
Abstract
Introduction
Unlike autoimmune hemolytic anemia (AIHA), literature on the etiological study of non-autoimmune hemolytic anemia (non-AIHA) is scarce. The incidence and prevalence of non-AIHA in different geographic regions are largely unknown perhaps owing to the lack of perspective investigation and different profiles of etiologies from different geographic regions. We aimed to examine the real-world etiology or mechanisms of the non-hereditary non-AIHA from a nationwide population-based administrative claim database in Taiwan.
Patients and Methods
The National Health Insurance Research Database of Taiwan was adopted for this research. The studied population was total inpatient claim records including both pediatric and adult patients, contributed by a population of 23 million insured individuals in Taiwan. From 2002 to 2008, we retrieved 3,903 patients having no pre-existing malignancy discharged after inpatient management for acquired hemolytic anemia, which was defined as coding in discharge diagnoses containing ICD-9-CM code 283. By contrast, ICD-9-CM code 282 and all of the sub-codes are for hereditary hemolytic anemias.
Results
AIHA accounted for 32% of the total cases. Among 2,657 patients with non-AIHA, mechanical or microangiopathic mechanism accounted for 19% of cases; hemolytic-uremic syndrome (HUS) 4%, hemoglobinuria because of hemolysis from external causes such as paroxysmal nocturnal hemoglobinuria (PNH) and march hemoglobinuria 7%, and chronic idiopathic hemolytic anemia or other unspecified non-AIHA 69%. We looked further for specific etiology or mechanism for this group of patients with non-hereditary extrinsic non-AIHA (n = 2,657). The explanatory disease states or conditions were splenomegaly; alcohol use disorder (spur cell hemolysis); heart-valve prosthesis; malignant hypertension; disseminated intravascular coagulation; transfusion reaction; dengue fever-induced hemolytic anemia; direct parasitization; snake, lizard, or spider bite; and Wilson's disease with internal toxin mechanism. All these cases can explain up to 34.6% of all the non-hereditary extrinsic non-AIHA cases. Fragmentation hemolysis (HUS, heart-valve prosthesis, malignant hypertension, and disseminated intravascular coagulation) accounted for 7.4% of non-AIHA hospitalized patients with non-neoplastic disease.
Conclusions
This article is the first one to clearly demonstrate that the non-neoplastic-induced HUS requiring hospitalization cases in Taiwan, which has a population of over 23 million were 110 over a span of seven years, 16 cases per year. Although the etiologies of non-AIHA are well known and described in the literature, this work added the statistical percentages of the various etiologies of non-AIHA in Taiwan.
Keywords
Hemolytic anemia is defined as an anemic state because of a shortened survival of circulating erythrocytes, resulting in a red blood cell survival of less than 100 days. This process results from either intrinsic red blood cell (intracorpuscular) defects or extrinsic red blood cell (extracorpuscular) defects causing acquired hemolytic anemia. Intracorpuscular defects are usually inherited, such as thalassemia major, glucose-6-phosphate dehydrogenase deficiency, hereditary spherocytosis, and sickle cell disease. Acquired hemolytic anemia is often because of autoimmune mechanisms, termed AIHA (autoimmune hemolytic anemia), as in warm and cold agglutinin hemolytic anemia (eg, Coombs'-positive AIHA). Nevertheless, there are many non-autoimmune etiologies causing non-autoimmune hemolytic anemia (non-AIHA), including mechanical destruction (eg, disseminated intravascular coagulation), increased destruction within an enlarged spleen (hypersplenism), systemic diseases, and the action of drugs and toxins that interfere with metabolic pathways in the erythrocytes.
Unlike AIHA, literature on the etiological study of non-AIHA is scarce. The prevalence of AIHA is 17 per 100,000 in Denmark. 1 Nevertheless, the incidence and prevalence of non-AIHA in different geographic regions are largely unknown perhaps owing to the lack of perspective investigation and different profiles of etiologies from different geographic regions. 2
We took advantage of our recent population-based cohort study of acquired hemolytic anemia in Taiwan to explore the real-world etiology or mechanisms of the non-hereditary extracorpuscular (extrinsic) non-AIHA in 2,657 hospitalized patients with non-neoplastic disease. In this cohort, patients with malignancy were deliberately excluded because of the study design.
The National Health Insurance Research Database as described in our previous studies was adopted for this research.3–7 The studied population was total inpatient (hospitalization) claim records including both pediatric and adult, contributed by a population of 23 million insured individuals in Taiwan. From 2002 to 2008, we retrieved 3,903 patients having no pre-existing malignancy discharged after inpatient management for acquired hemolytic anemia, which was defined as coding in discharge diagnoses containing ICD-9-CM code 283, whereas ICD-9-CM code 282 and all of the sub-codes are for hereditary hemolytic anemias.
AIHA accounted for 32% of the total cases (Table 1). Among 2,657 patients with acquired hemolytic anemia other than AIHA, mechanical or microangiopathic mechanism accounted for 19% of non-AIHA cases, hemolytic-uremic syndrome (HUS) 4%, hemoglobinuria because of hemolysis from external causes such as paroxysmal nocturnal hemoglobinuria (PNH) and march hemoglobinuria 7%, and chronic idiopathic hemolytic anemia or other unspecified non-AIHA 69% (Table 1).
Patients hospitalized for main diagnosis of acquired hemolytic anemia categorized further by ICD-9-CM codes. AIHA accounted for about 32% of the entire cohort.

We looked further for specific etiology or mechanism for this group of patients with non-hereditary extrinsic non-AIHA (n = 2,657). The disease states or conditions we were able to retrieve were splenomegaly; alcohol use disorder (spur cell hemolysis); heart-valve prosthesis; malignant hypertension; disseminated intravascular coagulation; transfusion reaction; dengue fever-induced hemolytic anemia; direct parasitization; snake, lizard, or spider bite; and Wilson's disease with internal toxin mechanism (Table 2). All these cases can explain up to 34.6% of all the non-hereditary extrinsic non-AIHA cases.
analysis on the etiology for the non-hereditary extracorpuscular non-AIHA patients (n = 2,657).
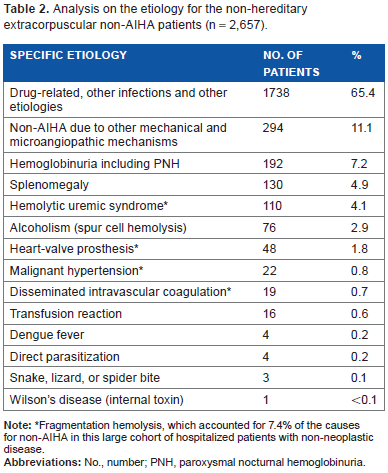
Fragmentation hemolysis, which accounted for 7.4% of the causes for non-AIHA in this large cohort of hospitalized patients with non-neoplastic disease.
In other words, we could postulate that the remaining majority of cases (65.4%) may be drug-related, and others infection-related or just chronic idiopathic non-AIHA despite direct evidence is lacking.8–13
Fragmentation hemolysis (HUS, heart-valve prosthesis, malignant hypertension, and disseminated intravascular coagulation) accounted for 7.4% of this non-AIHA hospitalized patients with non-neoplastic disease.
It is notable that our cases have no neoplastic causes because of prior exclusion criteria set for this cohort. Therefore, one will not expect to find malignancy-induced thrombotic microangiopathy with HUS or malignancy-induced disseminated intravascular coagulation in this series.
Table 2 with a list of a variety of etiology for non-AIHA gives us a mirror to reflect various interesting underlying diseases for the common outcome as hemolytic uremia.
PNH, a stem cell disorder, presents clinically acquired chronic hemolytic anemia in addition to bicytopenia (31%) or pancytopenia (49.5%) in a recent large Asian series. Only 26.1% of PNH in these Asian patients had hemoglobinuria as initial presentation and a little more than half of them got haptoglobin level <0.5 g/L. 14
It is also interesting to look at the spur cell hemolysis. The percentage of spur cells in peripheral blood can predict three-month survival as reported by Vassiliadis et al. The presence of 5% spur cells or more and/or hemolytic anemia is associated with poor prognosis (three-month survival) compared with those of 1-4% spur cells (P = 0.014). 15
This article is the first one to clearly demonstrate that the non-neoplastic HUS cases requiring hospitalization in Taiwan, which has a population of over 23 million, were 110 over a span of seven years from 2002 to 2008, approximately 16 cases per year.16,17 HUS is an uncommon cause of acute kidney injury in children. In contrast to Western countries, Streptococcus pneumoniae is the most common causative pathogen of HUS in Taiwan. 16
Although the etiologies of non-AIHA are well known and described in the literature, the new element added is the statistical percentages of the various etiologies of non-AIHA in Taiwan.
Although ICD-9-CM code-based study did not allow extensive categorization of all etiologies for non-AIHA, it fulfilled the complete separation of acquired hemolytic anemia from congenital form and also possessed an obvious and conspicuous code for AIHAs. Owing to de-identified nature of the database, linkage to individual medical records could not be possible. Therefore, certain risk of allocation bias cannot be completely excluded. Another limitation merits mention was definitive etiology or mechanisms could not be known in 65.4% of non-AIHA patients because the list of drug-related or infection-related etiologies is too huge.
The purpose of this article, in addition to a current etiologic reappraisal, is again to stimulate further large-scale prospective research into the etiology for non-hereditary extrinsic non-AIHA.
Author Contributions
VCK conceived and designed the study, participated in acquisition of data, analysis, and interpretation of data; as well as revised the manuscript and gave the final approval of the version to be published. J-TH, C-KL, C-CL, and F-CS participated in the study design, statistical analysis, and analysis and interpretation of data, and revised the manuscript. All authors read and approved the final manuscript.
Disclosures and Ethics
As a requirement of publication the authors have provided signed confirmation of their compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests.
Footnotes
List of Abbreviations
Acknowledgements
We are immensely thankful to the National Health Insurance Administration, Ministry of Health and Welfare, and National Health Research Institutes, all of Taiwan, for kindly providing the raw data for analysis. The interpretation and conclusions contained herein do not represent those of the above-mentioned institutes (![]() ).
).