
Abstract
A 55 year-old woman presented with abdominal pain. Transvaginal ultasonography demonstrated an enlarged fibroid uterus. She underwent total abdominal hysterectomy and bilateral salpingo-oophorectomy and was found to have torsion of a large pedunculated leiomyoma. There are fewer than 10 cases reported in the literature of torsion of a uterine leiomyoma.
Introduction
Uterine leiomyomata are benign tumors that arise from the smooth muscle cells of the myometrium. Uterine leiomyomata are the most common gynecologic tumors, clinically apparent in approximately 25 percent of reproductive aged women and noted on pathologic exam in approximately 80 percent of surgically excised uteri. 1 Although usually asymptomatic, acute torsion of a pedunculated leiomyoma causing severe abdominal pain is a rare complication and can be a surgical emergency when associated with infarction, necrosis, ischemic gangrene or peritonitis.2,3 To date, there are fewer than 10 cases reported in the literature of torsion of a uterine leiomyoma in non-pregnant women.
Case
A 55 year-old nulliparous woman presented to the emergency room at an outside institution with severe, sudden onset lower abdominal pain associated with subjective fever and nausea. Seven years prior, the patient's primary gynecologist noted an enlarged uterus on physical exam and follow-up sonography demonstrated a 15 cm uterine leiomyoma. Unfortunately, as this initial hospital admission occurred at an outside hospital, we do not have the medical records. However, per the patient's report she underwent a transvaginal sonogram that revealed an enlarged uterus measuring approximately 20 cm. The patient's laboratory values were within normal limits, she was afebrile and appendicitis and other etiologies of acute abdominal pain were excluded. She was admitted for pain management with oral narcotics for presumed leiomyoma-related abdominal pain. Her symptoms resolved and no further evaluation or intervention was pursued. She was discharged on hospital day number 3 with a plan for non-urgent surgical management of uterine leiomyomata.
One week later the patient presented for outpatient follow-up with a gynecologist. She underwent a transvaginal sonogram that demonstrated an enlarged uterus measuring approximately 25.0 × 12.8 × 18.2 cm that extended up to the xiphoid process and contained multiple small leiomyomata (Fig. 1). On physical exam she had an enlarged uterus, measuring approximately 20 cm, however, no abdominal tenderness or other exam abnormalities were noted. She was afebrile and had no leukocytosis (white blood cell count 9.3). The patient was scheduled for a total abdominal hysterectomy and bilateral salpingo-oophorectomy (TAH/BSO).
Transvaginal sonogram demonstrating enlarged uterus measuring approximately 25.0 × 12.8 × 18.2 cm that extends up to the xiphoid process and contains multiple small leiomyomata.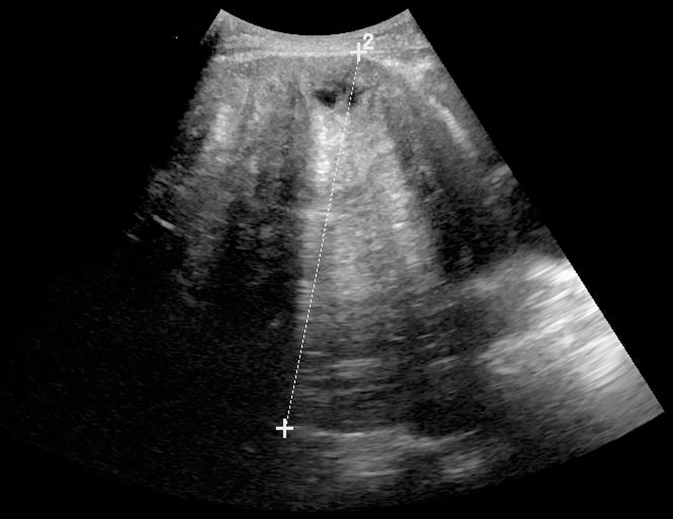
The patient was admitted to our hospital two weeks following the acute episode of abdominal pain for scheduled surgery. During the interim period and upon this hospital admission she reported feeling well, denying further abdominal pain or fever. A laparotomy was performed through a Pfannensteil incision revealing a large necrotic-appearing pedunculated leiomyoma, emerging from the fundus of the uterus and measuring 17.0 × 15.0 × 12.0 cm. When attempting to mobilize the leiomyoma, it was found to be twisted approximately four times around its vascular pedicle, with a small component, measuring approximately 2.0 × 2.0 cm, that was adherent to the sigmoid colon. Adhesions between the large intestine and the leiomyoma were taken down and the leiomyoma was removed using electrocautery at the pedicle. The patient was found to have multiple additional small pedunculated leiomyomata. She underwent an uncomplicated TAH/BSO. According to the pathology report, the leiomyoma weighed 1950 grams with a circumscribed white whorled appearance. There was one region of discoloration with hemorrhage and necrosis. The post-operative course was uncomplicated and the patient was discharged home on post-operative day number 4.
Comment
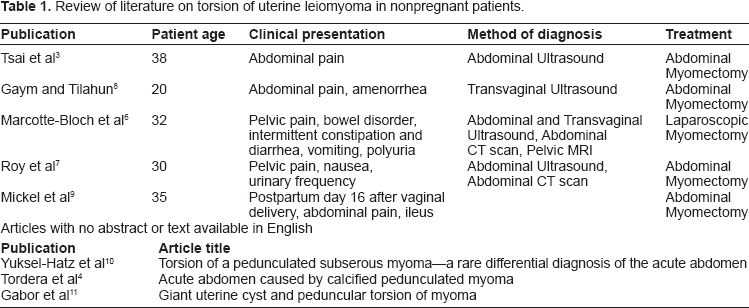
Review of literature on torsion of uterine leiomyoma in nonpregnant patients.
According to the available case reports, torsion of a uterine leiomyoma usually presents as sudden onset severe abdominal pain caused by ischemia of the vascular pedicle. The differential diagnosis for this pain includes ovarian or adnexal torsion, ovarian tumor, necrotic infarction of a leiomyoma and, less commonly, leiomyoma torsion. Transvaginal ultrasound can identify a lesion lateral to the uterus however a definitive diagnosis cannot be made and the pedicle is often too thin for identification with this imaging technique. MRI is considered the best imaging modality for uterine leiomyoma when ultrasound is inconclusive. 5 To date, there are no studies comparing the sensitivity and specificity of MRI to CT for evaluation of torsion of a leiomyoma. MRI may be a better diagnostic technique, however, access to MRI is not widely available, and therefore CT is frequently used. Marcotte-Bloch et al 6 report a case of torsion of a uterine leiomyoma where the pedicle was noted and diagnosis made based on MRI. Roy et al 7 report a case where diagnosis was made based on CT scan demonstration of normal ovaries and contrast enhancement of the uterine portion connected to the mass.
Regarding this case, the patient presented to the emergency room with severe acute abdominal pain and was discharged with resolution of symptoms, however, without a clear etiology for the pain. The diagnosis was not revealed until the time of laparotomy for the treatment of what were presumed to be chronic stable leiomyomata. The diagnosis of torsion of a peduculated uterine leiomyoma was not apparent on transvaginal sonogram, but perhaps a CT scan or MRI at the first hospital visit would have allowed for a more timely diagnosis of her underlying gynecologic pathology. Although she remained asymptomatic after the initial hospitalization, she was at risk for ischemic gangrene, peritonitis and disruption or torsion of the adherent large bowel.
Source
Case report from patient at New York Presbyterian Hospital-Weill Cornell Medical College.
Disclosure
This manuscript has been read and approved by all authors. This paper is unique and is not under consideration by any other publication and has not been published elsewhere. The authors and peer reviewers of this paper report no conflicts of interest. The authors confirm that they have permission to reproduce any copyrighted material.