
Abstract
African-born immigrants comprise one of the fastest growing populations in the U.S., nearly doubling its population size in recent years. However, it is also one of the most underrepresented groups in health-care research, especially research focused on gynecologic and breast malignancies. While the opportunity exists for access to an advanced health-care system, as immigrants migrate to the U.S., they encounter the same health-care inequalities that are faced by the native-born population based on ethnicity and social class, potentiated by limitations of health literacy and lack of familiarity with U.S. health systems. Given the continued influx of African-born immigrants in the U.S., we sought to understand the representation of this population in cervical and breast cancer research, recognizing the population's high risk for these diseases at baseline while residing in their native countries. We determined that there is limited research in these diseases that disproportionately affect them; yet, there are identifiable and potentially modifiable factors that contribute to this paucity of evidence. This clinical commentary seeks to underscore the clear lack of research available involving African-born immigrants with respect to gynecologic and breast malignancies in the existing literature, demonstrate the need for more robust research in this population, and provide fundamental insights into barriers and solutions critical to the continued health of this growing population.
Keywords
Introduction
The inequalities in access to health care for different ethnicities and social classes have been well documented. The unfortunate existence of these inequities affects one of the most vulnerable populations: immigrants. A vulnerable population is defined as a group at increased risk for poor physical, psychological, and social health outcomes and inadequate health care, 1 which may apply to all immigrants, regardless of immigration status. According to estimates from the 2012 American Community Survey, the U.S. immigrant population is just under 15% of the total U.S. population, with growth between 2011 and 2012 of almost one half of a million people. 2 Contributing to the influx of immigrants are the U.S. policies that provide “refuge to persons who have been persecuted or have a well-founded fear of persecution”, through the U.S. refugee and asylum programs. 3 The population admitted in the U.S. through its programs is largely a reproductive-age population, which makes it imperative to have a working understanding of outcomes in their reproductive health, including cancers of the reproductive organs.
In the U.S., African-born immigrants are among the fastest growing immigrant populations compared with other major groups, with a near doubling of its population size between 2000 and 2012 to approximately 1.6 million people according to the U.S. Census Bureau. 4 Also, according to the U.S. Census Bureau, in their 2008–2012 American Community Survey, of the 1.6 million foreign-born immigrants from Africa in the U.S., 36% were from Western Africa, 29% were from Eastern Africa, and 17% were from Northern Africa, followed by Southern Africa (5%), Middle Africa (5%), and other parts of Africa (7%). 5 When considering these regions with the greatest influx, breast and cervical cancer comprise the top two contributors to the cancer incidence and mortality burden, affecting women in these resource-limited countries. 6
Scope of the Problem
Despite the rapid growth in the African-born immigrant population, research involving their health-related issues has been lacking. The limited research that has been conducted involving this population has largely focused on infectious diseases, such as human immunodeficiency virus (HIV) and tuberculosis (TB), while other important chronic diseases, such as screening for the development of malignancies, goes unstudied. 7 The projections for cancer cases in Africa are expected to nearly double to 1.28 million new cancer cases and 970,000 cancer deaths by 2030, simply due to the aging and growth of the population.6,8 Over half a million (527,600) new cases of cervical cancer occur annually, and almost half of the deaths related to cervical cancer (254,374) were in women in less-developed countries.8,9 Of those deaths, almost 25% (60,100) occurred in Africa.9,10
Cervix and breast cancer top the list of leading cancers in women in Africa. 6 There is, however, significant variation in disease burden, with “the highest incidence of HPV infection and cervical cancer found in Eastern and Western Africa”, 11 which from where a significant proportion of the African-born immigrants have come to the U.S. in recent years (Table 1). Access to preventative health measures and improved therapeutic options for cancer care should be easily obtainable and its utilization encouraged in the United States for this population. Although the opportunity exists for access to an advanced health-care system, as immigrants migrate to the U.S., they encounter the same health-care inequalities that are faced by the native-born population based on ethnicity and social class. An understanding of contributors to these health inequities is necessary to positively impact the health of this population. 12
African-born population composition in the U.S. and breast and cervical cancer incidence.
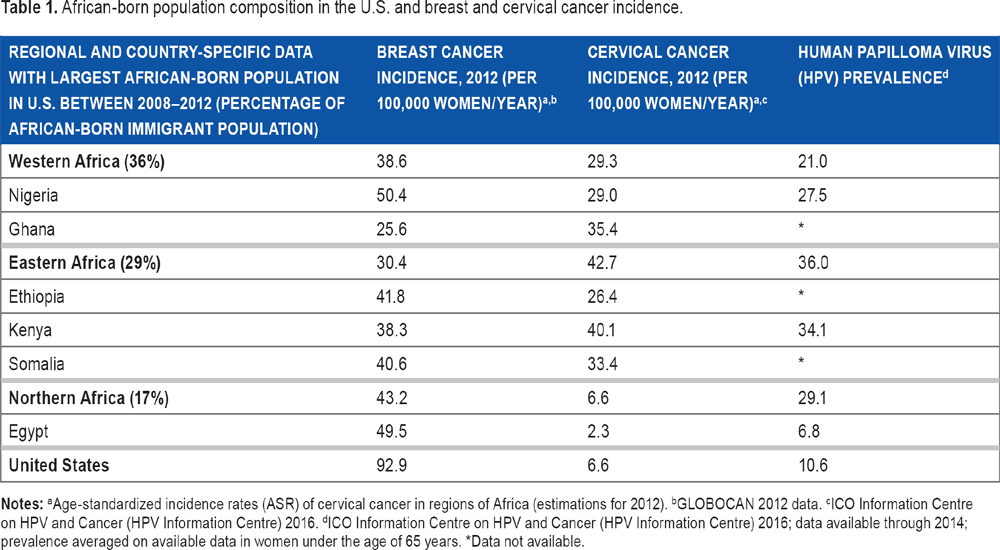
Age-standardized incidence rates (ASR) of cervical cancer in regions of Africa (estimations for 2012).
GLOBOCAN 2012 data.
ICO Information Centre on HPV and Cancer (HPV Information Centre) 2016.
ICO Information Centre on HPV and Cancer (HPV Information Centre) 2016; data available through 2014; prevalence averaged on available data in women under the age of 65 years.
Data not available.
African-Born Immigrants and Barriers to Health
Access to Health Care
In a study of barriers to access to health care for sub-Saharan African refugees in Australia and the UK, it was identified that language barriers, literacy and educational deficiencies, lack of transportation, and limited understanding of the risks of their diseases disadvantaged families in access to care (Table 2).13,14 Additionally, this study of African immigrants in Australia highlighted that unemployment, poverty, and former negative experiences with health-care services in their home countries potentially served as a detractor from seeking health care in their newly settled country. 14
Barriers to utilization of breast and cervical cancer preventative and treatment services in African-born immigrants. a

Based on extrapolated themes from studies utilized within this commentary.
In the U.S., studies focusing on cancer-specific health-seeking behaviors and access to cancer services in African-born female immigrants are limited and utilize small sample sizes and homogenous African populations. A systematic review of U.S. studies showed that barriers to screening for breast cancer echoed views seen in other countries of barriers to access to health care and also identified some new notions not previously discussed: barriers including “shame, modesty, and fear about screening procedures”. 7 Using qualitative data, this study also highlights limited knowledge and familiarity with cervical cancer and screening as important barriers to adherence to screening recommendations, in addition to beliefs of cervical cancer being “the will of God or a curse.” 7 Additionally, if female circumcision had been performed, a custom most commonly practiced in the western, eastern, and northeastern regions of Africa, 15 there was anticipation of embarrassment by practitioners unfamiliar with the practice, 7 leading to poor screening behaviors in women from these regions.
Involvement in Health-Care Research
Understanding the health-seeking behaviors of the African-born immigrant population can largely be accomplished through quality research. Racial and ethnic minority participation in clinical research is paramount, and benefits such as “generalizability of research findings, equity in provision of health care, and accuracy of ethnicity-specific subgroup analyses” have been well established. 16 When considering cancer care research, more than a third of the U.S. population comprises racial and ethnic minorities, but enrollment in the National Cancer Institute's publicly funded cancer clinical trials revealed that less than 18% of participants represented these groups, 17 and there is no clear delineation of how many of those participants represent immigrant populations.
Various perceptions and behaviors of both the researchers and potential participants have been suggested to result in limited involvement of minority groups in research studies. Poor communication by researchers about important aspects of health-related trials, potentiated by the lack of knowledge about cultural differences among ethnic minorities, has been indicated as a barrier to participation in research trials by minorities (Table 3). Furthermore, “psychosocial issues” such as mistrust, fear, and lack of confidence in the research process, in addition to logistical concerns including childcare, schedule conflicts, lack of transportation, and appropriate support, to research-related factors such as lengthy consent documents and lack of adequate information about clinical research hinder racial and ethnic minority participation. 17
Identified barriers to racial and ethnic minority participation in research and potential solutions. a

Summary inclusive of extrapolated themes from systematic review by George et al. 17
In a study of African-born immigrant community leaders and views on African immigrants' participation in genomic research, the study cited “a legacy of colonial mistreatment and exploitation by Western researchers in their home countries in sub-Saharan Africa” as a significant hindrance to participation. 18 A “central dilemma for participants” was the conflict between responsibilities to protect their people from harm and finding solutions for future African generations. 18 An understanding of the behaviors impacting cancer screening, treatment, and follow-up among African-born female immigrants may help to develop important targeted interventions, and this understanding can best be achieved through thoughtful, inclusive, and culturally sensitive research targeted to this population (Table 3). Overcoming these researcher-participant barriers is critical to developing appropriate preventative strategies and interventions and understanding health-related risks in these vulnerable populations.
Breast and Cervical Cancer Research Challenges
Available Breast Cancer Research
There is limited research in the literature focused solely on African-born immigrants and on their screening, treatment, outcomes, and follow-up for breast cancer. In a systematic review of the literature for African-born immigrants and breast cancer, only 10 studies were identified. 7 The research, a mix of quantitative and qualitative studies, focused on breast cancer prevention and detection, barriers to genetic testing, and barriers to mammography screening. These studies, however, were limited by the size of the sample of African-born immigrants present in the study, homogeneity of the study group (e.g. focus on Somali women), and lack of consideration of diversity within African-born populations, such as religion or tribe, immigration status (refugee/asylee), and length of residency in the U.S.
In a study by Vahabi et al 19 of breast cancer screening disparities among Canadian immigrants from several regions of the world including Africa, variables that were significantly associated with low rates of breast cancer screening for all or most regions included “living in low-income neighborhoods, being admitted as refugees, being new or recent immigrants, not having a general physical examination, not being enrolled in a physician enrollment model, having a male physician, and having an internationally trained physician”. Additionally in this study, low rates of breast cancer screening were seen in new immigrants from sub-Saharan Africa (<5 years residence in new country) and recent immigrants (6–10 years residence in new country), and they were noted to be more likely to live in low-income neighborhoods, which coincides with low rates of screening in this demographic. In contrast, the study by Harcourt et al presented data that women who reside in the U.S. for a longer duration were more likely to be screened for breast and cervical cancer. 20 Harcourt et al theorized that women who have spent more time in the U.S. are more likely to be proficient in English and more acquainted with and have better skills in navigating the seemingly complex U.S. health system. 20 They are also likely to be different in respect to cultural factors, including concerns related to modesty and cancer screening knowledge. This theory was born out of other studies looking at access to reproductive health services based on race and ethnicity. 21
Available Cervical Cancer Research
Despite the growing cancer burden in Africa, cervical cancer screening and preventive measures such as HPV vaccination continue to receive low public health priority in the region, largely because of limited resources and other pressing public health concerns, including communicable diseases such as HIV, TB, and malaria. An estimated 11.4% of women with normal cervical cytological findings carry detectable HPV (Table 1), with higher prevalence in less-developed countries like Guinea (47.9%), Kenya (38.8%), Honduras (36.8%), and Mozambique (32.1%). 8 As large numbers of the African population migrate west, those who are HPV carriers also remain at high risk for cervical cancer, despite their new environment due to barriers to health care.
As with breast cancer, research involving the African-born immigrant population and cervical cancer are lacking. A systematic review identified only 11 studies focusing on cervical cancer that included African-born immigrants in the study. 7 Studies included cross-sectional analysis and some qualitative data, although only one study focused on interventions. 7 In one of the reported studies conducted among foreign-born women, authors found disparities in cervical cancer screening based on length of stay in the U.S., with a higher percentage of immigrants residing longer in the U.S., having received screening in their lifetime as compared to recent immigrants; however, only a small population (2%) within the study were actually African-born immigrants. In the study by Harcourt et al, only 52% of African-immigrant women adhered to screening recommendations in the U.S., while screening rates for U.S.-born women surpassed 80%. This study's limitation was defining the study population as Somali or “other African immigrants”, highlighting the lack of heterogeneity and diversity in study samples. 20
Barriers to adhering to screening recommendations were similar to previously cited barriers such as language difficulties, distrust of the interpreters, fear of the test (pain, lack of trust), negative past experiences, and competing priorities and cultural barriers. 7
Discussion
The African-born immigrant population, inclusive of the refugee and asylum-seeking cohort of this population, denotes one of the most vulnerable populations in the U.S.; yet, the understanding of their needs to access health care, particularly in cancer control, is insufficient as evident by the limited research available on this group. Studies that seek to focus on cancer control in black women typically combine data on African-born immigrants, U.S.-born blacks, and black Caribbean women, resulting in extrapolation of potentially misleading data and an application of these outcomes to this underresearched population. American-born “African-American” women in the U.S. have higher rates of mortality and higher percentages of late-stage diagnoses of breast and cervical cancer when compared to other ethnic groups.22,23 Grouping foreign-born blacks with American-born blacks misses important variations within these populations and ignores potential cultural differences between the two populations that may have profoundly different effects on health outcomes.
It is imperative that this population not be ignored, or grouped into categories, and it is equally important to separate African-born immigrants based on region or country and include variables focused on diversity even within these groups, including immigration status and religion. Cultural differences addressed by studying diverse populations within the African-born population as a whole may lead to identification of differences in health-seeking behavior. Research is needed to further understand the factors that encourage or detract from screening recommendations, adherence to treatment, and follow-up care related to cervical and breast malignancy. To date, there are no apparent studies that solely consider adherence to treatment following diagnosis, outcome data, and adherence to follow-up in this population, nor is there an abundance of researched intervention programs targeted to this population.
Achieving inclusive, meaningful research in this population may best be accomplished through multi-institutional collaborations to ensure diversity among African-born populations, and further stratification may delineate risks, behaviors, and associations unique to specific subgroups within these populations. Engagement with community-based organizations that serve these communities may provide a platform for exploring meaningful interventions on health promotion and research in this underrepresented population.
Conclusion
Trends in immigration are not expected to change for this population and may even be expected to rise. The needs of African-born immigrants, refugees, and asylum seekers should emerge as a new public health priority, given the inherent risk to the population based on their native countries, current cancer data and cancer trends, and the continued rise in this population in the U.S. This health-care inadequacy can only be addressed with increasing availability of critical data through research, education of researchers to be mindful of inherent differences in populations and to utilize cultural sensitivity in their research, and active involvement and empowerment of immigrant communities themselves. In doing so, we will widen our health-care safety net to be inclusive of one of the most at-risk populations in the world, increasing in size here in the U.S., and we will potentially decrease disease burden in this population.
Footnotes
Author Contributions
Conceived and designed the experiments: LFP. Analyzed the data: LFP. Wrote the first draft of the manuscript: LFP. Contributed to the writing of the manuscript: LFP, BDN, ME, AG. Agree with manuscript results and conclusions: LFP, BDN, ME, AG. Jointly developed the structure and arguments for the paper: LFP, BDN, AG. Made critical revisions and approved final version: LFP, BDN, AG. All authors reviewed and approved of the final manuscript.