
Abstract
Although poor health-related behaviors that impact development of chronic diseases begin much earlier than when actual disease is evident, few studies have examined health behaviors in college students, who may be at an important transitional period where early intervention could prevent development of chronic diseases. The purpose of this study was to examine health-related factors in female college students (N = 61) by race/ethnicity and weight status. We found significant differences in health profiles between non-Hispanic White (White) and African American students, including greater physical fitness and healthier diets among White students. Overweight/obese students had worse health profiles than healthy BMI students. Furthermore, weight status was significantly associated with cardiovascular fitness. This supports a focus on PA promotion for interventions in the period of emerging adulthood, alongside the other healthy behaviors, to elicit improvements in weight status and potential reduction of chronic disease risks.
Introduction
Obesity is a serious health problem in the United States. The prevalence of obesity among adults has more than doubled since 19761 and is present across all demographic strata of the United States population.2,3 Adults are classified as overweight if they have a body mass index (BMI) greater than or equal to 25 and obese if they have a BMI greater than or equal to 30. 2 The most recent national data show that 34.9% of adults in the United States are classified as obese. 4 Although obesity is prevalent across all sectors of the population, obesity rates are significantly higher in Black and Latino populations, particularly among women. 5 In addition to racial and gender disparities, college students are a demographic group especially at risk for developing obesity. Mokdad et al 6 found that between 1991 and 1998, prevalence of overweight and obesity increased at a higher rate among young adults aged 18–29 years and at an even higher rate among young adults who attended and/or completed a college degree compared to age-matched peers who did not pursue college after high school. The National College Health Assessment II survey classified 31.3% of females and 34.6% of males enrolled in college as overweight or obese. 7 Multiple studies have documented increases in college students' body weight throughout all four years of college education;8,9 a significant portion of the weight gained by students during college years occurs during their first year of school.10–14 In addition to unfavorable weight changes, cardiovascular and muscular fitness and flexibility have also declined in college students in the last two decades, contributing to the rising risks of chronic diseases present in this population. 15 Weight gain among college students is particularly prominent among those living on campus where a lack of parental supervision, an abundance of unhealthy food options, support for physical inactivity, and the advent of stress-related behaviors and sleep deprivation are present in the campus environment.16–19
As demonstrated by the trends, the dramatic change in environment in the transition between high school and college places students at risk of gaining weight in their freshman year. This critical transition period is marked by a decline in healthy behaviors, including a decline in physical activity (PA) levels, 20 adoption of unhealthy eating habits, 18 adoption of unhealthy sleep patterns and practices, 21 and an increase in alcohol consumption. 22 Many factors play a role in college students adopting unhealthy behaviors. Being in a different food environment, often with unlimited quantities of unhealthy food options, coupled with newfound independence over food choices, can lead to consumption of larger quantities of unhealthy foods. 17 Stress stemming from a change in environment and an increase in responsibilities can lead to unhealthy coping behaviors, including the consumption of unhealthy, high calorie foods, and alcohol, in addition to elevated cortisol levels, which is linked to abdominal obesity.16,17,23 Lack of sleep due to studying demands can also contribute to overconsumption of food and beverages. 17 In addition, time management challenges may result in prioritizing school work and social obligations over PA and healthy food choices, leading to declines in PA levels and physical fitness, and a rise in consumption of unhealthy food.15,17 In addition to the short-term decline in healthy behaviors, bad habits formed in the first year of college can have lifetime implications, since they contribute to the development of obesity, a leading risk factor for many chronic diseases, including diabetes, hypertension, high cholesterol, stroke, heart disease, some cancers, and arthritis. 24 Although the effects of unhealthy behaviors may not be readily seen during the college years, research suggests that the poor health characteristics of college students and the continued decline of health behaviors during adulthood can have serious health implications.25–27
To date, few obesity interventions have focused on the college-aged population. 22 To understand how to develop effective interventions for college students, it is important to understand precollege health status and health-related behaviors. The purpose of this study was to examine the relationship between body composition and anthropometric measures, fitness, and health-related behaviors of first-year female college students. Our aims were to investigate differences in health-related factors and behaviors by race/ethnicity and BMI classification and to identify correlations between key health-related factors and behaviors and anthropometric variables (BMI, waist circumference, and body fat percentage [BF%]).
Methods
Participants
Participants (N = 61) were full-time, first-semester, non-Hispanic White (White; n = 31) or Black/African-American (Black; n = 30) female students, 18 years old on average, who lived on campus, reported having no major health issues that would prevent them from participating in the study as intended, and were interested in participating in obesity prevention and health promotion intervention programs. Studies were conducted at two universities in the south-eastern region of the United States—one private, Predominately White Institution (PWI), and the other a public, Historically Black College/University (HBCU). Participants were recruited by word of mouth, at orientation events, via Internet postings and emails to the targeted population, and by recruitment flyers posted throughout campus. The exclusionary criteria for participating in the parent studies included male gender; less than 17 years of age or greater than 22 years of age; reporting a positive history of cardiovascular disease, lung disease, nephropathy, retinopathy, neuropathy, or a musculoskeletal disorder or injury that would prevent successful completion of the exercise tasks; or reporting consuming tobacco products. No participants were excluded from participation based on these criteria. The Institutional Review Board and Human Subjects Research Offices on the campuses of the University of Miami and Winston-Salem State University approved recruitment, testing, and intervention procedures. All participants provided written, voluntary, informed consent prior to participation. Secondary data analyses of de-identified data conducted for the preparation of this manuscript was approved by the Institutional Review Board and Human Subjects Research Office at Winston-Salem State University. Furthermore, this research study complied with the principles of the Declaration of Helsenki.
Procedures
Participants underwent one screening appointment at baseline during the screening phase for the intervention programs that included the collection of demographics, personal contact information and availability for planned intervention sessions, and personal medical history. Participants also completed a comprehensive physical assessment and filled out self-reported measures using standard questionnaires and surveys.
Comprehensive physical assessment
The physical measures were assessed per the protocols described below in the following order: resting heart rate, resting blood pressure, height, weight, waist circumference, BF%, cardiovascular fitness, sit and reach, sit-ups, push-ups, and grip strength. All measures were collected by trained data collection staff.
Resting heart rate: with the participant seated in a relaxed position, heart rate was assessed at the radial pulse for a full minute and recorded as the number of beats per minute.
Resting blood pressure: blood pressure was assessed using an automated device (OMRON® Digital Blood Pressure Monitor; OMRON Healthcare, Inc.), with the cuff wrapped around the participant's right arm after she was seated at rest in an upright position for a minimum of five minutes.
Height and weight: standard protocols were used to measure height, to the nearest eighth of an inch, and weight, to the nearest half pound, with shoes removed. BMI was calculated as weight (kg)/height (m2). 28
Waist circumference: the National Health and Nutrition Examination Survey (NHANES) procedure was used for measuring waist circumference. 28 The waist was measured with a spring-loaded tape (Gulick Tape Measure; G&S Fibreflex) placed superior to the iliac crest and recorded to the nearest centimeter.
BF%: skinfold calipers were used to perform three-site (triceps, suprailiac, and thigh) body composition assessment for females. The American College of Sports Medicine's equations were used to convert skinfold measurements to body density, which was used to estimate BF% based on race/ethnicity for the participants. 29
Cardiovascular fitness test: this submaximal test included a three-minute warm-up at 3.0 mph on a stationary treadmill, followed by a walking speed of 3.5 mph with the grade increased 4% every three minutes, and ended by achieving a heart rate of 85% of age-predicted maximum, or having completed all four predetermined stages. Data from this test were incorporated into the equation to estimate energy expenditure (VO2) at the last completed submaximal stage using the American College of Sports Medicine's metabolic calculation for the estimation of energy expenditure during walking. 29 The VO2 was then divided by the percentage of age-predicted heart rate max at the last completed submaximal stage to estimate VO2 max.
Sit and reach: a standard sit and reach box (Acuflex® I; Rockton) was used to assess hip, hamstrings, and lower back flexibility. The participant was asked to slowly reach with her arms extended as far as she could while her legs were extended and her feet were flat against the box. Three trials were conducted, with the best of three recorded.
Sit-ups: as a measure of abdominal muscular endurance, each participant was instructed to do as many sit-ups as possible in 60 seconds. Participants started with their back and knees flexed, feet on the floor, heels 30–46 cm from the buttocks, and arms crossed over the chest with hands on opposite shoulders. A full sit-up was recorded when participants' elbows touched their thighs. 29
Push-ups: the participant was instructed to perform as many modified push-ups (body rigid and straight, with arms shoulder width apart, and her lower body supported by her knees) as possible until exhaustion to assess upper body muscular endurance. The test was stopped when the participant rested or when the push-up form was compromised. 29
Grip strength: the participant's maximal grip strength in both the left and right hands was assessed by a hand-grip dynamometer (Jamar® Hydraulic Dynamometer; Sammons Preston, Inc.). While standing, with the arm to be tested extended by her side, the participant was asked to grip as hard as possible for a few seconds. 30 Two trials were performed on each hand. The highest combined total was used as her grip strength score, measured to the nearest kilogram.
Questionnaires
Self-report questionnaires were used to assess PA, eating habits, and health behaviors.
International Physical Activity Questionnaire (IPAQ)-short form: the IPAQ is an instrument that assesses walking, moderate, vigorous, and total PA, in addition to sedentary activity across a seven-day period or a usual week. Compared to accelerometer use, the IPAQ has acceptable validity for a self-reported PA measure (ρ = 0.30) and is reliable (ρ = 0.76) in monitoring PA among 18-to-65-year-old participants. 31 The short form was used in this study because there was no reported difference in validity and reliability compared to the long form, and it was more feasible to administer. 31
Eating Attitudes Test (EAT-26): the EAT-26 is a widely used 26-item standardized survey designed to assess eating disorder risk through three subscales (dieting, bulimia and food preoccupation, and oral control). It is highly reliable (Cronbach's α = 0.90 for college-aged anorexia nervosa patients, α = 0.83 for a healthy college female comparison group) and valid in significantly predicting clinical and normal group membership, correctly classifying participants 83.6% of the time. 32
Health behavior survey (HBS): the Physician-Based Assessment and Counseling for Exercise program HBS measures psychological variables related to PA, fruits and vegetables (FV), fiber, dietary fat, and healthy eating. In the college student population, this instrument is considered valid and reliable for examining dietary and weight change displaying a Cronbach's α range of 0.61–0.91.33–35
Statistical analysis
Before analysis, data cleaning procedures were performed. When data were not available at baseline for a participant, the mean score at baseline of all participants for that particular measure was entered, consistent with the intent-to-treat approach that was utilized in the parent studies. Of the overall sample of 86 students recruited for the parent studies, participants who were not White and attending the PWI or Black and attending the HBCU were excluded from analyses (n = 25), a nonprobability, convenience sampling method. Data were analyzed using SPSS 22 for Windows. Significance was set a priori at α of 0.05. Descriptive statistics and independent samples t-tests were used to describe race/ethnicity differences in participant characteristics. The outcome variables included in these analyses were anthropometric variables (weight, BMI, waist circumference, and BF%), fitness variables (VO2 max, sit-ups, push-ups, grip strength, and flexibility [sit and reach]), and health behavior variables (PA-vigorous, moderate, and total per week; EAT-26 total; and HBS-FV servings, fiber intake, and healthy eating score).
To accomplish the first aim of this study, participants were categorized by race/ethnicity (White: n = 31; Black: n = 30) and BMI category (healthy: n = 29; overweight/obese: n = 32). Two-way analyses of variance (ANOVAs) were used to examine the differences in the outcome variables (dependent variables) by race/ethnicity and BMI categories (between-subjects independent variables) and the interaction between the two independent variables. Pearson-product moment correlations were performed between key outcome variables (VO2 max, muscular fitness, PA per week, and diet quality) and anthropometric variables (BMI, waist circumference, and BF%) to satisfy the second aim. All data were checked for compliance of the assumptions using these models, and corrections were applied accordingly. The Bonferroni method was used to correct the alpha level when performing multiple comparisons.
Results
Participant characteristics
As shown in Table 1, participants were a mean age of 18 years old, had normal resting HR and BP, and were of average weight (69.8 kg). Black students had significantly higher resting heart rate and blood pressure and were younger than White students. Although differences were not statistically significant, the average BMI for White students was classified as normal weight, while the average BMI of Black students was classified as overweight. Just under half (48%) of White students and just over half (57%) of Black students were overweight/obese.
Participant characteristics of female college students.

Race/ethnicity and BMI group analyses
The results of the two-way ANOVAs conducted to examine differences in health-related factors and behaviors by race/ethnicity and BMI classification in female college students for the first aim are shown in Table 2. White students had significantly greater mean scores for BF% (P < 0.001, η2 p = 0.335, Mdiff = 6.43), sit-ups (P = 0.009, η2 p = 0.114, Mdiff = 6.32), push-ups (P = 0.042, η2 p = 0.070, Mdiff = 5.52), FV servings (P < 0.001, η2 p = 0.474, Mdiff = 1.7), and fiber intake (P < 0.001, η2 p = 0.246, Mdiff = 0.58). Black students had significantly higher grip strength scores than White students (P < 0.001, η2 p = 0.269, Mdiff = 12.42). As expected, overweight/obese students had significantly greater waist circumference (P < 0.001, η2 p = 0.398, Mdiff = 16.16), BF% (P < 0.001, η2 p = 0.498, Mdiff = 9.02), and EAT-26 scores (P = 0.047, η2 p = 0.067, Mdiff = 3.27) than healthy BMI students. Healthy BMI students performed significantly more push-ups than the overweight/obese students (P = 0.014, η2 p = 0.1, Mdiff = 6.71). There were no significant interaction effects between race/ethnicity group and BMI classification for any variables.
Health-related variable comparisons of female college students by race/ethnicity and BMI classification.

significantly greater than other BMI category; P ≤ 0.05.
As shown in Figure 1, for cardiovascular fitness (VO2 max), White students had significantly higher fitness than Black students (P < 0.001, η2 p = 0.258, Mdiff = 8.79). Healthy BMI students were significantly more fit than overweight/obese BMI students (P = 0.008, η2 p = 0.117, Mdiff = 5.42).
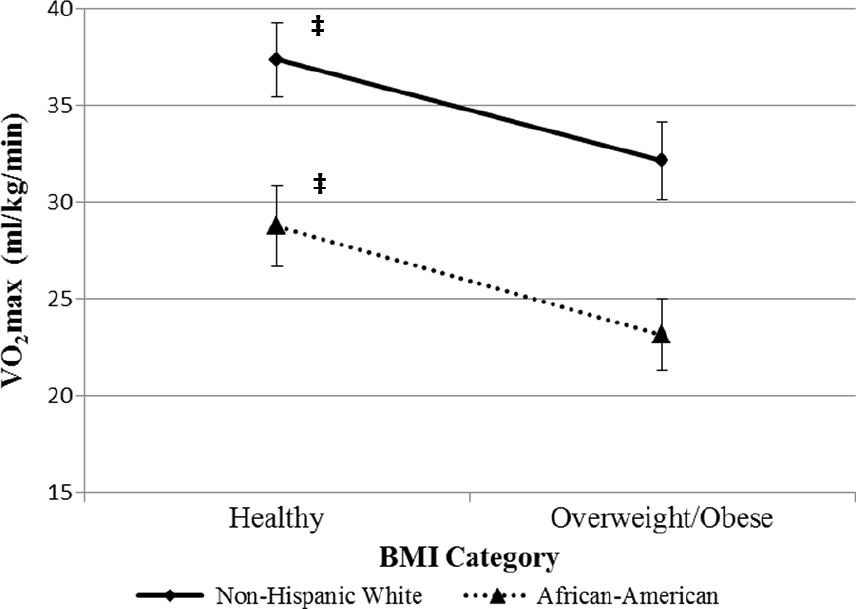
Cardiovascular fitness (VO2 max) by race/ethnicity and BMI classification. Values are mean ± SE. Bold line: significantly greater than other race/ethnicity group and ‡significantly greater than other BMI category; P ≤ 0.05.
Correlation analyses
Pearson-product moment correlations were conducted among the key health-related variables for aim 3. As shown in Table 3, BMI, waist circumference, and BF% were all significantly correlated with each other; however, these measures were not significantly correlated with the other key health-related factors and behaviors. VO2 max was negatively correlated with BMI and waist circumference and positively correlated with diet quality.
Correlation matrix for health-related variables of female college students.

P < 0.001.
Discussion
Although poor health-related behaviors that impact development of chronic diseases begin much earlier than when actual disease is evident, few studies have examined health behaviors in college students, who may be at an important transitional period where early intervention could prevent development of chronic diseases. To our knowledge, this is one of the first published studies to examine the relationship between anthropometric measures, fitness status, and health-related behaviors among female college students upon entering college. To our knowledge, this is also the first study to examine associations stratified by race/ethnicity and weight status. In this study of 61 full-time first-semester female college students, we found significant differences in health profiles between White and Black students, including greater physical fitness and healthier diets among White students. Furthermore, although not all statistically significant, analyses stratified by weight status were all in the expected direction, with overweight/obese students having worse health profiles than healthy BMI students.
In this study, White students demonstrated higher cardiovascular fitness and muscular endurance than Black students, with their significantly higher VO2 max and by performing significantly more push-ups and sit-ups. This may be due to the higher self-reported vigorous PA in White compared to Black students in this study. Vigorous PA is more likely to be performed for the purposes of enhancing health or improving fitness as planned exercise and not likely to be part of routine daily activities. Low-to-moderate intensity activity is not as strongly associated with improvements in fitness levels as routine vigorous PA. 36 These findings are in line with national self-reported data showing higher self-reported vigorous PA and purposeful PA levels among White compared to Black women. 37 The trend for racial/ethnic differences in PA begins during adolescence and has been described in the National Heart, Lung, and Blood Institute Growth and Health Study, which found a 100% decline in PA in Black girls compared to a 64% decline in PA in White girls by year 10 of the study, as the participants reached 18–19 years of age. 38
In addition to having higher fitness compared to Black students, White students also had significantly higher self-reported FV and fiber intake. Through a study of eating habits among 630 White and Black college students, White students reported better eating habits than Black students, consistent with the findings of this study. 39 Despite better health profiles for White students overall, including lower BMIs, White students had significantly higher BF% levels than Black students. While BF% and BMI are highly correlated, BMI is not a true representation of body composition and is not sufficient for describing the distribution of fat versus lean mass in the body. 40 Weight was higher, and BF% was significantly lower in Black than in White students, consistent with the genetic differences that exist between these race/ethnicity groups. Blacks have greater muscle and bone mass and bone mineral density than Whites, explaining both the higher weight and lower BF% found in this sample. 41 Furthermore, hand grip strength in Black students was significantly greater than in White students by a mean difference of over 12 kg. Since grip strength is an indicator of overall strength, 42 this provides additional support for the finding that Black students had less BF% than White students due to greater muscle mass relative to their overall body mass.
In the correlation analyses of the key health-related variables, cardiovascular fitness was the only variable that was significantly correlated with the anthropometric variables. Higher VO2 max was associated with healthier weight status, per the significant moderate negative correlations with BMI and waist circumference. Furthermore, VO2 max was also significantly correlated with diet quality (moderate strength) but not with any of the anthropometric variables. Researchers have reported that diet alone may be used as a viable tool for weight loss; however, the combination of a healthy diet and PA is best for improving anthropometric variables, especially related to preserving lean mass and lowering BF%.43,44 These findings supports a focus on PA in the period of emerging adulthood for obesity prevention, with secondary emphases on diet quality and promotion of other healthy behaviors in this age group, consistent with the recommendation for children and adolescents.45–47 PA resources are typically abundant, yet underutilized, on college campuses, therefore, intervention programs should be designed to emphasize the use of these facilities. If the cardiovascular fitness of college students can be improved through increased PA participation, which may also foster an appreciation and increase in enjoyment of PA, obesity and chronic disease risks may be reduced in this population.
The limitations of this study should be noted. First, students included in this sample were from two college campuses who volunteered to participate in healthy behavior promotion interventions. All White students included in the sample attended the PWI, and all Black students attended the HBCU; thus, data from these samples may not be generalizable to all college students. This study provides an initial glimpse of health-related behaviors and correlates among college students in a small sample; future studies that include larger and broader populations can continue to add to the understanding of health behaviors at early stages in high-risk populations. There were not enough Black students attending the PWI and White students attending the HBCU to make comparisons between campus types in this study, so we could not stratify the sample by university effect or compare Black students attending a PWI with Black students attending an HBCU. Finally, there are known limitations when collecting self-reported data, and this study was not immune to the biases associated with self-report. We used validated surveys and standardized protocols rather than creating our own surveys, which increases the validity of the current findings. In addition, VO2 max was estimated from a submaximal cardiovascular fitness test.
Despite the noted limitations, this study adds to the literature by providing insight about health-related behaviors among first-semester college students. Findings from this study are in line with existing data on adult women, including disparities by race/ethnicity and weight status. Although most chronic disease prevention programs focus on adults >35 years, findings from this study suggest earlier intervention is warranted, particularly in high-risk populations (ie, Black women) where low fitness levels, poor self-reported health behaviors, and high rates of obesity are already present at younger ages (ie, <35 years).
Conclusion
The transitional period between high school and independence during college could be a critical time for intervening on lifelong health habits. This study is one of the first to explore precollege health levels of incoming freshmen, particularly those from populations at highest risk for chronic disease. Future studies should explore natural changes in health profiles among college students throughout the transitional period to understand when and how health profiles are altered. Future studies should also understand specific policies, systems, and environmental factors on college campuses that can positively or negatively impact health behaviors as students transition through the college years. These observational studies can provide the basis for critical intervention strategies that could be implemented on college campuses to provide practical lifelong health-related skills that supplement college-level training in specific academic disciplines.
Author Contributions
Conceived and designed the experiments: AAP. Analyzed the data: AAP. Wrote the first draft of the manuscript: AAP. Contributed to the writing of the manuscript: AAP, MWG, and CLK. Agree with manuscript results and conclusions: AAP, MWG, CLK, and MJM. Jointly developed the structure and arguments for the paper: AAP and MWG. Made critical revisions and approved final version: AAP, MWG, CLK, and MJM. All authors reviewed and approved of the final manuscript.
Footnotes
Acknowledgements
This study was supported by internal funding mechanisms from the University of Miami and Winston-Salem State University. We gratefully acknowledge Kim Price and Bob Jennings for their support and guidance through this process.