
Abstract
Background
Marital status is a known prognostic factor in overall and disease-specific survival in several types of cancer. The impact of marital status on survival in patients with carcinoid tumors remains unknown. We hypothesized that married patients have higher rates of survival than similar unmarried patients with carcinoid tumors.
Methods
Using the Surveillance, Epidemiology, and End Results database, we identified 23,126 people diagnosed with a carcinoid tumor between 2000 and 2011 and stratified them according to marital status. Univariate and multivariable analyses were performed to compare the characteristics and outcomes between patient cohorts. Overall and cancer-related survival were analyzed using the Kaplan–Meier method. Multivariable survival analyses were performed using Cox proportional hazards models (hazards ratio [HR]), controlling for demographics and tumor-related and treatment-related variables. Propensity score analysis was performed to determine surgical intervention distributions among married and unmarried (ie, single, separated, divorced, widowed) patients.
Results
Marital status was significantly related to both overall and cancer-related survival in patients with carcinoid tumors. Divorced and widowed patients had worse overall survival (HR, 1.33 [95% confidence interval {CI}, 1.08–1.33] and 1.34 [95% CI, 1.22–1.46], respectively) and cancer-related survival (HR, 1.15 [95% CI, 1.00–1.31] and 1.15 [95% CI, 1.03–1.29], respectively) than married patients over five years. Single and separated patients had worse overall survival (HR, 1.20 [95% CI, 1.08–1.33] and 1.62 [95% CI, 1.25–2.11], respectively) than married patients over five years, but not worse cancer-related survival. Unmarried patients were more likely than matched married patients to undergo definitive surgical intervention (62.67% vs 53.11%, respectively, P < 0.0001).
Conclusions
Even after controlling for other prognostic factors, married patients have a survival advantage after diagnosis of any carcinoid tumor, potentially reflecting better social support and financial means than patients without partners.
Keywords
Introduction
Several studies have demonstrated a positive association between marriage and outcomes for patients with cancer. Whether as a proxy for an enhanced social network or because of a spouse's influence on health-related behaviors, married individuals have repeatedly been found to fare better in terms of general health at presentation, use of definitive therapy, and overall survival following a diagnosis of cancer.1–11
The association between marital status and improved overall and cancer-related survival persists in a variety of different cancers.1,2,4,11 It has been observed in colorectal, pancreatic, skin, breast, and head and neck cancers, among myriad others, with married patients consistently demonstrating greater longevity.1,2,5–7,11–13 For certain cancers, marital status even has a greater impact on survival than that of chemotherapy.2,10 This relationship is further modulated by sex status, as shown in urothelial carcinoma among others, with survival among women consistently higher than survival among men.14,15
There have been several theories proposed to explain this outcomes benefit, including increased health care utilization, greater access to health insurance, and decreased sense of social isolation and loneliness in married individuals.2,8–10 With only theories of causal factors, data regarding the differential effect of marital status on survival after diagnosis of cancer prompt questions about the extent to which health care providers should identify and seek to minimize potential marriage-related disparities. Certainly, marital status is a modifiable lifestyle factor, albeit not in a conventional sense.
In 2010, the US Census found that ~51% of the US population was married, which is significantly fewer than the 72% of married adults in 1960. Although divorce rates have plateaued in recent decades, the decline in marriage may have implications for population health. 16 Further investigation is warranted to determine whether this trend is manifesting in increasing rates of chronic disease, including cancer, over time and whether physician-directed initiatives can alter its course.
Carcinoid tumors represent a type of neuroendocrine malignancy that may arise in a wide range of organs, most commonly in the gastrointestinal (GI) and respiratory tracts. Five-year survival is ~70%, with significant variation depending on tumor stage at presentation and site of primary tumor, among other factors.14,17–20 For example, foregut tumors have historically been shown to demonstrate ~70% five-year survival, whereas survival is ~60% for midgut carcinoids and ~88% for hindgut carcinoids. 18 Carcinoids presenting with regional metastases demonstrate 71% five-year survival, whereas those with distant metastases have just under 40% five-year survival.14,17–19 Given the variation in survival estimates and the paucity of literature exploring the socioeconomic factors that moderate survival in this cancer, we studied the impact of marital status on survival in patients with carcinoid tumors. Using a large, national tumor registry, we hypothesized that married patients would have higher rates of disease-specific survival than similar unmarried patients with carcinoid tumors.
Methods
Data
This was a retrospective, cohort study using administrative data collected by the National Cancer Institute (NCI) for their Surveillance, Epidemiology, and End Results (SEER) national tumor registry from 2000 to 2011. SEER is an administrative database developed by the NCI to report on cancer incidence and survival in the United States, with data collected from population-based cancer registries that cover ~28% of the US population.21,22 It is the only population-based database that includes comprehensive cancer information, such as stage and survival, on all patients diagnosed with cancer in the registry areas between 1973 and 2012, thereby allowing study of overall and disease-specific survival.
We queried the SEER database to identify patients with a diagnosis of carcinoid tumor (n = 23,978) using International Classification of Disease for Oncology, 3rd edition, code 8420 with a behavior code of 3. After excluding 852 patients who survived less than one month following entry to the data set, there were 23,126 patients with carcinoid tumors in the final analysis.
The cohort was stratified according to marital status at the time of carcinoid diagnosis, with discrete strata for married, single, separated, divorced, and widowed patients. Analyses controlled for several patient variables, including demographics (age, sex, race, geographic region), site of primary tumor (colorectal, other digestive, lung, and bronchus, other non-GI), extent of tumor spread (localized, regional, distant), tumor grade (well-differentiated, moderately differentiated, poorly differentiated, undifferentiated, no differentiated/unknown), and pursuit of surgical resection. The primary outcomes of interest in this study were five-year overall survival, defined as death attributable to any cause, and cancer-specific survival, defined as death attributable to one's malignancy.
Statistical analyses
Statistical analyses were performed to determine whether marital status was significantly associated with five-year survival after controlling for important prognostic covariates. Baseline patient demographics and disease characteristics were compared between married, single, separated, divorced, and widowed patients utilizing chisquare tests for binary and categorical variables. We reported proportions with associated P-values.
The Kaplan–Meier method was used to estimate survivor functions. Differences between survival curves were tested using the log rank test. We also performed multivariable survival analyses using Cox proportional hazards models. Hazard ratios (HRs) and corresponding P-values and 95% confidence intervals were reported. Additionally, we reported the total number of deaths and total number of patients censored at one year and five years for each of the marital strata within survival analyses.
In order to determine if the survival effect could be explained by differential rates of definitive surgical intervention between married and unmarried (ie, single, separated, divorced, widowed) patients, we conducted a propensity score analysis. Married and unmarried patients were matched on demographic, disease, and treatment characteristics. We tested an overall treatment difference using 500 bootstrap replicates in order to obtain a confidence interval. All statistical analyses were performed using STATA software (version 12) and the psmatch2 routine.23,24 Statistical significance for all analyses was defined as a P-value <0.05. The study was conducted in accordance with the Declaration of Helsinki, and the study protocol was approved by the Institutional Review Board of the Penn State Milton S. Hershey Medical Center.
Results
Patient characteristics
Patients with carcinoid tumors treated in the US within 18 SEER geographic areas between 2000 and 2011 were included in the SEER database. The analysis sample included 23,126 patients stratified as married (n = 14,872), single (n = 3,430), separated (n = 272), divorced (n = 1,973), or widowed (n = 2,579). Demographic and tumor-related characteristics are shown in Table 1. There were statistically significant differences in age, sex, race, and geographic region between patients across marital status. Of note, widowed patients were clearly more likely to be older (P < 0.001) and female (P < 0.001) relative to other patients. There were also statistically significant differences across marital status for site of primary tumor (P < 0.001), tumor spread (P < 0.001), and proportions of patients undergoing tumor resection. More specifically, single patients more commonly presented with earlier stage carcinoid tumors (localized, 72.4%; regional, 16.6%; distant, 11.0%), whereas widowed patients more commonly presented with concomitant regional or distant metastases (localized, 59.3%; regional, 22.3%; distant, 18.5%). Similarly, single patients had the highest rate of definitive surgical intervention, whereas widowed patients had the lowest (68.0% vs 51.6%, respectively).
Demographic and disease characteristics of patients with carcinoid tumors, stratified by marital status.

Five-year survival
Figure 1 presents the results of Kaplan–Meier analysis for overall survival, stratified by marital status. Of patients who died within five years, time to death from any cause was significantly different between patients of different marital statuses (P < 0.0001). At one year and five years, married patients had rates of 94.7% and 82.3% overall survival, respectively, with median survival of 232 months. Single patients had 94.2% one-year and 84.5% five-year overall survival with median survival of 328 months. Separated patients had 90.2% one-year and 75.1% five-year overall survival with median survival of 128 months. Divorced patients had 92.2% one-year and 78.5% five-year overall survival, and widowed patients demonstrated 86.3% one-year and 61.3% five-year overall survival. Median survival for divorced and widowed patients was 205 and 88 months, respectively.
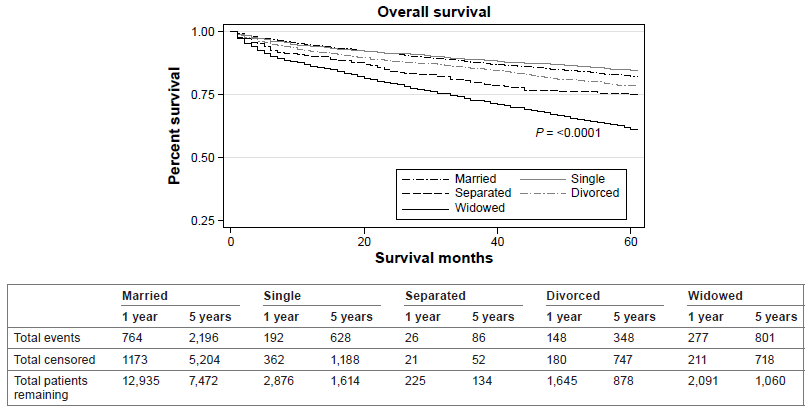
Overall five-year survival for patients with carcinoid tumors, stratified by marital status.
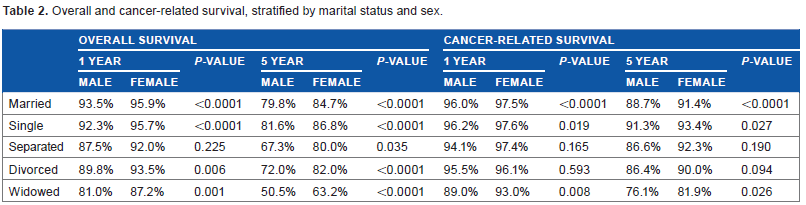
Figure 2 presents the results of Kaplan–Meier analysis for cancer-related survival. Of those patients who died within five years secondary to cancer-related causes, time to cancer-related death was significantly different between patients of different marital statuses (P < 0.0001). More specifically, married patients exhibited 96.7% one-year and 90.0% five-year cancer-related survival. Single patients had 96.9% one-year and 92.5% five-year cancer-related survival. Separated patients had 96.1% one-year and 90.2% five-year cancer-related survival. Divorced patients had 95.9% one-year and 88.7% five-year cancer-related survival. Widowed patients exhibited 92.4% one-year and 81.1% five-year cancer-related survival. Survival trends were consistent after further stratifying patients according to sex, although with significantly better overall and cancer-related survival in females (Table 2).

Cancer-related five-year survival for patients with carcinoid tumors, stratified by marital status.
Overall and cancer-related survival, stratified by marital status and sex.
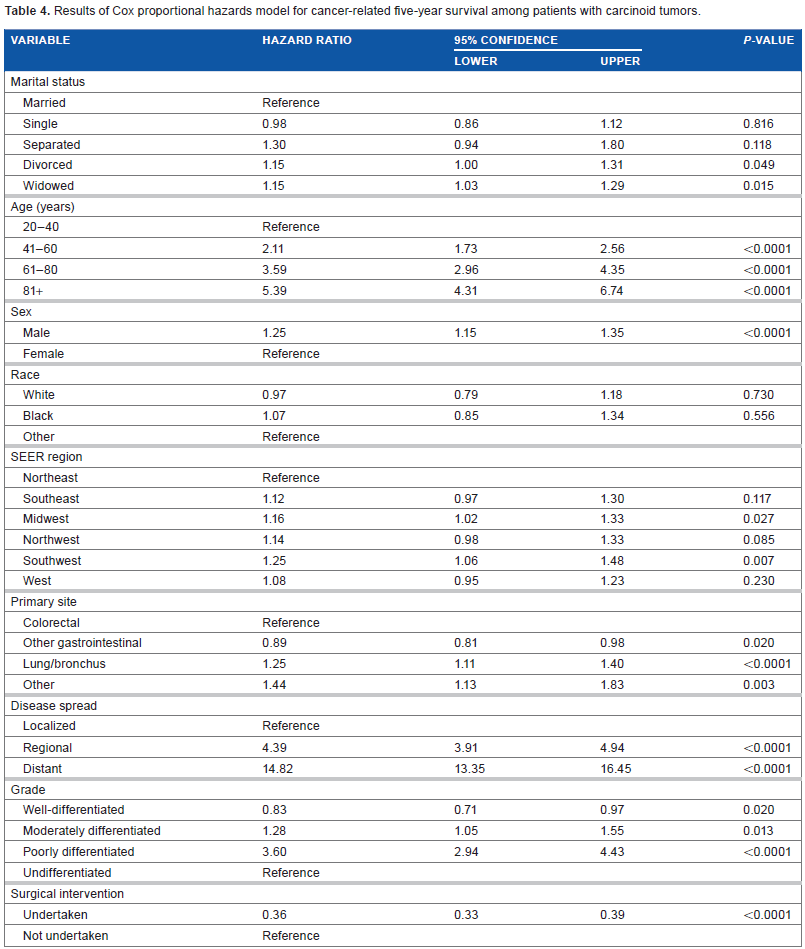
Multivariable analysis confirmed marital status as a statistically significant prognostic factor in overall and cancer-related survival, as shown in Tables 3 and 4. After controlling for other covariates, single patients had worse overall five-year survival (HR, 1.20, P = 0.001), but not worse cancer-related survival (HR, 0.98, P = 0.816). Separated patients had worse overall survival (HR, 1.62, P = 0.001), but not worse cancer-related survival (HR, 1.30, P = 0.118). Divorced patients had worse overall survival (HR, 1.33, P < 0.0001) and worse cancer-related survival (HR, 1.15, P = 0.049). Widowed patients had worse overall survival (HR, 1.34, P < 0.0001) and cancer-related survival (HR, 1.15, P = 0.015). Other variables in multivariable analyses that predicted worse overall five-year survival included age (P < 0.0001, all categories), male sex (P < 0.0001), black race (P < 0.0001), treatment in the South or Midwest (Southeast, P = 0.003; Midwest, P = 0.010; Southwest, P = 0.022), non-colorectal non-respiratory primary tumor (other digestive, P = 0.010; other, P = 0.026), tumor spread (P < 0.0001, all categories), and histological poor differentiation (P < 0.0001). Tumors that are well differentiated (P = 0.017) or treated by surgical resection (P < 0.0001) were protective for overall survival. Cancer-related survival differed from overall survival with respect to single, separated, and black patients, who did not have significantly worse cancer-related five-year survival. Cancer-related survival was significantly better with a non-colorectal digestive primary tumor (P = 0.020), but worse with a respiratory primary tumor (P < 0.0001), relative to colorectal carcinoids. Cancer-related survival was worse in carcinoids with moderate or poor differentiation relative to undifferentiated tumors (P = 0.010).
Results of Cox proportional hazards model for overall five-year survival among patients with carcinoid tumors.

Results of Cox proportional hazards model for cancer-related five-year survival among patients with carcinoid tumors.
After observing that univariate analysis of one- and five-year survival varied as a function of sex, Cox proportional hazards models for overall and cancer-related survival confirmed this effect. Again, males had substantially worse overall survival across all marital strata, while females had better overall survival, even to the extent of reversing statistical significance among single females and separated females, thereby showing that there was no difference in survival relative to the reference married female. The substantial differences seen in overall survival among men and women generally did not manifest for cancer-related survival as survival among the marital status cohorts did not diverge from that of the reference married individual. The single exception to this finding was among widowed patients. Widowed males did not differ in cancer-related survival from the reference married males, whereas widowed females had a 15% greater hazard of death from cancer (P = 0.040) relative to the reference married females.
Definitive surgical intervention
Propensity score analysis showed that married patients were not more likely to undergo definitive surgical intervention relative to patients without partners but that unmarried patients were more likely to undergo definitive surgical intervention (62.67% vs 53.11%, P < 0.0001), after matching married and unmarried patients on all demographic and disease-related characteristics, including tumor stage and grade.
Discussion
The effect of marriage on mortality has been consistently shown in various chronic disease states, including different types of cancer.1,5–7,12,13 Whereas health care providers target many other modifiable risk factors for intervention, marital status has yet to be the focus of such initiatives. Relationship counseling and online dating websites notwithstanding, efforts can otherwise be directed toward identifying populations at risk and disparities in care.
In this study of the relationship between marital status and survival for patients with carcinoid tumors, we found that married patients had a survival advantage relative to unmarried patients in both overall and cancer-related survival. This effect persisted from one year to five years, even after controlling for age, sex, race, geographic region, site of primary tumor, stage of disease, tumor grade, and receipt of surgical intervention. Although single patients fared similarly to married patients in univariate analyses, single patients had a 20% greater hazard of decreased overall five-year survival relative to married patients in multivariable analyses. Not surprisingly, these results further confirmed findings of previous studies with respect to the effect of age, sex, site of primary tumor, and degree of tumor spread on cancer-related survival.14,18–20,25,26
Survival secondary to cancer-related causes differed significantly between patients of different marital statuses in our study, with previously married patients having worse survival relative to currently married patients. Five-year cancer-related survival ranged from 81% to 93% among all patients, which is consistent with previous literature on carcinoid-related mortality.17–20,27,28 A significant amount of variation in rates of cancer-related survival between previous studies, from 67.5% to 94%, is likely attributable to the diversity that characterizes carcinoid tumors. This variation was reflected in our Kaplan–Meier analysis of five-year cancer-related survival for all carcinoid variants. Although known to be a tumor with generally good prognosis, carcinoids demonstrate different degrees of aggressiveness depending on tumor characteristics such as site of primary pathology and stage at presentation.14,18 Still, these causes of variation did not diminish the effect of marital status on survival in our multivariable model. Moreover, we found that among matched married and unmarried patients, the rate of definitive surgical management among married patients was lower than that of unmarried patients in spite of matching on several prognostic factors, thereby suggesting that the effect of marriage cannot be explained by a greater likelihood of undergoing surgical treatment. Hence, targets for intervention might more appropriately focus on social initiatives, such as more frequent follow-up by clinicians, rather than on interventions focused predominantly on access to surgical treatment. To our knowledge, this study is the first to demonstrate a statistically significant relationship between five-year cancer-related survival and marital status in patients across all carcinoid tumors.
Our finding of a survival advantage for married patients has been demonstrated in other disease states and in a multitude of other cancers. Kaplan and Kronick 3 found within a US population that married people tend to live longer overall. 3 Manzoli et al 8 showed that among the elderly exclusively, marriage was a significant protective factor in overall mortality. 8 They posited that separated/divorced and widowed elderly have a greater risk of mortality secondary to the impact of stress related to marital dissolution or bereavement. Marital status not only bears psychological influence but also has been shown to influence immune and neuroendocrine function. 9 Hence, the benefits of marriage are well described.
More specific to cancer-related survival, numerous previous studies have shown a survival advantage for married individuals with a variety of cancers, including those within the colon, kidney, testis, head and neck, bladder, cervix, and skin/soft tissue among other oncologic disease states.1,4,6,7,11–13 While the threat of publication bias is certainly a concern, even pancreatic adenocarcinoma and glioblastoma multiforme, two particularly insidious tumors, have shown improved prognosis in married individuals relative to unmarried individuals.5,7 Moreover, Aizer et al 2 found that the survival benefit of marriage surpassed that of chemotherapy in patients with prostate, breast, colorectal, esophageal, and head/neck cancers. Our findings are congruent with the findings of these previous studies.
As a corollary, we found that unmarried individuals tended to have a greater hazard of mortality relative to married individuals. The mechanism underlying this hazard has not been conclusively determined in this or previous research, but theories exist in the literature.8,9 Perhaps, related to a lack of social support or even supervision, unmarried patients have been shown to present at a later stage and have decreased adherence to therapeutic regimens. Indeed, several analyses have confirmed that unmarried patients present later and are less likely to receive definitive therapy.1–3,6 However, Chang and Barker 7 found that even across patients who received treatment for glioblastoma multiforme, unmarried patients had shorter survival than married patients. 7 Wang et al 1 similarly showed that this effect persisted after controlling for tumor stage at presentation and receipt of surgery. Likewise, we found that the increased hazard secondary to being unmarried was present even after accounting for carcinoid tumor site, stage, and receipt of surgical intervention.
An interesting finding in the present study was the lack of an association between status as a single patient and decreased hazard of cancer-related survival in multivariable analysis. In univariate analysis, single patients actually had slightly better overall and cancer-related survival relative to married patients. This is likely because single patients were among the youngest patients and presented more often at an earlier stage of disease. However, after controlling for other variables, status as a single patient did not show a statistically significant cancer-related survival benefit. While this finding differs from most previous studies, it may actually suggest that loss of a spouse, rather than never having had one, may explain decreased survival in divorced and widowed patients.2,8,9 This is further bolstered by the lack of an association between status as a separated patient, who theoretically still maintains a spouse, and cancer-related survival. Our finding may support theories regarding a synergistic effect of cancer and stress, biological or otherwise, associated with loss of a spouse on survival.
Our findings indicate a survival advantage conferred by marriage in carcinoid patients; yet, there are limitations to the present study. SEER data lack information regarding changes in marital status over the five-year study period. The threat of marital discord and divorce resulting from the stress created by a cancer diagnosis is likely not small and thereby raises the possibility that patients in our married cohort may have transitioned to the separated or divorced cohort. 8 Other patients who entered the database as single may have subsequently been married. These changes in marital status are frequently accompanied by significant social and economic changes, including modifications in insurance status. Given the greater likelihood of marital discord rather than marital union in patients with cancer, it is likely that a portion of patients in the married group became separated or divorced and that incorporating data on these transitions would enhance our finding of a survival benefit in married individuals. Additionally, SEER data do not provide information regarding the nature of individuals’ relationships beyond marital status classification at the time of diagnosis. For example, classification as married may not equate with being in a stable, nurturing relationship or even with cohabitation. Likewise, classification as single does not eliminate the possibility of having a long-standing partner. Therefore, there is potential that marital status categorization does not accurately reflect relationship status and support network. However, this limitation in the database would likely not systematically impact every patient and therefore would only mediate outcomes in a minority of individuals.
Another limitation to the present study is a minimum of demographic data collected in the SEER database with which to control for in our multivariable model. Without data on living arrangement, income, comorbidities, and other socioeconomic factors and demographic variables, it is not known whether these variables actually mediate the survival advantage of marriage. 17 Hence, our findings might be better explained by an exogenous, unobserved demographic factor.
This study suggests that married patients with carcinoid tumors have better overall and cancer-specific survival than other patients. Given the wide variation in the presentation of this particular malignancy, further study should consider each organ system affected by carcinoid tumors in order to determine whether the influence of marriage persists.
Conclusions
We conclude based on this nationwide analysis of administrative data for individuals with carcinoid tumors that married individuals have a survival advantage relative to unmarried individuals. Other factors, such as social support, may mediate the association between marital status and survival and thereby present an opportunity for health care providers to identify populations at risk and disparities in care. Future efforts should be directed toward identifying other mediators in the relationship between marriage and survival in patients with carcinoid tumors, implementing interventions to counteract these influences and ultimately assessing the effectiveness of such interventions to improve survival in this patient population.
Author Contributions
Study concept and design: ABC and CSH. Acquisition and analysis of data: EKG and CSH. Interpretation of data: EKG, ABC, and CSH. Drafting of the manuscript: EKG. Critical revision of the manuscript for important intellectual content: EKG, ABC, and CSH. Study supervision: CSH.
Footnotes
Acknowledgment
The authors gave a poster presentation of this research at the Society of Surgical Oncology 2015 Annual Symposium, Houston, TX, March 25–28, 2015.