
Abstract
In clinical studies, skeletal myoblast (SKMB) transplantation late after myocardial infarction (MI) has minimal impact on left ventricular (LV) function. This may be related to our previous observation that the extent of SKMB engraftment is minimal in chronic MI when compared to acute MI, which correlates with decreased hepatocyte growth factor (HGF) expression, an important regulator of SKMB function. Here, we investigated delivery of exogenous HGF as a strategy for augmenting SKMB engraftment late after MI. Rats underwent SKMB transplantation 4 weeks after coronary ligation. HGF or vehicle control was delivered intravenously during the subsequent 2 weeks. LV function was assessed by MRI before and 2 weeks after SKMB transplantation. We evaluated HGF delivery, SKMB engraftment, and expression of genes associated with post-MI remodeling. Serum HGF was 6.2 ± 2.4 ng/mL after 2 weeks of HGF infusion (n = 7), but undetectable in controls (n = 7). LV end-diastolic volume and ejection fraction did not improve with HGF treatment (321 ± 27 mm3, 42% ± 2% vs. 285 ± 33 mm3, 43% ± 2%, HGF vs. control). MIs were larger in HGF-treated animals (50 ± 7 vs. 30 ± 6 mm3, P = 0.046), but the volume of engrafted SKMBs or percentage of MIs occupied by SKMBs did not increase with HGF (1.7 ± 0.3 mm3, 4.7% ± 1.9% vs. 1.4 ± 0.4 mm3, 5.3% ± 1.6%, HGF vs. control). Expression of genes associated with post-infarction remodeling was not altered by HGF. Delivery of exogenous HGF failed to augment SKMB engraftment and functional recovery in chronic MI. Expression of genes associated with LV remodeling was not altered by HGF. Alternative strategies to enhance engraftment of SKMB must be explored to optimize the clinical efficacy of SKMB transplantation.
Introduction
Skeletal myoblast (SKMB) transplantation has been extensively investigated as a strategy to positively influence ventricular remodeling following myocardial infarction (MI). While SKMBs transplanted by direct injection improved ventricular function in animal models of myocardial injury,1,2 a randomized trial in patients with chronic MI did not show improved ventricular function compared to controls. 3 We previously reported that the timing of SKMB transplantation relative to the MI influences the extent of engraftment. 4 If SKMB transplantation is delayed until a chronic MI scar has developed, there is a 95% reduction in the volume of engrafted SKMBs compared to transplantation immediately after MI. 4 This may be why in the clinical setting, SKMB transplantation into a chronic MI scar does not have a major impact on ventricular remodeling.3,5 Strategies to augment engraftment of SKMBs transplanted late after MI may enhance the utility of this therapy in the clinical situation, where the time required for isolation and expansion of autologous SKMBs in culture precludes immediate delivery after an MI. We observed a correlation between the degree of SKMB engraftment and the amount of hepatocyte growth factor (HGF) present in the MI, which declined over time. 4 HGF is the primary regulator of skeletal muscle repair by SKMBs.6–9 We showed in vitro that recombinant human HGF can augment SKMB proliferation and protect against hypoxia and oxidative stress, 4 effects that may assist SKMB engraftment following transplantation into an MI. Since decreased HGF in the MI scar over time correlates with degree of SKMB engraftment, 4 the aim of this study was to determine whether delivery of exogenous HGF could enhance engraftment of SKMBs transplanted into a chronic MI scar.
Methods
Animals
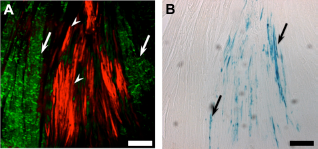
Inbred Dark Agouti transgenic rats expressing β-galactosidase under the CAG promoter (DA-Tg(CAG-lacZ)30 Jmsk) 10 were obtained from the Rat Resource and Research Center (Columbia, MO, USA) and a breeding colony established at our center. These animals have widespread β-galactosidase activity that is particularly strong in skeletal muscle (Fig. 1A). We maintained inbred transgene positive and wild-type lines, which were used as SKMB donors and recipients, respectively. All animals were genotyped prior to inclusion in the study using the REDExtract-N-Amp Tissue PCR Kit (Sigma Chemical Co., St. Louis, MO, USA) according to manufacturer's instructions and the primers GAATCTCTATCGTGCGGTGGTTGA (forward) and GCCGTGGGTTTCAATATTGGCTTC (reverse). Animals were cared for in accordance with the Canadian Council on Animal Care guidelines. The Dalhousie University Committee on Laboratory Animals approved the experimental protocol.
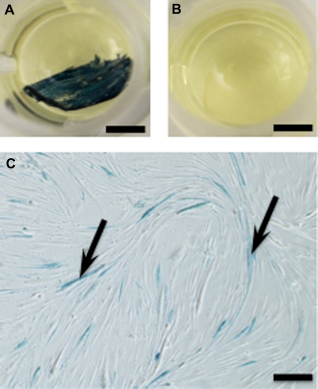
Characterization of β-galactosidase staining. Representative images from X-gal stained tissues and cultured cells. (
Experimental protocol
The experimental protocol was 6 weeks long (Fig. 2). Male transgene negative rats (SKMB recipients, approximately 20 weeks old) underwent coronary ligation. During week 4, cardiac Magnetic resonance imaging (MRI) was performed and SKMBs were harvested from male transgene-positive rats (SKMB donors, approximately 24 weeks old). Implantation of an osmotic pump carrying HGF or vehicle control, and transplantation of SKMBs into MI scars of recipients occurred at the end of week 4. A second cardiac MRI was performed at the end of week 6.
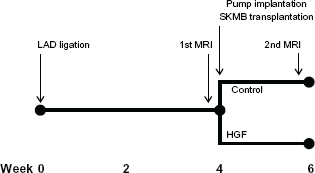
Experimental protocol.
Coronary ligation
Rats were anesthetized with ketamine hydrochloride (26 mg/kg intraperitoneally), xylazine (4.8 mg/kg intraperitoneally), and isoflurane (approximately 2%), intubated, and ventilated. The mid-left anterior descending coronary artery was ligated through a left thoracotomy. Animals were extubated when breathing spontaneously. Ketoprofen (5 mg/kg subcutaneously) and buprenorphine (0.03 mg/kg subcutaneously, every 8 to 12 h × 4 doses) were used for analgesia.
Cardiac MRI
MRI scans were performed using a Magnex Scientific Scanner (Oxford, UK) interfaced with a Direct Drive spectrometer (Varian Inc., Palo Alto, CA, USA). A custom quadrature radio frequency (RF) transmit/receive volume coil was used for imaging. Rats were anesthetized with isoflurane (2%–3%) and were spontaneously breathing. A 3D balanced steady-state, free precession, self-gated sequence adapted from a previously described technique 11 was used to obtain 500 μm isotropic resolution volumetric images (approximately 26 per cardiac cycle). Raw 3D image sets were imported into RView (Colin Studholme, University of California), de-identified, and provided to a cardiac radiologist for assessment of left ventricular (LV) volumes and ejection fraction (EF). End-diastole and end-systole were determined based on visual inspection of short axis images (Fig. 3). Manual planimetry of endocardial contours from 500-μm thick and short continuous axis slices through the entire left ventricle (18 to 20 per heart) was used to calculate LV volumes.

Cardiac MRI. representative images from MRI data showing examples of short axis LV chamber contours determined at end diastole (
Skeletal myoblast isolation and culture
SKMBs were isolated as previously described. 4 Briefly, donor rats were anesthetized and the soleus muscles were removed and enzymatically dissociated. Cells isolated by centrifugation were plated in laminin-coated dishes (1 μg/cm2, Sigma) and cultured in Ham's F-12 media (Invitrogen, Carlsbad, CA, USA) containing 20% fetal bovine serum (FBS, Invitrogen). After 7 days in culture, the cells were harvested by trypsinization and re-suspended in minimum essential medium (Sigma) at a final concentration of 1 × 10 6 cells/85 μL. This technique yields cells with approximately 95% viability according to trypan blue exclusion and approximately 90% positive labeling with antibodies against desmin, a cytoskeletal protein expressed in myoblasts and myocytes. Only 5% ± 1% of cultured cells showed β-galactosidase activity (Fig. 1C).
Implantation of osmotic pump and skeletal myoblast transplantation
Implantable osmotic intravenous infusion pumps (200 μL, 0.5 μL/h, Alzet, Cupertino, CA, USA) were loaded with human recombinant HGF (2.5 mg/mL, Genentech, San Francisco, CA, USA) in buffer (500 mM NaCl, 20 mM Tris-HCl, dextran sulfate 25 mg/mL) or vehicle control (buffer only) and primed overnight (37 °C) in 0.9% NaCl before implantation. The activity of HGF used in this experiment for promoting SKMB proliferation had been confirmed in a cell culture assay (data not shown). Rats were anesthetized as described above, the left jugular vein was cannulated, and a bolus injection of HGF (30 μg in 500 μL buffer) or vehicle control (buffer only) was administered. The pump cannula was secured in the jugular vein and the pump was implanted subcutaneously. Previous thoracotomy was reopened and SKMB transplantation was performed as previously described. 4 Four injections of 1 × 10 6 SKMBs were performed in a diamond pattern within each infarct (total of 4 × 10 6 cells per animal). Animals were recovered as described above.
Sample collection
Rats were euthanized 2 weeks after SKMB transplantation. Serum was collected for assessment of HGF concentration. The left ventricle was opened longitudinally opposite to the MI, pinned to a dish with the endocardium exposed, and fixed in 2% paraformaldehyde followed by 30% sucrose. Sections (40-μm thick) were cut parallel to the endocardial surface using a freezing microtome. Samples of left ventricular myocardium remote from the infarct were snap-frozen in liquid nitrogen for later mRNA isolation. Remaining fluid in the osmotic pump was collected and quantified.
Hepatocyte growth factor Elisa
Serum HGF levels were quantified using the Quantikine Human HGF Immunoassay kit (R&D Systems, Minneapolis, MN, USA) according to the manufacturer's instructions. A standard curve was generated using recombinant human HGF (Genentech). The assay has a detection limit of 40 pg/mL.
Immunofluorescence and β-galactosidase staining, quantification of infarct size, and skeletal myoblast engraftment
Every fifth section through the ventricular wall was stained for β-galactosidase activity (NovaUltra Special Stain Kit, IHC World, Woodstock, MD, USA) according to the manufacturer's instructions. The same sections were then immunofluorescence double-labeled as described previously 4 with antibodies against skeletal myosin to identify engrafted SKMBs and connexin 43 to identify surviving myocardium. Immunofluorescence staining was quantified using a computerized image analysis system as previously described. 4 Briefly, total infarct area (absence of connexin 43 labeling) and area occupied by engrafted SKMB's (positive for skeletal myosin) was quantified on each section and the corresponding volumes calculated from the entire stack of serial sections.
mRNA isolation and quantitative PCR
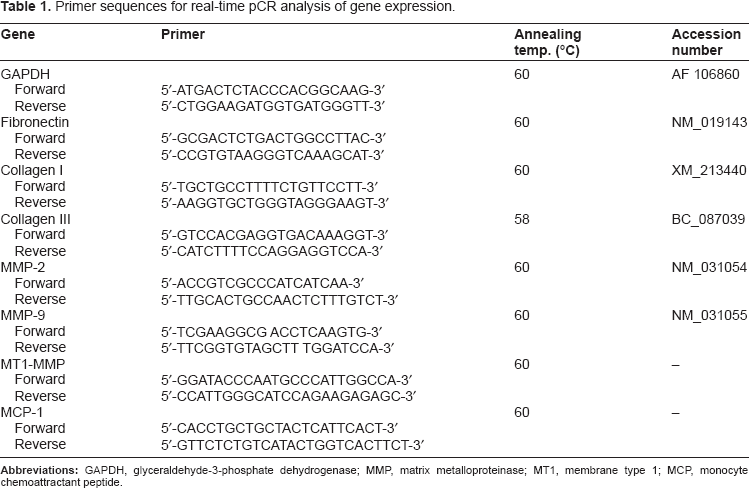
Left ventricular myocardium remote from the infarct was collected and immediately frozen in liquid nitrogen. RNA was extracted using the Aurum Total RNA fatty and fibrous tissue kit (Bio-Rad, Hercules, CA, USA), quantified using the Qubit RNA assay kit (Invitrogen), and reverse-transcribed using the iScriptcDNA synthesis kit (Bio-Rad). Quantitative gene expression was assessed using a CFX96 Real-Time PCR detection system (Bio-Rad) and SYBR Green technology (Bio-Rad). Fibronectin (FN), collagen-I (C-I), collagen III (C-III), matrix metallo-proteinases (MMP)-2 and −9, membrane type 1-MMP (MT1-MMP), and monocyte chemoattractant peptide-1 (MCP-1) gene expression was assessed using the primers shown in Table 1. PCR conditions were optimized for each set of primers. Melting curve analysis showed a single PCR product for each gene amplified. The PCR cycling profile consisted of an initial denaturation at 95 °C for 30 s and 35 cycles of 95 °C (5 s) and 58 or 60 °C (5 s), depending on the primer set (Table 1), for annealing with extension. The housekeeping gene glyceraldehyde 3-phosphate dehydrogenase (GAPDH) was used for normalization. Relative gene expression was calculated using the 2–ΔΔCt method. 12
Primer sequences for real-time pCR analysis of gene expression.
Results
Coronary artery ligation and skeletal myoblast transplantation
Thirty-one rats underwent LAD ligation. Nine (30%) died, either from arrhythmia immediately after ligation or from euthanasia due to respiratory distress in the post-operative period. Twenty-two rats returned to the operating room 4 weeks later for implantation of the osmotic pump and SKMB transplantation. Three animals died intraoperatively due to bleeding during re-thoracotomy and three died during the post-operative period (1 control animal and 2 HGF-treated animals). Two animals showed no evidence of MI and were excluded. A total of 14 rats (7 control and 7 HGF) successfully completed the protocol. Initial weights at the start of the experiment were similar (263 ± 8 g for control vs. 270 ± 8 g for HGF), and weight changes during the experiment did not differ (–8 ± 2 g for control vs. −3 ± 4 g for HGF, P = 0.35).
Hepatocyte growth factor delivery
Based on the amount of residual fluid in the osmotic pumps at the end of the experiment, 192 ± 11 μL of buffer containing HFG was delivered over the 2-week period. Including the initial 30 μg bolus of HGF delivered at the time of pump implantation, the amount of HGF delivered over the 2-week period was 509 ± 28 μg. Serum HGF levels measured by enzyme-linked immunosorbent assay (ELISA) were 6.2 ± 2.4 ng/mL in the HGF group and were undetectable in the plasma of all animals in the control group.
Ventricular dimensions
LV volumes and EF were assessed by MRI before and 2 weeks after SKMB transplantation (Fig 2). LV volumes and EF did not differ between control and HGF groups prior to SKMB transplantation (Table 2). There was no progression in LV dilation during the 2 weeks after SKMB transplantation and slight improvement in LV volumes and EF were generally observed at the second MRI, although the differences were not statistically significant. There were no differences between animals that received HGF and those that did not (Table 2).
Cardiac MRI results.
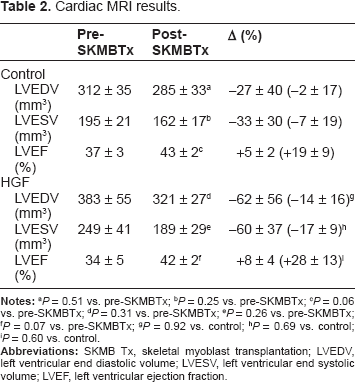
P = 0.51 vs. pre-SKMBTx;
P = 0.25 vs. pre-SKMBTx;
P = 0.06 vs. pre-SKMBTx;
P = 0.31 vs. pre-SKMBTx;
P = 0.26 vs. pre-SKMBTx;
P = 0.07 vs. pre-SKMBTx;
P = 0.92 vs. control;
P = 0.69 vs. control;
P = 0.60 vs. control.
Infarct size and skeletal myoblast engraftment
Two weeks after SKMB transplantation (6 weeks after MI), the volume of the MI scar and skeletal myoblast engraftment were quantified from immunofluorescence labeled histological sections (Fig. 4). The volume of the MI scar was larger in HGF-treated animals compared with in controls (Fig. 5A, 50 ± 7 vs. 30 ± 6 mm3, P = 0.046). MIs occupied a larger area in the HGF-treated group; however, the difference was not statistically significant (Fig. 4B, 54 ± 8 vs. 40 ± 8 mm2, P = 0.24). The volume of engrafted SKMBs detected was low and did not increase following administration of HGF (Fig. 5A, 1.7 ± 0.3 vs. 1.4 ± 0.4 mm3, HGF vs. control, P = 0.58). Similarly, the percentage of the infarct scar occupied by SKMBs did not increase following HGF treatment (4.7 ± 1.9 vs. 5.3% ± 1.6%, HGF vs. control, P = 0.81).
Identification of MI and engrafted SKMBs. (
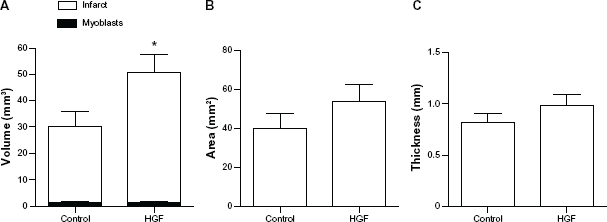
Delivering exogenous HGF did not enhance engraftment of SKMBs. (
Expression of genes associated with post-MI ventricular remodeling
Expression of genes associated with post-MI remodeling19,20 was assessed in LV myocardium remote from the MI (Fig. 6). Expression (2–ΔΔCt) of FN (5.3 ± 0.3 vs. 5.8 ± 0.2, HGF vs. control), C-I (15.4 ± 0.4 vs. 14.7 ± 0.4, HGF vs. control), C-III (3.3 ± 0.2 vs. 3.7 ± 0.4, HGF vs. control), MMP-2 (4.7 ± 0.1 vs. 5.1 ± 0.2, HGF vs. control), MMP-9 (13.7 ± 0.1 vs. 12.7 ± 0.6, HGF vs. control), MT1-MMP (7.3 ± 0.1 vs. 7.7 ± 0.2, HGF vs. control), and MCP-1 (16.6 ± 0.5 vs. 16.3 ± 0.2, HGF vs. control) was not altered by HGF administration.
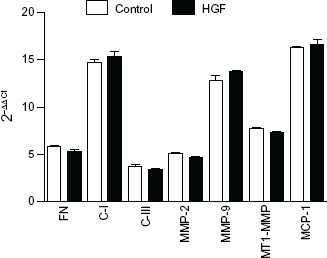
Expression of genes associated with LV remodeling in non-infracted myocardium was not altered by delivery of exogenous HGF.
Comment
In the rat model of MI, infarcts develop into a chronic scar by 4 weeks after coronary ligation. In the present study, we found that SKMBs occupy only about 5% of the MI scar when transplantated 4 weeks after coronary ligation. This result is consistent with our previous report that showed 2.5% of the MI occupied by SKMBs transplanted 5 weeks after MI, which is a 95% reduction in engraftment compared to when the same number of SKMBs were transplanted in the setting of an acute MI. 4 McCue et al also reported that only a small percentage of SKMBs transplanted 1 month after MI in rabbits can be identified in the heart. 13 In humans, only about 1% of SKMBs transplanted into chronic MIs can be identified through histologic examination. 14 The limited engraftment observed when SKMBs are transplanted into a chronic infarct scar may explain the modest benefit observed in clinical trials.3,5 Because of the time required to expand autologous SKMBs in culture before transplantation, it is not practical to perform transplantation very early after MI. Therefore, strategies for augmenting engraftment in the setting of chronic MI are necessary for enhancing the clinical impact of this therapy.
In our previous study, we found that the extent of myoblast engraftment correlated with HGF immuno-reactivity in the MI scar, which declined over time. HGF plays an important role in mediating repair of skeletal muscle by SKMBs.6–9 HGF promotes SKMB proliferation in vitro4,15 and protects against hypoxia and oxidative stress,4,16 conditions that are present in MI and heart failure.16–18 We therefore hypothesized that delivery of exogenous HGF would enhance engraftment and positively influence LV remodeling. However, we found that delivery of exogenous HGF did not enhance the extent of SKMB engraftment when SKMBs were transplanted late after MI. There was also no impact on ventricular function, and the expression of genes associated with post-MI ventricular remodeling19,20 in the remote un-infarcted myocardium was not altered. In fact, MI volume was somewhat larger in the HGF group, but this is likely related to variability in the size of the initial infarct rather than an adverse impact on remodeling by HGF. Ventricular dimensions were stable during the two week period following SKMB transplantation and were not affected by HGF.
Our results are in contrast with those of Tambara et al in which HGF was delivered locally by sustained release matrix placed at the time of transplantation of 5 × 10 6 skeletal myoblasts 4 weeks after MI (21). In control animals, the volume of SKMB engraftment was similar to that observed in our study (5 ± 0.7 mm3). However, with the addition of local HGF delivery, Tambara et al observed an approximately 7-fold increase in the volume of engrafted SKMBs, whereas we found no impact of HGF delivered systemically. While it is possible that neonatal SKMBs used in their study behaved differently than the more clinically relevant adult SKMBs used in our model, it is also possible that the route of HGF delivery is important. In the setting of MI, systemic delivery may not provide adequate tissue concentrations of HGF within the infarct scar. Poppe et al examined the effect of transfected neonatal SKMBs overexpressing HGF on LV function and infarct size following transplantation 2 weeks after coronary ligation. 22 Consistent with our results, they found that transfecting SKMBs overexpressing HGF had no impact on ventricular function after transplantation. However, SKMB engraftment was not quantified in the study. It is possible that had we chosen a local delivery method to target the transplanted SKMBs with HGF, we would have observed an impact on engraftment rate.
We used a dose of HGF based on a previously reported protocol in which human recombinant HGF was delivered in rats at a dose of 100 μg/kg/day for 14 days by osmotic intravenous pump, which was associated with a biological effect in a model of kidney disease. 23 While it is possible that a higher dose of HGF would alter our results, high concentrations of HGF are known to have a negative impact on myoblast proliferation by inducing myostatin expression. 24 Yamada et al demonstrated that HGF concentrations of 2.5 and 10 ng/mL have a positive influence on SKMB proliferation; however, beyond this dose range, SKMB proliferation is reduced. 24 The HGF concentrations used in our experiment (6.2 ± 2.4 ng/mL) appear to be in the optimal range.
Conclusions
In summary, delivery of exogenous HGF by intravenous infusion did not enhance engraftment of adult SKMBs transplanted in the setting of a chronic MI scar or positively impact LV remodeling. This finding is in contrast with a previous report demonstrating that local delivery of HGF does enhance engraftment of fetal SKMBs transplanted into MIs of a similar age. It appears that alternative strategies for enhancing engraftment of adult SKMBs in the setting of chronic MI will be required to optimize the potential clinical impact of this therapy.
Author Contributions
Conceived and designed the experiments: SO, AL, CB, DD. Analysed the data: SO, AL, CB, DD, MA, JC. Wrote the first draft of the manuscript: SO. Contributed to the writing of the manuscript: SO, AL, CB, DD, MA, JC. Agree with manuscript results and conclusions: SO, AL, CB, DD, MA, JC. Jointly developed the structure and arguments for the paper: SO, AL, CB, DD, MA, JC. Made critical revisions and approved final version: SO, AL, CB, DD, MA, JC. All authors reviewed and approved of the final manuscript.
Funding
This work was funded in part by the Heart and Stroke Foundation of New Brunswick.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.