
Abstract
Background
Chronic hepatitis C virus (HCV) infection is not a simple viral infection; it has many metabolic and autoimmune complications.
Objective
To investigate the impacts of chronic HCV infection on glucose and lipid metabolism and its correlation-if any-with body mass index (BMI) and hepatosteatosis in chronic HCV patients.
Patients and Methods
One hundred and three (103) chronic HCV patients were involved in this study. After blood sugar testing patients were classified into three groups; Group I: 68 chronic HCV patients with type 2 diabetes. Group II: 35 chronic HCV patients without Type 2 Diabetes and Group III: 25 patients with Type 2 Diabetes as a control group. With informed written consents and approval from Ain Shams medical ethics committee, all groups were subjected to the following: full history taking, thorough clinical examination, calculation of BMI, and measurement of the waist/hip ratio were done. Assessment of fasting plasma insulin level was done by the immune-enzymatic method. Assessment of the insulin resistance state was done by Homeostatic Model Assessment (HOMA-IR).
Detection of anti-HCV was done by the 3rd generation ELISA test and confirmed by qualitative polymerase chain reaction (PCR).
Results
Diabetic and non diabetic chronic HCV patients were found to have significantly higher fasting plasma insulin levels and insulin resistance states than the control group. This insulin resistance was not due to increased body mass index as there was a non significant difference in BMI between all the studied groups. Positive correlations were found between plasma insulin level, liver enzymes and steatohepatitis in HCV patients whether they were diabetic or not. No correlation was found between BMI and plasma insulin level in group II patients (HCV only).
Conclusion
Chronic HCV infection may be regarded as an independent risk factor for the development of insulin resistance and type 2 diabetes. HCV induces insulin resistance; the key step for glucose intolerance, and virus C induced steatohepatitis therefore leading to faster progression to cirrhosis. The impacts of chronic HCV infection on glucose and lipid metabolism should be recognized in clinical care centers and addressed in future studies.
Introduction
An epidemiological link has been established between chronic HCV infection and Type 2 Diabetes. The incidence of Type 2 Diabetes among chronic HCV patients was significantly higher than that in general population; (50% versus 14.5%) respectively. 1 The development of progressive insulin resistance impaired fasting glucose and/or frank Type 2 Diabetes (IFG/DM) was higher in chronic HCV patients than in general population. 2 It was postulated that, the presence of HCV core RNA in the circulation; triggers a multistep vicious cycle of metabolic derangement starting with a decreased expression of hepatic insulin receptor substrates 1 and 2 (IRS1 and IRS2) on hepatocytes leading to progressive insulin resistance and impaired glucose tolerance. 3 Kawaguchi et al 4 have found that, HCV directly causes insulin resistance through HCV core protein elicited proteasomal degradation of insulin receptor substrates and subsequent inactivation of intracellular insulin signaling molecules such as AKT. Additionally, tumor necrosis factor α and/or triglyceride accumulation induced nuclear factor-Kabba B activation in the liver is shown to play a role in insulin resistance in chronic HCV patients.
These changes are specific for chronic HCV infection and are not associated with infection by other hepatic viruses (HBV), suggesting an HCV induced intrinsic defect in hepatocytes independent from liver injury or autoimmunity. 5
In 2001, Cimino et al 6 described the interactions between chronic HCV infection, insulin resistance, Type 2 Diabetes and hepatosteatosis as a metabolic syndrome observed in chronic HCV patients. The progress of hepatic damage; (steatosis/fibrosis) scores was inversely proportional to plasma cholesterol levels and directly proportional to plasma insulin levels. Fibrosis is the hallmark of hepatic cirrhosis, of which worsening is probably the best surrogate marker for progression of chronic liver disease in chronic HCV patients. 7 Douglas and George (2009) 8 reported that; insulin resistance (IR) is most strongly associated with HCV infection, and its faster progression to fibrosis and cirrhosis in chronic HCV patients that may culminate in liver cell failure and hepatocellular carcinoma.
HCV is responsible for approximately 50% of hepatosteatosis cases. 9 Additionally, chronic HCV infection has an impact on lipid metabolism; lipoatrophy, peripheral (limb) wasting, increase hepatic handling and storage of fats. Lack of insulin sensitivity and an insulin resistance state activate hormone dependant lipase; with excessive mobilization of peripheral fats to the liver and hepatosteatosis. Characteristically, these patients have low plasma cholesterol and triglyceride levels.10–11
The aim of the study was to investigate the impacts of HCV infection on glucose and lipid metabolism and its correlation—if any- with body mass index (BMI) and hepatosteatosis in chronic HCV patients with and without Type 2 Diabetes.
Patients and Methods
One hundred and three (103) chronic HCV patients were enrolled—none consecutively—in a retrospective observational study. They were either inpatients in the internal medicine department or were regularly attending HCV specialized out patients clinic, at Ain Shams University Hospital, in the period between January 2006 to September 2007.
Full history taking, thorough clinical examination, routine laboratory investigations including complete liver function tests and abdominal U/S were performed on all patients. Obese patients, patients with other concomitant viral infections (HBV), alcoholics, autoimmune hepatitis, hepatorenal syndrome and patients with hepatic focal lesions were all excluded from the study. Informed written consent were obtained from all participants and the study was approved by Ain Shams University Hospitals medical ethics committee (FMASU REC). HCV infection was diagnosed by the detection of anti-HCV antibody using the 3rd generation ELISA test and confirmed by qualitative polymerase chain reaction (PCR). After blood sugar testing; Type 2 Diabetes was diagnosed according to the working definition of the WHO criteria of Type 2 Diabetes [fasting blood sugar ≥126 mg%]. Chronic HCV patients were classified into two groups:
All patients were subjected to the following: Full history taking and thorough clinical examination, calculation of body mass index (BMI): weight (kgm)/ height (m2), measurement of waist/hip ratio as an index of visceral obesity; an independent risk factor for hepatosteatosis and insulin resistance, 13 BMI: 18.5–24.9 kg/m2 normal, 25–29 over weight, ≥30 obese. Obesity was classified as the following; class I: 30–34.9 kgm/m2, class II: 35–39.9, class III ≥40 kg/m2,12 Assessment of the insulin resistance state was done to all patients using the Homeostatic Model Assessment (HOMA-IR): Fasting plasma insulin (μIU/ml) × fasting glucose (mmol/ml)/22.5. 14 Pelvic abdominal ultrasonography (U/S) was performed on all patients after an overnight fast and with the usual preparations. Aloka 3.5 Mega Hertz curved probe was used to examine; liver size, parenchymal echogenisity, enhancement, portal vein caliber and the billiary system.
Laboratory Investigations
Seven ml of venous blood was withdrawn from each patient after an overnight fast. Three ml was taken on EDTA for complete blood count (CBC) using an automated cell counter (Advial120), erythrocyte sedimentation rate (ESR) by the Westergren method and HbA1C by the quantitative colouremetric determination of glycosylated Hb in whole blood using the Stanbio Kit (1261 Northmain Street. Boerne, Texas 78006. www.stanbio.com). Four ml was put in a sterile plain tube, blood was allowed to clot and serum was separated by centrifugation at 3000 rpm for 20 minutes and stored at -20 °C until used. Serum was used in the following investigations:
Using the automated chemistry analyzer Synchron Bechman Coulter CX9ALX CX5 Delta; Fasting and 2hr.pp serum glucose level.—Liver function tests: Alanine amino transferase (ALT), Aspartate amino transferase (AST), gamma glutamyle transpeptidase (γGT), Alkaline Phosphates (ALP).—Kidney function tests. Lipid profile. Anti-HCV antibodies were detected by 3rd generation ELISA Diasorin S.A kit (Alcopenges Madrid, Fax 39.0161.487628). HCV infection was confirmed by qualitative polymerase chain reaction (PCR) using the COBAS Amplicore HCV monitor test (Roche Diagnostic System Inc. branch burg, NG). Using the PCR amplified product; genotype was determined by INNO-LIPA HCVII (innogenetics N.V. technologies park 6. 9052 Ghent Belgium). The steps were followed according to the manufacture instructions and genotypes were deduced by using the INNO-LIPA HCVII interpretation chart. Fasting serum insulin level was assayed by immune-enzymatic method: using ELISA technique (MEDGENIX ins—ELISA).
Statistics
Analysis of data was done by an IBM computer using SPSS (statistical program for social science version 12). Description of quantitative variables as mean, SD and range. Unpaired t-test was used to compare the two groups as regards to quantitative variables in parametric data (SD < 50% mean). The Spearman correlation test was used to rank different variables against each other. A one way ANOVA test was used to compare more than two groups regarding quantitative variables in parametric data: (SD < 25% of the mean). P value > 0.05 is non significant (NS), p < 0.05 is significant (S), p < 0.001 is highly significant (HS).
Results
The results were statistically analyzed and presented in (5) tables and (4) figures.
Demographic data of the studied groups.
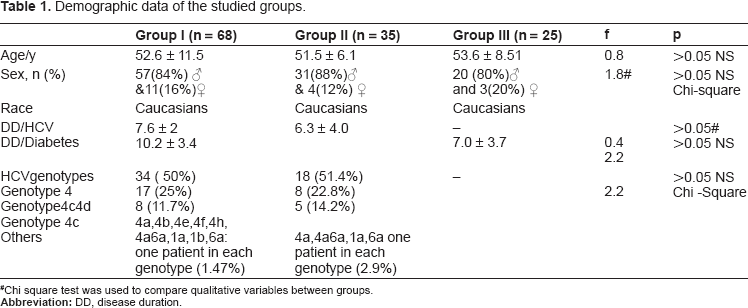
Chi square test was used to compare qualitative variables between groups.
Symptoms and signs of impaired liver functions in chronic HCV patients with (group 1) and without (group 2) Type 2 Diabetes.
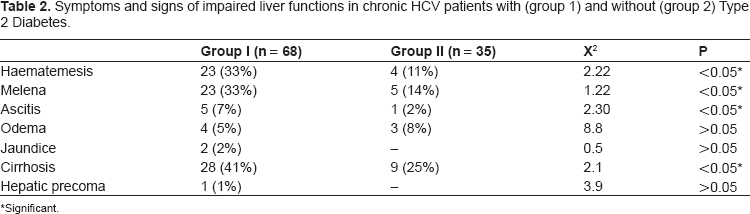
Significant.
Of the 68 patients in group I 37 (54%) and 35 patients in group II, 21 patients (60%) had previously undergone liver biopsies; to assess the degree of hepatic fibrosis/steatosis before interferon therapy; (for therapeutic purposes and not as a part of this research methodology).
Comparison between group I and group II (chronic HCV patients) regarding liver function tests and fibrosis/ steatosis scores.
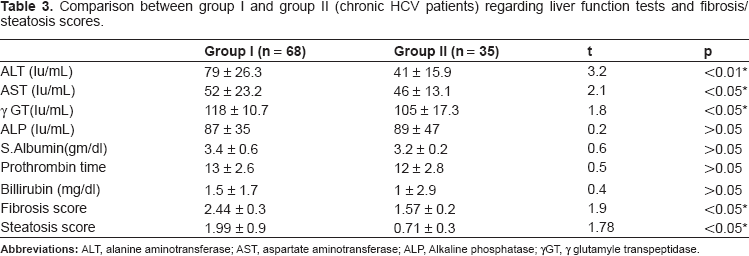
Liver enzymes (AST, ALT and γ GT) were significantly higher in diabetic chronic HCV patients than in non diabetic chronic HCV patients. However non-significant differences were found between the groups regarding synthetic liver functions.
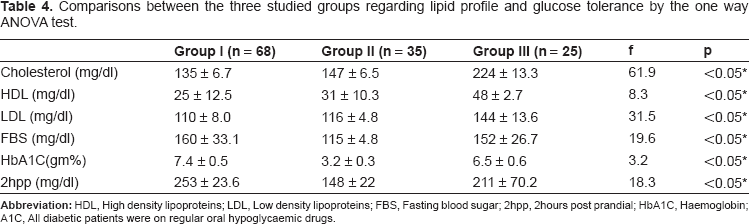
Comparisons between the three studied groups regarding lipid profile and glucose tolerance by the one way ANOVA test.
Comparison between the three groups in regards to BMI, waist/hip ratio, plasma insulin level and homeostatic model assessment of insulin resistance (HOMA-IR).
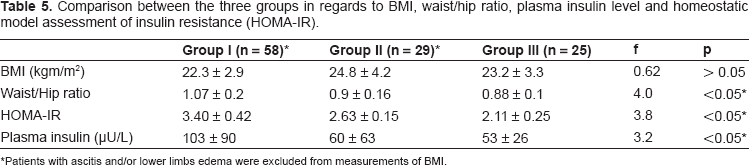
Patients with ascitis and/or lower limbs edema were excluded from measurements of BMI.
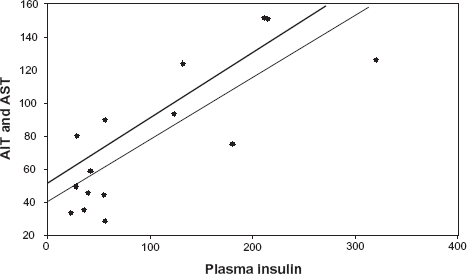
Correlation between plasma insulin level and liver enzymes in all chronic HCV patients.
Discussion
Recently, chronic HCV infection has been regarded as a metabolic syndrome rather than a simple viral infection. Metabolic complications were frequently observed in chronic HCV patients concerning glucose and lipid metabolism. 17 Both host and viral factors contribute to insulin resistance, glucose intolerance and steatohepatitis. Importantly, fibrosis progression is closely linked to the insulin resistance state and hepatic steatosis in chronic HCV patients. 18
Up to one third of chronic HCV patients develop Type 2 Diabetes. 19 In agreement with this statement, we have found that 66% of chronic HCV patients in the present study were found to have Type 2 Diabetes.
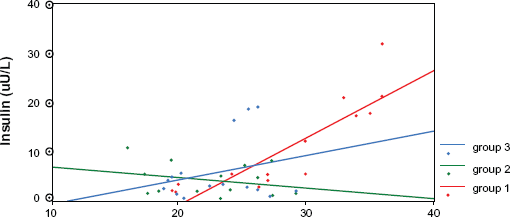
There were significantly higher plasma insulin levels, waist/hip ratio and insulin resistance states by HOMA-IR in chronic HCV patients whether they were diabetics or not than diabetic patients without HCV infection (controls). This insulin resistance state that presents, even in non diabetic chronic HCV patients, was not due to an increased BMI, as there was non-significant differences in BMI between all studied groups. Despite the presence of significant positive correlation between BMI and fasting plasma insulin level in groups I and III patients (diabetics with and without HCV infection), no correlation was found in group II patients (non diabetic chronic HCV patients), indicating a unique mechanism of insulin resistance and hyperinsulinaemia in chronic HCV patients other than an elevated BMI.
This finding is in agreement with Zein et al 1 and Kazuhiko Kokie 20 who concluded that the development of progressive insulin resistance measured by HOMA in chronic HCV patients is in dependent on the anthropometric markers of obesity. Thus it would appear that insulin resistance and hepatic steatosis frequently observed in chronic HCV patients were not simply secondary to obesity. In the same way Hickman et al 21 and Yoneda et al 22 have concluded that elevated plasma insulin level might be a factor responsible for the association between steatohepatitis and chronic HCV infection irrespective of the viral genotype.
The molecular mechanisms underlying HCV induced insulin resistance is complicated and not clearly understood. In 2008, Imazeki et al 23 refer this insulin resistance state simply to HCV induced autoimmunity, as they found 33% of chronic HCV patients have anti-insulin antibodies (AIA). These antibodies complicate the course of chronic HCV infection and are not present with any other viral hepatitis. While Kawaguchi et al 4 refer it directly to the HCV core protein that inactivates intracellular insulin signaling molecules such as AKT.
In the present study, retrospective analysis of the available liver biopsies reports revealed that diabetic chronic HCV patients have a more advanced histopathological grade of hepatic damage (steatosis/fibrosis scores) compared to non diabetic chronic HCV patients. Though, there was non-significant (p > 0.05) differences regarding HCV disease duration between both groups. Additionally, we have found significant positive correlations between plasma insulin level with liver enzymes and steatosis scores in chronic HCV patients (whether they were diabetic or not). The higher the plasma insulin level and insulin resistance state the more likely the elevated liver enzymes, and steatosis/fibrosis score -markers for hepatic damage in chronic HCV patients.
Median plasma insulin levels in the three studied groups. Correlation between plasma insulin level and BMI in all groups.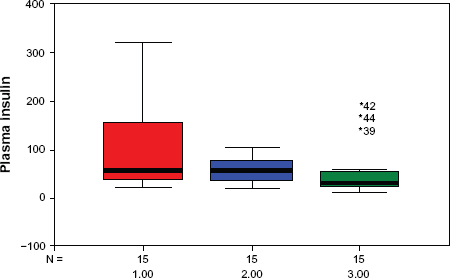
Our results were consistent with that of Moucari et al
24
who studied the association between insulin resistance, serum HCV RNA level and steatohepatitis scores in a large prospective cohort of chronic HCV patients. They concluded that insulin resistance and hyperinsulinaemia are specific features of chronic HCV infection, especially with genotypes 4 and 1 (the most prevalent types in Egypt) and it positively correlated with the degree of steatohepatitis in HCV patients. It is well known that steatohepatitis accelerates cirrhosis in chronic HCV patients. Similarly, Douglas and George
8
found that there was a positive correlation between steatosis scores and the progression of hepatic damage due to cirrhosis in chronic HCV patients. Steatosis worsened the course of hepatitis C with faster progression to cirrhosis and which may culminate in liver cell failure and hepatocellular carcinoma.
Correlation between plasma insulin level and hepatosteatosis.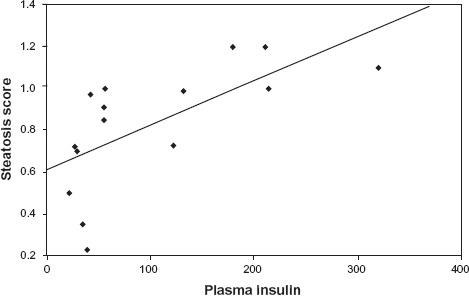
Similarly, Hora et al 25 concluded that insulin resistance and hyperinsulinaemia in HCV patients may aggravate virus C induced hepatic damage by up regulating hepatic stellate cells to produce connective tissue growth factor which plays a major role in extra cellular matrix protein production (fibrin) and progressive hepatic fibrosis. Therefore, it is of a vital importance to prevent and control diabetes, obesity, insulin resistance and hyperinsulinaemia in chronic HCV patients. Interestingly, Kattab et al 26 have found that; Pioglutazone (an insulin sensitizer) improves the virological response to peg interferon/ribavirin therapy in genotype 4 chronic HCV patients with insulin resistance.
In the present study, diabetic patients with chronic HCV infection have poorly controlled diabetes with higher FBS, 2hpp blood sugar and HBA1C levels than diabetic patients without HCV infection in spite of the fact that both groups of patients were on regular oral hypoglycemic drugs. The incidence of diabetic nephropathy and neuropathy was found to be significantly higher in diabetics with HCV infections than diabetic patients without HCV infection. Chronic HCV infection may negatively affect the diabetes course and prognosis. This is in agreement with Crook et al 27 who reported that hepatitis C viral infection is a predictor of poor renal outcomes in diabetic patients with chronic HCV infection.
There was significant hypocholesterolemia (LDL/HDL) in chronic HCV patients (with and without diabetes) compared to diabetic patients without HCV infection. The total cholesterol level was negatively correlated with plasma insulin levels and hepatosteatosis scores in chronic HCV patients. This was in keeping with the results of Lecube et al 10 and Liakina et al 11 as they found that lack of insulin sensitivity and insulin resistance state activates hormone dependant lipase; with excessive mobilization of peripheral fats to the liver and hepatosteatosis. Characteristically, these patients have low plasma cholesterol and triglyceride levels.
Importantly, in this study the incidence of liver cirrhosis was higher (41%) in diabetic chronic HCV than in non diabetic chronic HCV patients (25%). This agrees with the Lonardo et al 28 who investigated large numbers of chronic HCV patients in double blind cross sectional study; they concluded that, chronic HCV infection is associated with dysmetabolic syndrome impaired insulin signaling, insulin resistance, Type 2 Diabetes, steatohepatitis and impaired response to antiviral therapy. These metabolic derangements accelerate liver cirrhosis and hence increase the risk of hepatocellular carcinoma. They added that insulin resistance is the key step for the metabolic derangement that complicates the course of chronic HCV infection.
Conclusion and Recommendations
There appears to be an association between Type 2 Diabetes Mellitus and chronic HCV infection as both may aggravate each other. Chronic HCV infection may be regarded as an independent risk factor for Type 2 Diabetes. HCV infection induces a state of insulin resistance, hyperinsulinemia and glucose intolerance (independent of BMI), which in turn might accelerate virus C induced steatohepatitis and hence a progression to cirrhosis.
Dyslipidemia and hepatic steatosis were frequent complications in chronic HCV patients, whether they were obese or not. However, HCV patients with a higher BMI have an additional risk for aggressive hepatosteatosis and cirrhosis than those with normal BMI. The potential impacts of chronic HCV infection on glucose and lipid metabolism should be recognized in clinical care centers and addressed in future research studies. Chronic HCV patients should have a regular exercise program, diet, weight control and follow up to antagonize the insulin resistance state which is the key step of virus C induced diabetes, steatohepatitis and cirrhosis. HCV patients should have regular blood sugar testing and diabetic patients-in HCV endemic areas -should be screened for HCV infection.
Footnotes
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors report no conflicts of interest.