
Abstract
Prosthetic joint infections (PJI) of the hip and knee are uncommon, but result in significant morbidity and mortality when they do occur. Current management consists of a combination of either single- or two-stage exchange of the prosthesis and/or exchange of polymer components with intravenous (IV) antibiotics (4–6 weeks) and intraoperative debridement of the joint prior to reimplantation. However, failure rate, morbidity, and expense associated with current management are high, especially if the infection involves resistant pathogens and/or osteomyelitis. Also, the current use of systemic antibiotics does not allow for high local concentrations of the drug and biofilm penetration of the infected prosthesis. To overcome these difficulties, we examined the outcomes of aggressive operative debridement of the infected prosthesis. This was achieved through the use of a single-stage revision and administration of high concentrations of local intra-articular antibiotics via Hickman catheters. We present 57 patients with PJI who were treated with intra-articular antibiotics and single-stage revisions. Minimal systemic toxicity was observed along with a 100% microbiologic cure rate and 89% without relapse at 11-month follow-up despite isolation of multidrug resistant pathogens. This is the largest study to date using this method in the treatment of PJI.
Introduction
Prosthetic joint infections (PJI) are uncommon. Cumulative incidence of total hip arthroplasty (THA) infections occurs in approximately 1%–2% of 1 million total knee arthroplasty (TKA) and hip arthroplasty over the prosthesis lifetime. 1 6 However, when PJI occurs, it is a significant complication, which is costly, debilitating, and associated with high morbidity and mortality. This is particularly true of infections with multidrug–resistant (MDR) bacteria, such as methicillin-resistant Staphylococcus aureus (MRSA), methicillin-resistant Staphylococcus epidermidis (MRSE), gram-negative organisms, and, occasionally, yeast. 7 10 These infections result in a much higher failure rate despite all present aggressive therapeutic measures. 11 13 Current management strategies involving the use of systemic antibiotics for 4–6 weeks and operative debridement of the joint with one- or two-stage hardware revisions result in an approximate 10%–20% failure rate.1,4,14–19 Such failure rates are thought to be associated with difficulty in obtaining high local intra-articular concentrations of antibiotics and/or penetration of biofilm with the use of systemic antibiotics. 1 Small case series describe the use of intra-articular antibiotics (IAA) for such infections with varied success. 20 22 We postulate an improvement in microbiologic outcomes and decrease in relapse and recurrent infection with the use of local intra-articular (IA) for prosthetic hip and knee infections. We present outcomes of a study involving 57 patients who were treated with IAA over a period of 4–6 weeks. All patients had presented with a relapse of PJI that had failed primary therapy with either oral or intravenous (IV) antibiotics with either one- or two-stage revision.
Methods
This was a multicenter study involving delivery of IAA for 4–6 weeks after relapse or recurrence of infection in hip and knee prosthesis. Ethics committee approval for the study was granted by the Las Palmas Del Sol Healthcare Institutional Review Board. The research was conducted in accordance with the Declaration of Helsinki. All patients had an initial one- or two-stage revision, placement of antibiotic cement spacer, and administration of 4–6 weeks of systemic IV antibiotics or oral antibiotics. Concomitant systemic antibiotics were not used during the administration of IAA. Fifty-seven patients (age range 36–91 years) with a history of a previously infected PJI (defined below) were enrolled in the study after the appropriate informed consents were obtained. Inclusion criteria included at least one of the following: patients with recurrence (same organism), relapse (new organism or culture negative), infection with a retained arthroplasty after incision and debridement of joint, and administration of systemic IV and/or oral antibiotics.
Primary outcomes were microbiologic cure and clinical cure. Microbiologic cure was defined as conversion from positive synovial fluid cultures to negative cultures. Clinical cure was defined as resolution of the clinical signs of infection and normalization of the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP).
Secondary outcomes were defined as resolution of relapse or recurrent infection after initial clinical and/or microbiologic response. Monthly follow-up of the patient was also done by two of the physicians to establish if recurrence or relapse of infection had occurred over 11 months. (Relapse or recurrent infection was deemed to occur if it was noted within the 6- to 8-month follow-up period).
Criteria for failure of primary therapy were defined as: pain, tenderness, and restricted range of motion, with and without a positive culture from an aspiration with obvious signs of infection and elevated ESR and CRP that had clinical evidence of relapsed or recurrent infection with same or different organism. Criteria for failure of primary therapy was defined as follows: (1) pain, tenderness, and restricted range of motion at the joint; (2) a positive aspiration was not necessary, but infection was suspected if obvious signs of infection were present, such as elevated ESR and CRP; (3) clinical evidence of relapsed or recurrent infection with same or different organism. If the aspiration or the cultures done intraoperatively were negative, we used the clinical signs of infection such as purulence of the joint fluid with leukocytosis, sinus tract, or histopathological evidence of synovitis as additional criteria.
IAAs were selected based on sensitivity data of synovial fluid culture. If synovial fluid cultures were negative or not available, antibiotics were empirically selected based on most likely pathogen(s). Hickman catheters was placed within the joint cavity and anchored to the skin. Two catheters were preferred for convenience of administration.
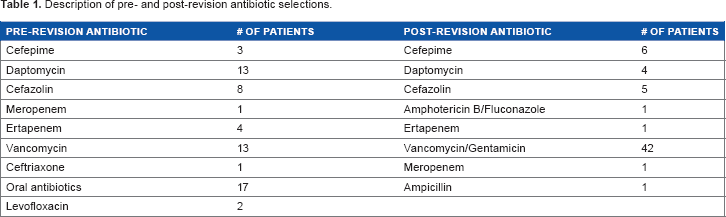
The antibiotics were infused in a concentrated solution through the catheter without flushes after the infusion. The drug was either given once a day or twice a day depending on the pharmacokinetics of the antibiotic. The dose of the vancomycin and gentamicin were selected depending on the random levels in the serum. We monitored the levels of vancomycin and gentamicin weekly through the entire infusion process keeping the trough levels in the higher range of normal as mentioned below. The dose of the other antibiotics was selected based on what we felt were appropriate to achieve high local concentrations. For drugs where there were no guiding data on its use in intra-articular infections, we calculated the dose by reducing it 50% from that of the serum dose, assuming it would achieve high concentrations in a confined space. Weekly fluid cultures from the Hickman catheter were obtained in all the patients. Complete blood count, complete metabolic panel, ESR, and CRP were obtained weekly. Vancomycin and gentamicin levels were also obtained weekly and were adjusted to the serum level of the vancomycin (random 8–20 mg/dL) and gentamicin (1–2 mg/dL). IAA included the following given as monotherapy or in combination with other antibiotics: vancomycin/gentamicin, vancomycin/meropenem, vancomycin/cefepime, cefazolin, daptomycin/cefepime, daptomycin/ertapenem, ampicillin, and cefepime/daptomycin. These antibiotics were chosen depending on the pathogens isolated (Table 1).
Description of pre- and post-revision antibiotic selections.
It was difficult to obtain intra-articular levels of the antibiotics, perform sonication of the fluid, or obtain 16rRNA testing of the synovial fluid due to the lack of these laboratory facilities. At the end of therapy, Hickman catheters were removed intraoperatively or in the office. The prosthesis in all the cases were either replaced by a single-stage antibiotic-impregnated methyl-methacrylate prosthesis or a temporary spacer was inserted (four cases) until clearing of the infection was achieved. This was then followed by placement of the prosthesis.
Results
There were 28 males and 29 females. The average age of males and females was 65 years (Table 2). Previously infected sites included 20 hip joints, 37 knee joints, and 1 elbow joint, 6-combined THA, TKA, and femur prosthesis. Antibiotics used to treat these patients prior to our revision included cephalexin (oral), vancomycin (IV), cephalosporin (IV), quinolones IV/per os, carbapenems IV, trimethoprim-sulfamethoxazole (oral), and daptomycin (IV) (Table 1). The average duration of treatment, prior to IAA, ranged from 10 to 42 days, with some having been treated on two occasions with systemic antibiotics and revisions. Following our revision, the IAA used included vancomycin, gentamicin, carbapenems, cephalosporin, daptomycin, and ampicillins or combination of drugs (Table 1).
Demographics.
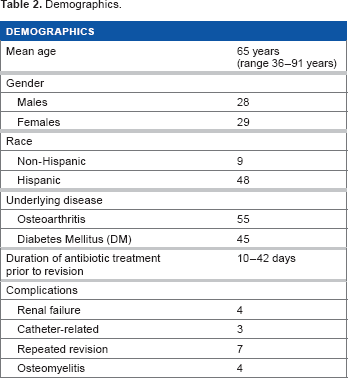
The combination of vancomycin/gentamicin was used in 39 of the patients with only 1 of these patients needing retreatment. None of these patients had positive cultures from the synovial fluid after the treatment. Daptomycin was used in four patients with none of these patients failing therapy. There did not appear to be a correlation between the antibiotics and the patients who failed therapy, but a relation seemed to exist with the multiple previous complex orthopedic surgeries and MDR pathogens seen in these patients. Complex orthopedic procedures (COP) were defined as patients having had multiple revisions to the joint (>2), having had previous multiple infections to the joint (>2), or two or more joints revised or infected. Forty-two patients met these criteria.
Osteomyelitis of the adjacent bone was documented in four patients (one patient with a TKA and one patient with a total elbow arthroplasty).
Fifty-three of the 57 patients underwent a single-stage procedure with concurrent IAA after the initial surgery. The remaining four patients had to have an antibiotic spacer inserted for 2–4 weeks while we achieved a sterile surgical site. This was done due to the overt infection of the joint noted by the surgeon at the time of surgery. Interestingly, all these patients had MDR pathogens (MRSA/MRSE/Pseudomonas aeruginosa).
All the patients were treated with IAA for 4–6 weeks after removal of the spacer and a revision without systemic antibiotics. One patient had to undergo an amputation due to mechanical failure of the prosthesis and lymphatic leak; the TKA from this patient was culture negative and the gram stain showed no white blood cells (WBCs). One patient died due to aspiration pneumonia (sudden onset of aspiration of food leading to respiratory failure), but had no clinical evidence of infection of the TKA at the time of death and was not considered a therapeutic failure as he died weeks after the knee joint was treated. Four of the patients who underwent a spacer/IAA were placed on oral suppressive antibiotics for 4 months. All the patients with complications mentioned above were from the group with COP.
Prior to the one-stage surgery, the average WBC count was 10 per cubic millimeter, hemoglobin and hematocrit 10 g/dL, 22%, platelets 222 k/mm3, ESR 87 mm/h, and CRP 8.8 mg/dL.
Follow-up cultures were negative in all patients. ESR and CRP returned to near normal (ESR ≥25 mm/h and CRP ≥1.0) in 87% of the patients at the end of 4 months. Reversible acute renal failure occurred in 4 patients secondary to gentamicin. These patients had received the vancomycin/gentamicin combination. All four patients had diabetes with possible diabetic nephropathy, which may have contributed to the renal failure. It took approximately 3 weeks for these patients to recover the renal function. Technical problems (leaking and catheter misplacement) occurred in three patients. The catheters were either removed or changed out.
Underlying pathogens prior to treatment included MRSA, MRSE, Escherichia coli, MSSA (methicillin-sensitive S. aureus), P. aeruginosa, vancomycin-resistant enterococcus (VRE), enterococcus, citrobacter, extended-spectrum beta-lactamase, yeast and mixed infections. Intraoperative cultures included MRSA/MRSE, yeast, and other gram-negative pathogens (Table 3).
Description of pathogen cultures from synovial fluid pre- and post-operatively.
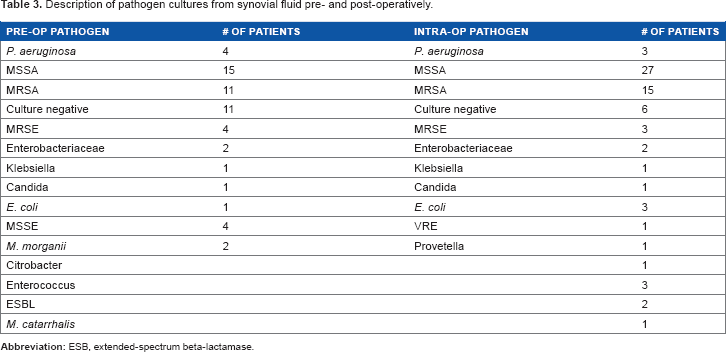
There were six patients who were culture negative but had clinical evidence of infections such as elevated ESR and CRP and drainage from the wounds, etc. These infections occurred in both the knee and hip joints.
Infected sites included THA, 20 TKA, 23 combined THA, TKA, and femur. 6 Microbiological cure occurred in 100% of the patients, but clinical failure occurred in six patients. All these six patients had MDR pathogens such as MRSA/MRSE and yeast. Of the patients, 89% had no evidence of recurrence/relapse at the end of 11 months.
There was one patient with a THA infected with yeast, who also had liver cancer, who was treated with intra-articular amphotericin B. This patient experienced poor wound healing but had normal ESR and CRP values. We suspect the poor wound healing was due to the immunosuppressive therapy being taken by the patient.
Underlying disease processes included osteoarthritis in 55/57 patients. There did not appear to be a predisposing underlying factor in this group of patients that seemed to predict failure versus success in the treatment except previous COP with MDR infections in the past. The class of antibiotic used in these patients prior to this revision did not appear to be related to the failure or success of the first surgery. Staphylococcus (MRSA/MSSA) still appeared to be the major cause of infection in this group of patients (42/57).
The primary outcome (microbiological) was a 100% cure as evidenced by repeated fluid cultures from the joints after the start of treatment (minimum three aspirations).
Secondary outcomes (no evidence of relapse/recurrence) occurred in 51/57 (89%) of the patients. All six patients who failed this form of therapy had COP with MDR pathogens and underlying medical issues.
Discussion
In general, the infection rate for primary hip arthroplasty is between 1% and 2% and that for revision hip arthroplasty is between 3% and 4%.8,24 In knee arthroplasty, the infection rate is usually ≥1% and ≥2% for revision procedures. 25 29 However, with repeated infections and COP with MDR pathogens, the failure rates are as high as 60%. 27 33 In this study, we observed a 100% microbiological cure and an 89% clinical cure (without relapse/recurrence) when patients were administered IAA and a one-stage revision at the 11-month follow-up. In previous studies, the failure rate for salvaging these arthroplasty (single-stage or a two-stage revision) with MDR and systemic IV antibiotics was between 41% and 66%, but in this patient population, the response rate seems favorable using high local antibiotic concentration along with a single-stage revision.29,32–36 Smaller studies describing the use of IAA showed almost a 100% cure with single pathogens and one-stage revision and IAA therapy.20,22,37,38
Our study differed from the others in the following respects: (1) size of the patient cohort; (2) severity of underlying illness and history of previous failures; (3) several of our patients had complex orthopedic prosthesis and had several surgeries done prior to this one stage; and (4) many of our patients had polymicrobial pathogens with MDR infection. This difference in the success/failure rate is probably due to the high drug concentrations achieved in the joint space.
Despite the cure rate of 89%, which does not differ significantly from previous studies, the rate of limb salvage in COP with MDR pathogens seems to be much better in this series than in previous studies in which the rate was between 41% and 66%.7,13,33–35 This method of treatment may be a useful alternative in patients who have no option but drastic surgeries such as disarticulation/amputation.
In addition, the lack of systemic toxicity from the IV antibiotics was noticeably absent as was the fact that these patients were ambulatory almost immediately. These appear to be distinct advantages over the two-stage method with IV systemic antibiotics. The financial savings, if calculated, would be substantial as there is only a one-stage revision performed, lack of systemic antibiotics (cost, side effects, central line devices), and reduced physical therapy and rehabilitation cost.
Successful treatment of hip infections with two-staged reimplantation with IV antibiotics has been reported to range from approximately 80% to 92%, depending on the series published. The success rate for the infections has been reported to be around 80% following staged reimplementation if a low-virulence organism (MSSA, anaerobic cocci, and streptococci other than group D) is isolated.15,23,39,40 The success rate has been reported to decrease to 40% in patients with highly virulent infections such as gram-negative organisms, polymicrobial infections, enterococcus, methicillin-sensitive staphylococci, and any organism that elaborates a glycocalyx, which typically increases the virulence of the organism. 15 , 39 , 40 The use of IAA in this study seems to circumvent these pharmacologic difficulties due to the high concentrations achieved. Thus, having MDR organisms may not be such a major issue if the arthroplasty is treated in this manner.
In some series, patients underwent debridement with the retention of prosthesis and resection of sinus tracts with IV antibiotics. The failure rates were again high (40%–67%).14,22,41 Use of a one-stage revision with IAA may overcome this problem as well.
The cornerstone to a successful outcome in this group of patients will be aggressive debridement of the infected tissue, resection of the sinus tract, and removal of the biofilm-coated hardware. It would be very difficult to effectively cure these patients if the biofilm is not removed and if the drug does not penetrate the biofilm. Again, use of a single-stage revision with aggressive debridement and high concentration of IAA would seem to be useful.
Osteomyelitis continues to be a major problem in orthopedic surgery. Staphylococci, gram-negative bacteria, and anaerobes cause the majority of the cases. 24 , 33 Osteosynthesis implant devices are at high risk of infection by bacteria with multiple drug resistance, such as MRSA, MRSE, and VRE. Successful treatment outcomes are affected by both systemic and local factors. These factors include the following: (1) whether radical surgical debridement was performed; (2) choice of antimicrobial agent or regimen; (3) the ability of the drug to reach and maintain effective concentrations at the site of the action; (4) the ability of the drug to penetrate into the infected bone and joint tissue; (5) underlying medical problems of the patient; 41 and (6) presence of biofilm on the prosthesis and bone. In this study, there were four patients with associated osteomyelitis in addition to PJI. All these patients did well with surgical debridement and IAA. One will need to be cautious in interpreting these data based on the small number of patients, but clinical success was noted in all four patients marked by normalization of inflammatory markers and decreased pain/swelling/increased range of motion.
Microbiology and in Vitro Antibiotic Joint Concentrations
In some laboratory studies, the joint penetration of both vancomycin and teicoplanin ranged from ≥15% to a satisfactory range of 15%–30% in the cortical compartment, but was much higher in the highly vascular cancellous tissue. 42 , 43 Higher bone concentration of vancomycin was observed in patients who had higher inflammatory markers and this was probably due to the increased vascularized tissue and vascular permeability under inflammatory conditions. 44 Bone concentrations over the MIC and area under the curve/MIC ratios suggested that glycopeptides achieve a satisfactory pharmacokinetic exposure in the cancellous bone, as far as gram-positive pathogens are concerned.23,45–47 This can be seen with MDR bacteria, which tend to absorb antibiotics at a much higher rate when there is a local infection. 48 51 The high intracellular levels achieved overcome many resistance mechanisms. There are some reported data that local vancomycin concentrations can range between 50 and 2,095 μg/mL and in vitro testing has demonstrated that vancomycin will precipitate rapidly when mixed with small amounts of cephalosporins, clindamycin, and penicillins.50,51
Difficulties encountered when managing these types of joint infections include negative intraoperative cultures, with clinical signs of an infectious disease process actively occurring (such as elevated ESR and CRP).
A study done in patients who were culture negative at the time of surgery, but had signs of infection, revealed that routine hospital culturing of the tissue showed bacterial growth in only 9/22 (41%). The same specimens underwent prolonged culturing with resultant bacterial growth noted in 14/22 of the patients (64%). However, when they cultured the scrapings from the biomaterial surface of the explanted prosthesis, bacterial growth was noted in 19/22 patients (86%).14,46,48,52 This method of culturing the biofilm appears to be more useful when deciding on the antimicrobial therapy and surgical intervention.46,48 This, unfortunately, is not done on a routine basis in most PJI patients and was not done in our patients who were culture negative. Use of sonication of the tissue/fluid and the use of polymerase chain reaction in identifying the microbes are also useful tools in this situation, but these are not easily available and have not been standardized in clinical studies. 53 61 These advanced methods of detection of microbes along with IAA and a single-stage revision may prove to be a useful alternative in culture-negative infections.
Conclusion
In this study, we observed a 100% microbiologic cure and 89% clinical cure in patients who underwent a one-stage revision with IAA with an 11-month follow-up, even when MDR pathogens were cultured. Failure rates with this method appear to be acceptable.
This method appears to have several important advantages (1) one-stage revision compared to two-stage revision involves less surgery, cost, morbidity, and possibly less surgical mortality; (2) there is less tissue/bone manipulation allowing for better wound healing and fixation of prosthesis; (3) there are possibly reduced morbidity and mortality rates using this method; (4) it is possible that MDR pathogens may not be a major factor in the salvage of these prosthesis as much higher concentrations of the drug can be given in this way to overcome the MIC of the pathogen without systemic toxicity; (5) failure rates using this method appear to be acceptable at this time; (6) side effects and systemic toxicity appear to be minimal and acceptable as well; (7) finally, it is theoretically conceivable that the prosthesis can be sterilized and reused immediately (assuming biofilm can be successfully removed) resulting in substantial savings to the health-care systems.
Shortcomings of this study include the fact that this is an observational study without a blinded comparator arm, small population size, and length of follow-up may be inadequate to assess relapse. There is a widespread lack of the ability to measure synovial concentrations of the antibiotics or determine MICs, and at this time, there is a lack of standardization for dosing and administration of IAA. In addition, surgical expertise and familiarity in placing the Hickman catheter and familiarity with IAA may not be widely available.
Single-stage revision of PJIs along with appropriate intra-articular antibiotics appears to be a safe, effective alternate option in many patients with infected prosthetic joints, especially with MDR pathogens. Randomized controlled studies are needed to establish long-term recommendations.
Author Contributions
Conceived and designed the experiments: SA, JH, JJ, RW. Analyzed the data: SA, JJ, RW, JN, JH. Wrote the first draft of the manuscript: SA. Contributed to the writing of the manuscript: SA, RW, JH, JJ, JN. Agree with manuscript results and conclusions: SA, JJ, JH, RW, JN. Jointly developed the structure and arguments for the manuscript: SA, JH, RW, JJ. Made critical revisions and approved the final versions: JH, JJ, RW, JN. All authors approved and reviewed the final manuscript.
Footnotes
Acknowledgments
We would like to acknowledge Dr Rupal Mody and Dr Craig Cameron for their insightful comments in the writing of this paper.