
Abstract
Background
This study assessed the antimicrobial susceptibilities and the presence of inducible macrolide–lincosamide–streptogramin B (iMLSB) resistance in methicillin-resistant Staphylococcus aureus (MRSA) of Jamaica as well as the relatedness using polymerase chain reaction-based staphylococcal cassette chromosome mec (SCCmec) and multiple-locus variable numbers of tandem repeat analyses (MLVAs).
Materials and Methods
Antimicrobial susceptibility, the presence of MLSB resistance, and SCCmec and MLVA patterns were assessed for 61 nonduplicate isolates of MRSA from hospitalized patients.
Results
While no isolate was resistant to vancomycin, 53 (86.9%) isolates were resistant to ciprofloxacin, 52 (85.3%) to erythromycin, 49 (80%) to lincomycin, and 45 (74%) to clindamycin. Of the 52 erythromycin-resistant isolates, 48% exhibited constitutive resistance and 8% showed inducible MLSB (iMLSB) resistance. Most (85%) of typable isolates were SCCmec type IV, and among these, 16 MLVA patterns were identified.
Conclusion
Multidrug resistance continues to characterize MRSA. Among the erythromycin-resistant isolates, constitutive resistance and iMLSB resistance are common. These facts will complicate the treatment of MRSA infections and warrant continued surveillance and judicial use of antimicrobial agents.
Keywords
Introduction
Methicillin-resistant Staphylococcus aureus (MRSA) is a major cause of hospital-acquired (HA) infections and has established itself as a significant community-acquired pathogen.1,2 In most if not all cases, invasive infections because of MRSA are associated with significant morbidity and mortality and high costs to the healthcare system. 3 Community-associated MRSA (CA-MRSA) is usually caused by emerging strains unlike those responsible for HA infections and can cause infections in otherwise healthy persons with no links to healthcare systems or no known risk factors for MRSA colonization. 4 CA-MRSA is occurring with increasing frequency and tends to occur in conditions where people are in close physical contact, such as athletes involved in football and wrestling, soldiers kept in close quarters, inmates, childcare workers, and residents of long-term care facilities. 5 7 CA-MRSA differs from HA-MRSA in that it does not generally belong to the major clonal groups of epidemic MRSA, it is susceptible to most non-β-lactam antibiotics, it contains the type IV, V, or VI staphylococcal cassette chromosome mec (SCCmec) element, and it frequently contains genes for Panton-Valentine leukocidin. 8 11 In the main English-speaking Caribbean islands (Jamaica and Trinidad and Tobago) and Puerto Rico, it has been shown that the prevalence of methicillin resistance in S. aureus is increasing. 12 15 Further, Chroboczek et al 16 noted that the distribution of the major MRSA clones in these islands was different, and clones most closely resemble those circulating within the home countries of frequent tourist travelers.
Macrolide antibiotic resistance in S. aureus may be because of three factors: (1) cells harboring the linA gene that inactivates both lincomycin and clindamycin but resists high levels of lincomycin alone (L resistance), (2) an active efflux mechanism encoded by msrA (that confers resistance to macrolides and type B streptogramins only, ie, macrolide–streptogramin (MS) resistance), and (3) ribosomal target modification that affects macrolide–lincosamide–streptogramin B (MLSB) resistance. Strains with inducible MLSB (iMLSB) resistance demonstrate in vitro resistance to 14- and 15-member macrolides (eg, erythromycin), while appearing susceptible to 16-member macrolides, lincosamides, and type B streptogramins. On the other hand, strains with constitutive MLSB resistance show in vitro resistance to all of these agents.17,18
Advances in molecular typing have been achieved by analysis of variable numbers of tandem repeat (VNTR) loci identified in the genomes of eukaryotic and prokaryotic species during genome sequencing projects. The number of repeat units at the same locus varies from strain to strain and can be detected by polymerase chain reaction (PCR) with flanking primers. The sequencing of the S. aureus genome indicated the presence of several VNTR loci, including sdr, clfA, clfB, sspA, and spa. 19 Given that there is so much genetic variability in MRSA regionally and so little information available in Jamaica, the aims of this study were to: (1) determine the antimicrobial susceptibility patterns of isolates of MRSA submitted by patients admitted to public hospitals in the Kingston and St. Andrew metropolis in Jamaica, (2) determine if iMLSB resistance is present in MRSA resistant to erythromycin, (3) group isolates using PCR-restriction fragment length polymorphism analysis of the SCCmec element, and (4) discriminate among isolates based on the multiple-locus VNTR analysis (MLVA) of five (sdr, clfA, clfB, ssp, and spa) tandem repeat loci.
Materials and Methods
Isolates and Antibiotic Susceptibility Testing
Sixty-one nonduplicate isolates of MRSA were submitted by patients admitted to public hospitals in Kingston and St. Andrew, Jamaica (excluding the University Hospital of the West Indies (UHWI)). These public hospitals included two adult hospitals (over 750 beds) and a children's hospital (283 beds), and they are served mainly by the government-run public health laboratory system. More than half of the patients admitted to the adult hospitals are from the surrounding inner city communities. The UHWI was excluded as several studies have been reported from that institution, and there is a robust infection control program in place. Patients were seen on the pediatric, medical, and surgical wards, and isolates were obtained between September 2011 and August 2012. It is unclear whether patients were treated with antibiotics prior to sample isolation. Isolates were recovered from wounds, sputum, midstream urine and catheter tip, ear and nasal swabs, and a knee aspirate, identified as S. aureus by standard biochemical techniques, and subsequently confirmed as MRSA by disc susceptibility results with 1 g oxacillin or by growth on plates containing oxacillin. Antimicrobial susceptibility tests were carried out on Müeller-Hinton agar using the disc diffusion technique as per the Clinical and Laboratory Standards Institute guidelines 20 and using gentamicin (10 μg), rifampicin (30 μg), trimethoprim/sulfamethoxazole (SXT) (1.25/23.75 μg), ciprofloxacin (5 μg), teicoplanin (30 μg), vancomycin (30 μg), lincomycin (2 μg), clindamycin (2 μg), erythromycin (15 μg), mupirocin (5 and 200 μg), linezolid (30 μg), chloramphenicol (30 μg), quinupristin–dalfopristin (15 μg), and tetracycline (30 μg). All isolates were first tested with the 5 μg mupirocin disc to determine low-level resistance (LLR). High-level resistance (HLR) was confirmed in isolates resistant to 5 μg mupirocin using 200 μg mupirocin discs.
Disc Induction Testing
The determination of the presence of iMLSB resistance in MRSA to erythromycin was carried out according to Novotna et al. 18 Essentially, lincomycin, clindamycin, and quinupristin–dalfopristin discs were placed at the sides of an erythromycin disc, about 15 mm apart, and then the plates were incubated for 16–18 hours.
SCCmec and MLVA of MRSA Strains
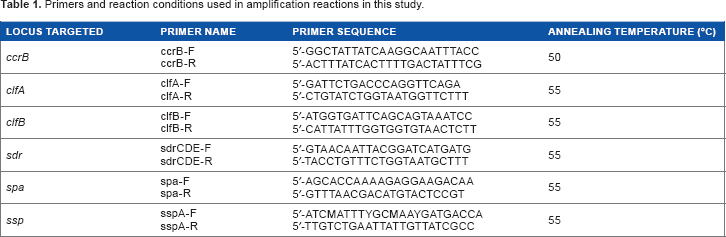
SCCmec analysis was carried out on chromosomal DNA extracted from the strains according to the scheme proposed by Yang et al, 21 using the ccrB forward and reverse primers (Table 1) and appropriate controls. Subsequently, PCR products were digested with HinfI and BsmI (New England Biolabs) at 37°C for three hours, and then the digested products were analyzed by 1% agarose gel electrophoresis. MLVA analysis was determined based on the scheme proposed by Sabat et al 19 using a set of PCR primers to simultaneously amplify the hypervariable VNTR regions of the spa, sspA, clfA, clfB, and sdrCDE genes (Table 1). PCR products were analyzed by 2% agarose gel electrophoresis, and a 100 bp DNA ladder was included in each run as a DNA size marker. Any two MLVA patterns differing by one or more bands were considered distinct types.
Primers and reaction conditions used in amplification reactions in this study.
Results
Antimicrobial Susceptibility Testing
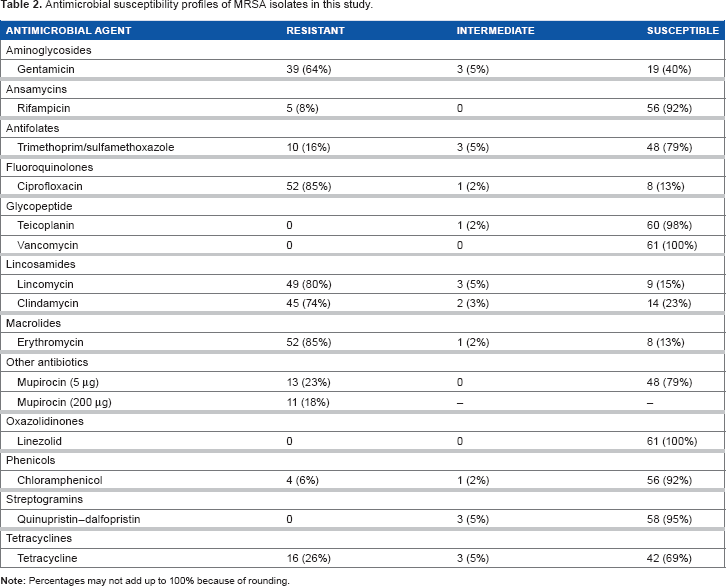
The number and percentages of MRSA isolates resistant and susceptible to antimicrobial agents are presented in Table 2. While no isolate was resistant to vancomycin, 53 (86.9%) isolates were resistant to ciprofloxacin, 52 (85.3%) to erythromycin, 49 (80%) to lincomycin, 45 (74%) to clindamycin, and 39 (64%) to gentamicin. Furthermore, five (8%) isolates were resistant to rifampicin. Thirteen (23%) isolates showed LLR to mupirocin; 11 (85%) of these 13 isolates (18% of the 61 isolates) showed high-level mupirocin resistance. High-level mupirocin resistance was observed in two isolates recovered from nose swabs.
Antimicrobial susceptibility profiles of MRSA isolates in this study.
Eleven isolates showed multiple resistance to seven or more antibiotics. These isolates showed complete resistance to lincomycin, and 91% and 82% of isolates were resistant to erythromycin and clindamycin, respectively. Almost all (28 of 30) isolates that showed multiple resistance to five antibiotics were resistant to the same antibiotics (lincomycin, gentamicin, ciprofloxacin, erythromycin, and clindamycin). The other two isolates showed resistance to mupirocin, tetracycline, and trimethoprim/SXT.
Disc Induction Testing
Of the 52 erythromycin-resistant isolates, full cross-resistance occurred in only 3 (6%) isolates. Even in the presence of erythromycin (an inducer), 50 (96%) of these isolates were susceptible to at least one MLSB antibiotic (Fig. 1); in all cases, the isolates were susceptible to quinupristin–dalfopristin. The most common type was the ELC phenotype (ie, resistance to erythromycin, lincomycin, and clindamycin). The constitutive macrolide–lincosamide–streptogramin (MLS) resistance mechanism was evident in 25 (48%) isolates, MS resistance mechanism in 24 (46%) isolates, and inducible MLS resistance mechanism in 4 (8%) isolates.
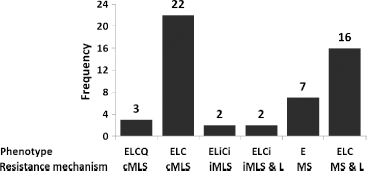
Phenotypes identified by a triple-disc induction test in erythromycin-resistant strains in this study.
SCCmec analysis
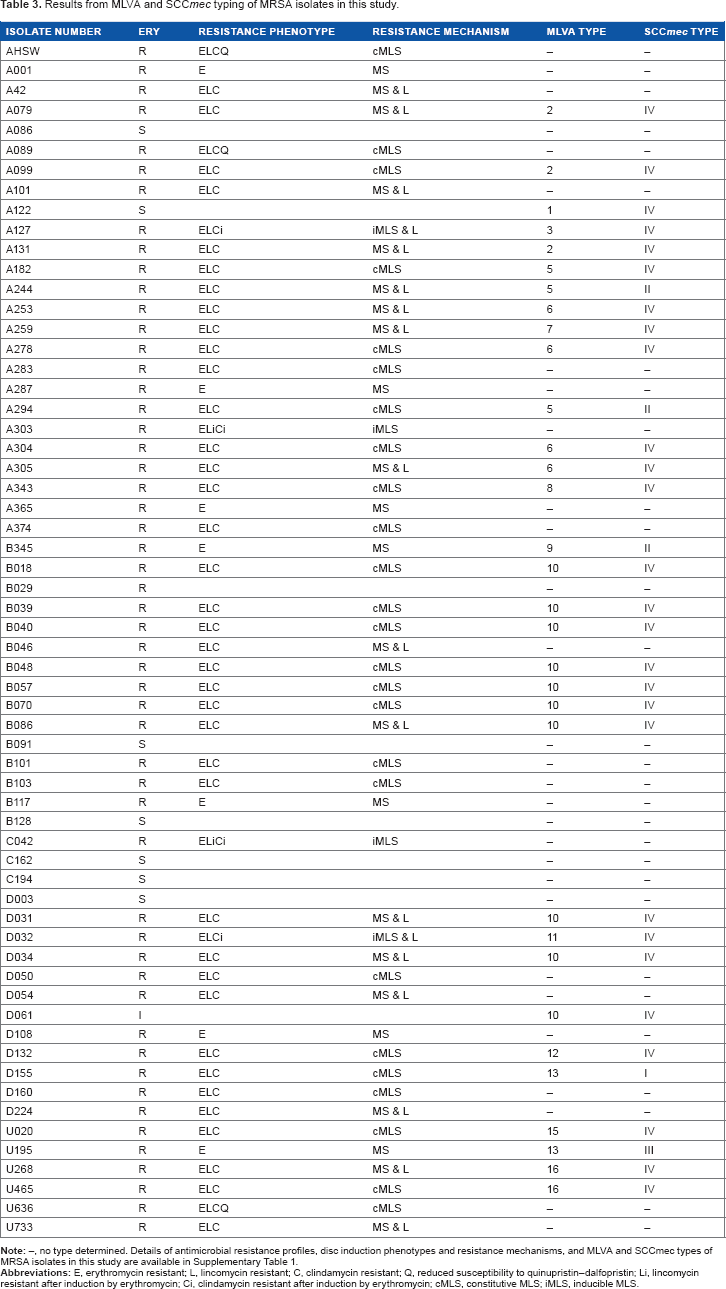
SCCmec typing confirmed a type in only 34 isolates. Analysis yielded 29 (85%) isolates as SCCmec type IV, 3 (9%) as type II, and 1 each (3%) as type I and type III, respectively (Table 3).
Results from MLVA and SCCmec typing of MRSA isolates in this study.
Multigene Analysis (Genetic Typing) of MRSA
Results were obtained for the 34 isolates that yielded an SCCmec type. Sixteen MLVA patterns were identified based on the scheme proposed by Sabat et al. 19 MLVA pattern 10 (with 12 isolates) was the most common, followed by patterns 6 (4 isolates) and 2 and 5 (3 isolates each). Six isolates were unrelated based on MLVA patterns (Table 3). Of the isolates that showed identical MLVA patterns, all isolates with patterns 2, 6, 10, and 16 had the same SCCmec type (type IV).
Discussion
S. aureus, and in particular MRSA, has long been one of the more serious and problematic nosocomial pathogens, repeatedly responding to the challenge of staphylococcal antibiotics by acquiring new resistance. In fact, its prevalence has increased globally, and it is clear that there are major differences in prevalence between countries and regions. In Jamaica, prevalence studies have largely been centered around the UHWI, the main teaching hospital in Kingston. However, this study sought to assess the characteristics of isolates outside of this controlled zone, where less stringent infection control is practiced.
In light of this, the highest overall susceptibility rates were observed for the glycopeptides and oxazolidinones (100% susceptible), followed by the susceptibility to ansamycins, phenicols, and streptogramins (93–95%). While parenteral glycopeptides remain the forefront treatment for systemic MRSA infections, not all of these infections have poor prognosis, and oral agents might be indicated, particularly when long-term therapy is required. 22 For example, rifampicin and trimethoprim–SXT, with demonstrable better tissue penetration than the glycopeptides, might be better suited oral agents 22 and, as shown in this study, had good coverage rates against MRSA. On the other hand, the highest resistance rates were observed against fluoroquinolones and macrolides, as reported elsewhere. 23 25 It is worth noting that fluoroquinolones select for methicillin resistance in staphylococci and with a 75% resistance rate, as seen in this study, suggest that these drugs can no longer be used in empirical therapy against MRSA infections.
As expected, no resistance was observed against either teicoplanin or linezolid; however, the one intermediate (reduced susceptibility) phenotype to teicoplanin and the three intermediate phenotypes to quinupristin–dalfopristin are of some concern as none of these drugs are used locally in Jamaica. However, the findings for linezolid are in concern with the results from other studies reviewed by Beibei et al, 26 which indicated that linezolid has excellent success rates against MRSA in randomized control studies. While the authors noted that there was no difference in total adverse effects related to the use of linezolid versus vancomycin and vancomycin tended to result in more nephrotoxicity, there was superior clinical and microbiological outcomes with linezolid in S. aureus infections.
With a low resistance rate of 6%, chloramphenicol shows similar results to other studies: 10%, 13 5%, 27 10.7%, and 4.9% resistance. 28 Result for rifampicin, with a resistance rate of 7%, is at the lower end when compared to other reports (3%, 29 18%, 22 and 53% 30 ), although higher resistance rates of rifampicin resistance in MRSA might be attributable to the treatment of tuberculosis.31,32 Trimethoprim/SXT and tetracycline had resistance rates of 14% and 23%, respectively. The relatively low resistance of SXT of 16.4% 33 and high susceptibility rates of 82.1% and 80.6% 28 are comparable to the results from this study.
Gentamicin, lincomycin, and erythromycin had relatively high resistance rates of 56%, 71%, and 77%, respectively. These values are of concern, especially for lincomycin, as it is a relatively new drug that should show increased effectiveness against MRSA. There is concern of the 65% resistance rate for clindamycin, as it has been proven to be an effective drug in treating S. aureus infections. It is well established that inducible clindamycin resistance can decrease its therapeutic efficacy.34,35
In terms of mupirocin resistance, we found a 23% LLR and 18% HLR compared to 30% LLR and 24% HLR reported by Nicholson et al 36 at the UHWI, Jamaica. These figures are high when compared to reports in the literature of 1–13% LLR and 2.4–14% HLR. 37 However, the rates at the UHWI are lower than those in Trinidad and Tobago, with 44% LLR and 26% HLR. 38 These data are worrying as mupirocin, a topical agent, is widely used in the management of infection and colonization by MRSA, and the inability to effectively clear the nasal colonization of S. aureus will undoubtedly increase the subsequent risk of development of infection by MRSA, in addition to increasing the spread of these pathogens. 39 Interestingly, McNeil et al 40 noted a 14.7% mupirocin resistance rate among S. aureus isolates from pediatric patients and that the genetic determinant was more significantly associated with methicillin-susceptible S. aureus (MSSA) than with MRSA.
There have also been a number of reported clindamycin and lincomycin treatment failures in S. aureus infections with iMLSB resistance.34,35 This brings into focus the efficacy of clindamycin use in infections caused by erythromycin-resistant S. aureus. Published data indicate that there is significant variability in iMLSB resistance among erythromycin-resistant S. aureus isolates and could be related to geographical location, hospital environment, patient age, and clinical samples examined. 41 In discussing their finding of 12% inducible resistance, the authors noted that such resistance varied from a low of 11% in Brazil to a high of 35% in India. Of note was the observation that this phenomenon was reduced in MSSA but was more prevalent in coagulase-negative staphylococci. The results of this study appear to be at the lower end of the spectrum as only 8% of erythromycin-resistant MRSA isolates showed iMLSB resistance. On the other hand, a number of erythromycin-resistant S. aureus isolates may show true clindamycin susceptibility. Of 52 erythromycin-resistant MRSA isolates obtained, 8 (15%) were clindamycin susceptible, with no indication of inducible resistance. Therefore, the assumption of clindamycin resistance based on actual confirmation of erythromycin resistance and the elimination of clindamycin as a potential therapeutic agent for erythromycin-resistant MRSA infections is problematic.
However, while clindamycin remains useful in the treatment of skin and soft-tissue infections and serious infections caused by S. aureus and MRSA, accurate susceptibility data are important for appropriate treatment decisions. This is because of the fact that susceptibility testing for clindamycin may indicate false susceptibility by the disc diffusion testing with erythromycin and clindamycin discs in nonadjacent positions. If inducible resistance can be reliably detected in clinical isolates, clindamycin can be safely and effectively used in the patients with true clindamycin-susceptible strains. 17
An important finding was the high proportion of type IV CA-MRSA among these apparent nosocomial isolates. This could indicate the emergence of a new MRSA lineage in Jamaica, with particular fitness for spread in the community. 42 It is clear that particular attention should be paid to the early detection of CA-MRSA strains in hospitals because of the potential for easy transmission of the type IV SCCmec element to nosocomial MRSA isolates. The determinants for resistance to multiple antibiotics carried by the types of SCCmec elements (types I, II, and III) may be suited for the survival of HA-MRSA, where various antibiotics provide selective pressure, but their large sizes and potentially hazardous arrays of exogenous genes may not be suited to MRSA strains in the community, where selective advantage would make strains more inclined to have a higher growth rate and to be better able to colonize humans than to have a multidrug resistance phenotype. 43 From this viewpoint, the type IV SCCmec may be one of the fitter SCCmec types that can give β-lactam resistance to community strains of MRSA without compromising their competitiveness among human and other vertebrate hosts. Consequently, the ability of type IV isolates to survive in the hospital setting increases the challenges for control and treatment. However, in this study, we noted that only some of the MRSA isolates produced an SCCmec genotype, having the mecA gene and high minimal inhibitory concentration values against oxacillin. In these isolates without the mecA element, alternate resistance mechanisms, such as overexpressing β-lactamase or altered penicillin-binding proteins (PBPs), could account for this resistance, 44 with or without the concomitant loss of the mecA gene.45,46 However, it is possible, albeit remotely, that the new mecC element 47 could be involved.
The eight sets of isolates that showed identical MLVA patterns (same set of bands) proved to be genetically identical; the remaining isolates were unrelated, as they showed a different profile. Furthermore, it was noted that the genetically identical isolates displayed the same SCCmec type. An important factor of MLVA is the differentiation power, defined as the ability to clearly differentiate among unrelated isolates and simultaneously demonstrate the relationship of organisms isolated from individuals infected through the same source. This criterion was fulfilled by MLVA as a typing system as all 18 distinct strains in this study were clearly discriminated. On the other hand, epidemiologically linked, and therefore genetically related, MRSA isolates showed little variation of repeat units. However, an inherent weakness of DNA-based typing methods, which rely on DNA fragment amplification, may fail to type some strains because of differences in the DNA sequence to which primers anneal. 19 This could account for some of the isolates not giving a band.
In conclusion, it is apparent that both HA-MRSA and CA-MRSA are coexisting among hospitalized patients in Jamaica. While some of these isolates are already showing reduced susceptibility to antimicrobial agents not yet licensed for use in Jamaica, many (erythromycin-resistant isolates) display constitutive and iMLSB resistance. These facts will complicate the treatment of MRSA infections. Hence, continued surveillance and judicial use of antimicrobial agents are warranted.
Author Contributions
PDB conceived and designed the experiments, analyzed the data, wrote the first draft of the manuscript, contributed to the writing of the manuscript, including the results and conclusions, developed the structure and arguments for the paper, made critical revisions and approved final version.
Footnotes
Supplementary Material
Supplementary table 1. Antimicrobial resistance profiles, disc induction phenotypes and resistance mechanisms, and MLVA and SCCmec types of MRSA isolates in this study.