
Abstract
This work aims to understand the knowledge and perceptions of women aged over 40 years with breast cancer seen in mastology outpatients at the Maternity Hospital of Huambo, central Angola, from February to August 2010. It also examines the clinical practice of prevention and detection of breast cancer. The research consisted of a collection of descriptive, cross-sectional data through a questionnaire. Statistical analysis of the data was performed using Epi Info, version 6.04b. In our sample, half of the women were single, all had history of breast cancer in the family, and most had heard of breast self-examination, with the primary source of information being the mass media. Almost all women reported that it was important to perform self-examination and that they were aware of the seriousness of breast cancer, and although most of them had not been taught how to do breast self-examination, almost all knew the basics of how to do it. Some 17.6% had heard of mammography, but none had ever had a mammogram.
Introduction
Assessment of the rates of cancer incidence and mortality allows for the forecasting of new cases and mortality rates, enabling better planning of prevention and control programs. Predicting breast cancer is based on the interaction of several factors: genetics, lifestyle, reproductive habits, and environment. 1
Breast cancer is a worldwide problem and is more prevalent among women.2,3
The World Health Organization has estimated that for the year 2030, there will be 27 million new cases of cancer, 17 million cancer deaths, and 75 million people living with cancer each year. The largest increases in reported cancer cases are expected in countries with low and medium income, as these countries improve their health networks and create policies aiming at diagnosis and systematic cancer treatment. 2
The standardized incidence of breast cancer, adjusted for age, reaches 127–128 per 100,000 women in some northern regions of the US and Hawaii, while in China it is only 17 per 100,000, and in Africa, 21 per 100,000. 4 The incidence is highest in North America and Northern Europe, intermediate in the rest of Europe and South America, and lowest in Asia and in less developed countries. 4
According to data from the Surveillance Program, Epidemiology, and End Results of the National Cancer Institute in the United States during the years 1990–2000, the incidence rate of breast cancer was increasing by about 3% per year. The increase in this period was attributed in part to the improvement of screening programs for breast cancer and dissemination of specific information on the cancer-related health system. 5
Studies conducted in Brazil indicated that the likelihood of developing breast cancer was estimated as 0.4% for women 30–39 years old, 1.5% for women 40–49 years old, 2.8% for women aged 50–59 years, and 3.6% for women aged 60–69 years. 6 Its incidence at an early age is usually associated with family history, attributed to genetic factors. 7
Owing to the high incidence, high mortality, and high cost of treatment, breast cancer is considered a public health problem globally. 8 Thus, several programs of primary and secondary prevention have been developed in order to reduce the incidence, and especially mortality related to this disease.
Several factors are associated with either high or low risk of breast cancer. Factors associated with high risk are female, early menarche (before 11 years), late menopause (after 55 years), nulliparity, first pregnancy to term after 30 years, mother or sister with a history of breast cancer, diet rich in animal fat, low-fiber diet, obesity (especially after menopause), and ionizing radiation. Factors associated with low risk are menarche after 14 years, menopause before 45 years, first full-term pregnancy and lactation at less than 30 years old, regular physical activity, and healthy eating habits. 9
Many recent pathology studies, experimental studies, and population-based investigations have been conducted with the aim of defining the risk factors for developing breast cancer, both external, such as fumes and chemicals, and internal, such as genetic mutations, hormonal interactions, and changes in metabolism. These in turn may act alone or in combination, and the time between exposure to the risk factors and the development of cancer can be 2–17 years depending on the state of the person before exposure. 10
Female gender and age are the main risk factors, applying to 77% of cases. Most of the cancers diagnosed in women in the US were diagnosed in women aged less than 50 years. Other risks are attributed to individuals with BRCA1 genes and BRCA2, family or personal history of breast cancer, atypical hyperplasia in the breast, exposure to high doses of radiation, reproductive factors (early menarche, late menopause), nulliparity, first late delivery (after age 30), and absence or short periods of breastfeeding. 10
Cancer is characterized by the abnormal growth of cells. In 2005, of 58 million deaths, 7.6 million were attributed to cancer, representing 13%. 10 Based on the current knowledge, it is virtually impossible to implement primary prevention of breast cancer; early diagnosis offers the only chance of cure. Thus, the myth of prevention is replaced by a reality in which early detection can provide an appropriate and effective therapy.
Early diagnosis of breast cancer results in very large gain for affected women, as it increases the chances of a cure, provides treatment with fewer chances of comorbidities, and decreased costs related to treatment. 9
The disparity in breast cancer incidence and mortality between the developed and developing nations is because of the different levels of knowledge about risk factors for disease, access to effective treatment, and especially the existence of screening and early detection programs. 11
Primary prevention aims to act in the healthy individual, preventing her from acquiring the disease, but this is not yet fully possible because of the variation of risk factors and genetic characteristics that are involved in the etiology of breast cancer. Secondary prevention has as its main strategy population screening by mammographic examination performed at least every two years for women aged 50–69 years, and annual clinical breast exam for women aged 40–49 years. 9 Clinical breast examination should be performed in all women seeking health care, regardless of age, as part of health care for women. For women in population groups considered at high risk for breast cancer (with family history of cancer in first-degree relatives), it is recommended that a clinical breast exam and a mammogram be done annually, starting at 35 years of age. Although there is controversy about the impact of breast examination on morbidity and mortality from breast cancer, in countries with low coverage of screening mammography, clinical examination cannot be overlooked as a means of detection of breast carcinoma. 9
Although considered a relatively good prognosis of cancer, if diagnosed and treated in time, death rates from breast cancer remain high in some countries, most likely because the disease is still diagnosed in advanced stages. 9 About half of the tumors breast cancer are diagnosed in stages III and IV, which may be related to lack of screening programs, including the conduct of the clinical breast examination, annual mammography, and identifying population groups at high risk for developing breast cancer. 12
Scientific evidence suggests that breast self-examination is not efficient for screening and does not contribute to reducing mortality from breast cancer, but is useful to encourage women to examine their own breasts systematically and methodically, so that they discover changes in their breast(s) early. This practice, encouraged because 70% of tumors are detected by the patient, should be done monthly in the ten days after menstruation. 9
Nevertheless, breast examination performed by the woman herself does not replace the physical examination performed by a qualified health professional (doctor or nurse). 3 In cancer care, primary health care is responsible for action at all levels of the natural history and clinical course of the disease, from the promotion of knowledge and prevention to early detection and palliative care. 13
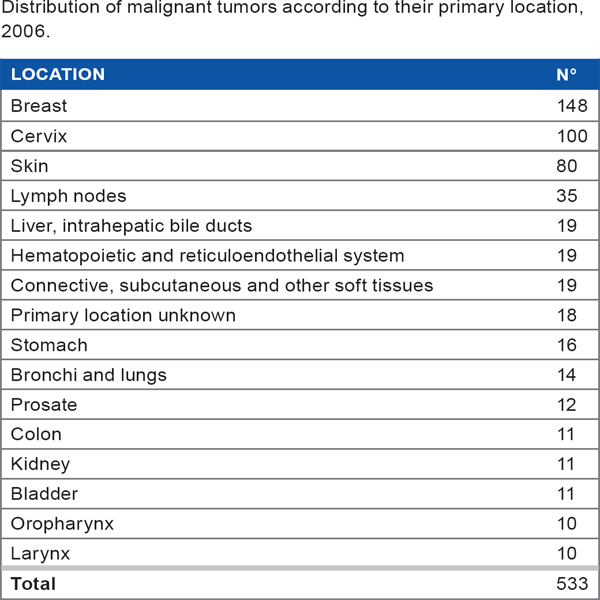
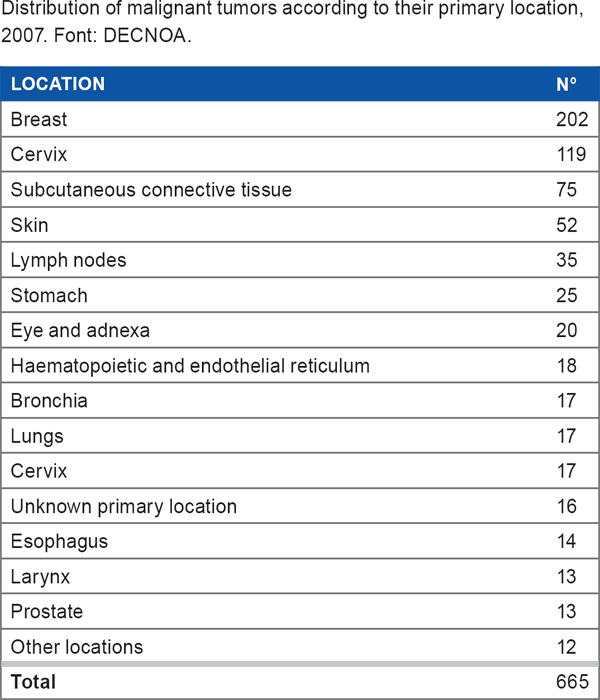
1. During the years 2006 and 2007, the National Oncology Center of Angola diagnoses for breast cancer followed by cervical cancer, and the same organ with primary location.
The reported frequency of breast cancer cases increased at our center between the years 2006 and 2007, probably because of improved means of diagnosis (imaging and histopathology), increased life expectancy of citizens, improvement of health facilities in the country, higher social and academic status of the population, improvement of access roads to the capital, and the end of the war in 2002.
The similarity of the female population in other regions, the Angolan female population has major cancers breast and uterus neck. 14
Methodology
This descriptive, observational, cross-sectional study was conducted in Huambo, Angola, in 2010, based on response data obtained through questionnaires in women users of outpatient visits to the gynecology department at the General Maternity Hospital of Huambo, Angola, over 40 years of age, using survey CAP. 11
Distribution of malignant tumors according to their primary location, 2006.
Unit of Study: General Maternity Hospital of Huambo
Huambo is a province of Angola with an area of 35,771 km2 and a population of ~2.225 million inhabitants. The General Maternity Hospital of Huambois a tertiary unit and receives an average of 130 women daily. It has 80 beds for admissions and performs on average 36 deliveries per day, of which about six are dystocia by cesarean section. The service includes the provision of ten physicians, nine of whom are specialists in gynecology and obstetrics. 15
Distribution of malignant tumors according to their primary location, 2007. Font: DECNOA.
Data were obtained primarily through interviews of outpatients at the mastology department of General Hospital of Huambo, Angola, 40 years of age or older. Women who declined to participate were excluded from the study, as were those who did not respond adequately. The Ethics and Research Committee of the Ministry of Health of Angola approved the study. Participants gave their informed consent to be part of the study, and they were informed that the survey data would be used for research only and anonymity would be maintained at the time of publication of the study.
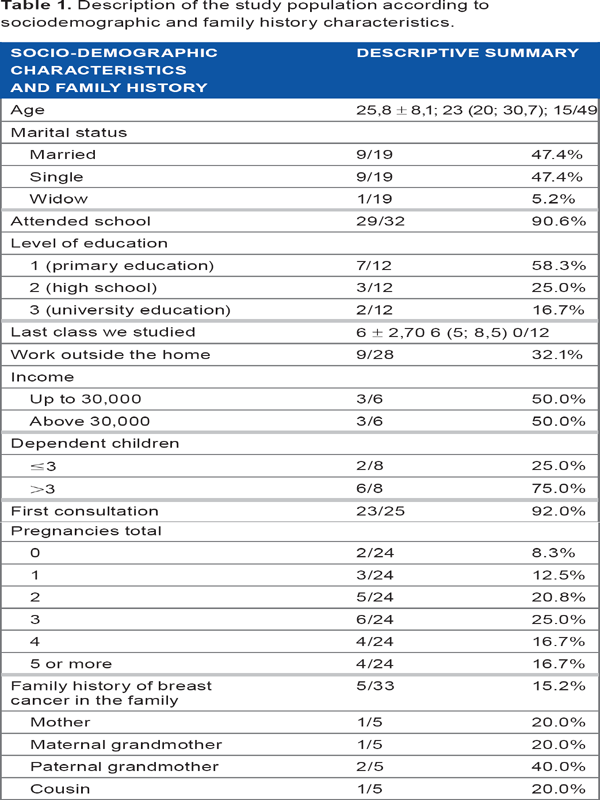
Using a descriptive analysis of frequencies, we found associations between breast cancer and marital status; women living with husbands had more information on breast cancer.
Data processing and analysis were performed with Microsoft Excel and Ep-Info 8.0, version 6.04b, from the Centers for Disease Control and Prevention (2000).
Results
About half of the respondents had heard of self-examination, and ~75% of that group had learned of self-examination through radio or television (Tables 1 and 2). Regarding the statement that self-examination is one way to perceive changes in the breast, 81.2% of respondents believed that the statement was false or did not know whether it was true or false. This lack of knowledge leads us to believe that there is a need for a mastology education program. This situation is the characteristic of developing countries, where the lack of government programs targeting mastology affects patient knowledge levels. Another result that stands out is the significant percentage of respondents with incorrect perceptions about the correct method for breast self-examination. This shows the need for both adoption of public policies and action from health professionals to improve health education in the general population. 16
Description of the study population according to sociodemographic and family history characteristics.
Description of knowledge about breast self-examination.
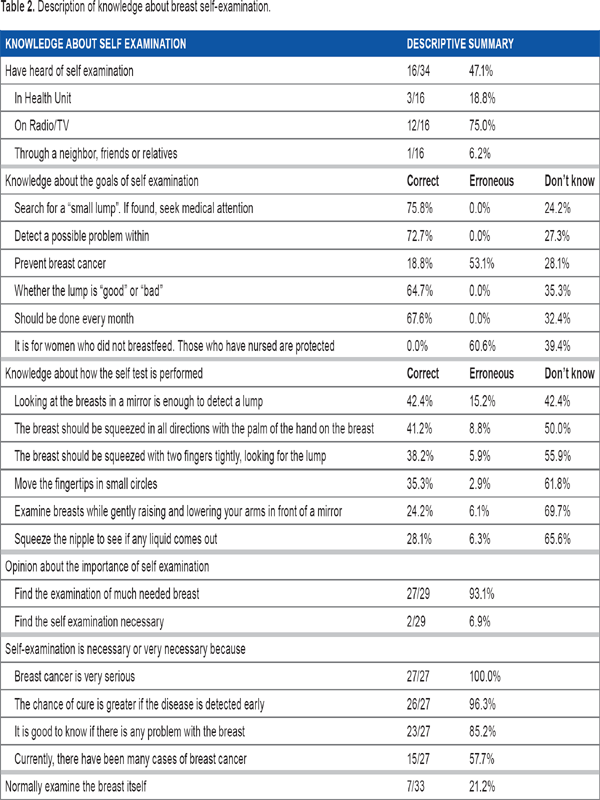
The percentage of women who do not know whether a particular procedure is right or wrong ranged between 42% and 69%. On return visits, it appeared that many were not given instructions regarding how to do self-examinations, and women attending the mastology clinics mostly did not do self-examinations correctly. These results were similar to those found in other studies.11,16,17
Since the available health resources are less than the needs of the population, there is an urgent need for mechanisms to emphasize the importance of breast self-examination. Regarding the importance of the examination, the interviewees showed awareness of the need for self-examination. A relatively low percentage of women usually perform self-examination (22%), and as shown in Table 3, there is evidence of a difference between women who perform self-examination and those who do not, in relation to knowledge of the procedure.
Description of the study population according to the frequency of breast self-examination.
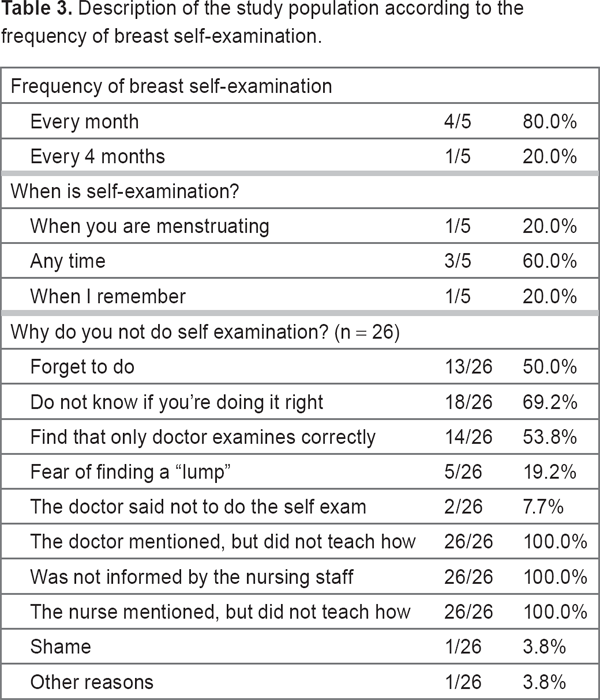
Of the respondents who answered the question related to the frequency of performing self-examination, most reported performing it each month. Those who did not perform self-examinations attributed this to a lack of education from the healthcare team (Table 4).
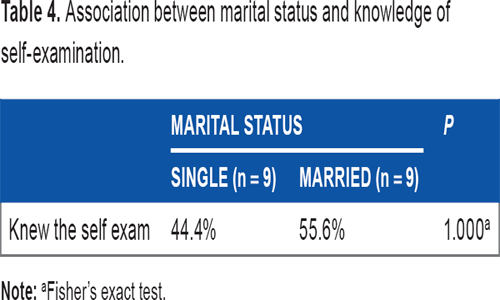
Association between marital status and knowledge of self-examination.
It was observed that a one-year increase in age reduced the chance of ever having heard of self-examination, as follows: OR = 0.84, CI (OR; 95%) test = (from 0.73 to 0.96) (P = 016, Wald chi-square test).
The level of education did not influence the knowledge of self-examination. Among the 10 women with level 1, 28.6% were familiar with the self-examination, while among women the 5 level 2 or 3, 75% had heard of breast self-examination. Although the difference is about 50%, there was not sufficient evidence to conclude that levels of education correlated with a significant difference in levels of knowledge of breast cancer (P = 0.558; Fisher's exact test) (Table 5).
Association between history of breast cancer in the family and knowledge of self-examination.
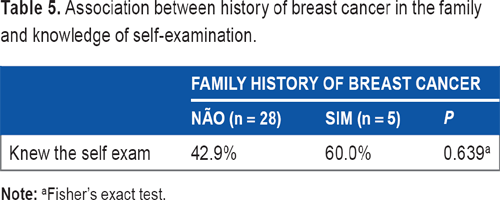
Although there has been evidence that women with a family history of breast cancer are more informed and seek more information about self-examination, we found no evidence of association between having had a history of breast cancer in the family and knowledge of the self-examination (P = 0.639; Fisher's exact test).
Conclusion
Outpatients of the mastology and maternity clinic at the General Hospital of Huambo mostly do perform breast self-examinations. However, health professionals have not taught these patients how to perform self-examination. Self-examination is an important detection technique as mammography is not available in this province, but only in the capital of the country.
Footnotes
Author Contributions
Conceived and designed the experiments: HPT. Analyzed the data: FAN. Wrote the first draft of the manuscript: SBMPT. Contributed to the writing of the manuscript: DPC. Jointly developed the structure and arguments for the paper: HPT, SBMPT, FAN, DPC. All authors reviewed and approved of the final manuscript.