Selection for antiviral resistance mutations occur over time. Prolonged virus shedding and selection for resistance mutations and cross resistance can be exacerbated in immuncompromised patients. In addition to 2009H1N1, recent concerns have been raised regarding the ability of avian influenza (H5N1) mutations that can result in transmission between mammals. 73 As influenza continues to be a major public health concern, these challenges make influenza an important area for the development of new vaccine and antiviral approaches.
Author Contributions
Conceived and designed the experiments: RBM. Analysed the data: RBM. Wrote the first draft of the manuscript: RBM. Contributed to the writing of the manuscript: RBM. Agree with manuscript results and conclusions: RBM. Jointly developed the structure and arguments for the paper: RBM. Made critical revisions and approved final version: RBM. All authors reviewed and approved of the final manuscript.
Footnotes
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.
Dr. Moss is an employee of NexBio Inc.