
Abstract
This case report describes a 16-year-old girl with fulminant bacterial meningitis in whom external ventricular drainage and intense volume-targeted therapy (the Lund protocol) was not sufficient to control intracranial pressure, but lumbar drainage on day 8 decreased the intracranial pressure immediately and led to a sustained low intracranial pressure level. The case is unusual and not fully understood, but the authors assume that due to inflammation and tissue reactions following aggressive infection, cerebrospinal fluid could not flow freely from the posterior fossa up to the ventricular drain. High pressure in the posterior compartment maintained the high intracranial pressure measured by the ventricular drain, and lumbar drain insertion caused an immediate fall in pressure. The lesson learned is that during an intracranial pressure crisis in a patient with open basal cisterns, a lumbar drain may be necessary because the cerebrospinal fluid space can be compartmentalized.
Case Report
A 16-year-old girl was brought to the emergency ward at the University Hospital in Reykjavik, Iceland, in a comatose state after an epileptic fit. Her pupils were dilated. A lumbar puncture showed raised intracranial pressure, and bacteriological examination demonstrated growth of Neisseria meningitidis. An emergency computed tomography (CT) scan of the head showed small ventricles, and an external ventricular drain was acutely placed in the right precoronal area. The initial water column was 60 cm in height, but after a while, the intracranial pressure stabilized at approximately 25 cm water.
Intracranial pressure was measured hourly by closing the drainage for 10 minutes and then evaluating the intracranial pressure value. The drain system was kept open to a level of 10–12 cm above the assumed anterior end of the third ventricle. This produced approximately 300 mL of cerebrospinal fluid (CSF) every 24 hours until day 7 when CSF production sharply declined. Resumption of drainage did not restore previous flow of CSF.
The patient was treated on a respirator with normal ventilation and sedation, and drugs were given according to the Lund protocol, including antihypertensive therapy, normalization of plasma colloid osmotic pressure and blood volume, and antistress therapy. 1 A constantly open ventricular drain is not part of the Lund concept. The patient received appropriate antibiotic therapy. The patient was stable, and intracranial pressure, mean arterial pressure, and cerebral perfusion pressure values were acceptable.
Drugs given included: antibiotics (ceftriaxone and later cloxacillin) and an antiviral agent (aciclovir); agents used in the Lund protocol, ie, metoprolol, clonidine, and dihydroergotamine; sedatives (pentothal, fentanyl, and midazolam), and others, including mannitol, furosemide, dexamethasone, indomethacin, and Voluven® (as a volume expander).
On day 7, intracranial pressure rose to approximately 30 cm water and by day 8 the situation was gradually worsening, with further intracranial pressure rises and intermittent dilation of the pupils. Lowering the outflow resistance below the standard height of 10 cm did not change the situation. Repeated CT scans (Figure 1) consistently showed small ventricles.
Computed tomography scan on day 7 showing a part of the ventricular drain coming in from the right.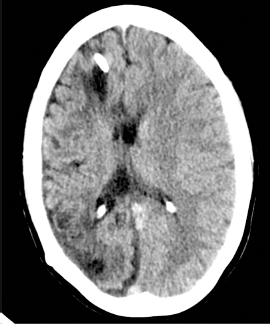
A magnetic resonance examination on day 8 showed considerable ischemic changes in large areas of the right hemisphere and the left occipital region. The basal cisterns were discernable. Radiological examination did not show that intracranial pressure in the posterior fossa was dangerously high (Figure 2).
Magnetic resonance imaging scan on day 8 showing the lower end of the cerebellum at the foramen magnum level.
The clinical situation demanded action. With the patient on her left side, a lumbar drain was inserted in the L3/L4 interspace under sterile conditions. The catheter was then taped upwards along the spine and positioned to join the ventricular catheter, so both drainage systems had the same maximal height and opening pressures. After starting lumbar drainage, the patient's intracranial pressure decreased from 35 cm to about 22 cm water in 2 minutes.
This had an immediate positive effect on the cerebral perfusion pressure, that had been below 60 mmHg. After the procedure, intracranial pressure was under better control, with only two episodes of rise above 20 cm water that responded to medical treatment in the following 2 days; thereafter intracranial pressure was low. On day 21, both drains were removed, with only the lumbar drain being patent. The patient had a ventriculoperitoneal shunt implanted on day 25. At this time, the patient is a happy girl attending school, but with considerable neurological sequelae. In spite of spastic paraplegia she is now out of wheelchair, has a left-sided visual field defect and problems with a spastic bladder.
Discussion
In 2004, Lindvall et al reported their continuous intracranial pressure and cerebral perfusion pressure measurements in patients with bacterial meningitis and raised intracranial pressure. 2 They found that patients with very high intracranial pressure on day 1 usually did not survive, and that those who presented with a moderate rise in intracranial pressure gradually normalized during treatment. Our patient behaved differently, with a very high intracranial pressure on the first measurement but then remained stable, with acceptable values until day 7 when her CSF drainage decreased sharply. Addition of a lumbar drain to an existing external ventricular drain was probably life-saving in this patient.
Lumbar drainage has been described as a tool to be used for raised intracranial pressure in meningitis. In 1986, Thomas et al 3 reported on an 18-year-old girl with acute fulminating meningococcemia and meningitis, coma, shock, disordered coagulation, and extensive purpura who was treated from the outset with lumbar drainage and had a favorable outcome. Further, Macsween et al 4 have described lumbar drainage as an important tool in situations where raised intracranial pressure does not lead to ventricular dilation. They point out the possibility of overdrainage leading to tentorial or tonsillar herniation, or formation of a subdural hematoma. Mobilization of the patient is relatively easy because the drain can easily be clamped or closed temporarily, but it is unclear how much CSF needs to be removed to control symptoms and minimize risk.
Other authors5–8 have described lumbar drainage as a safe and useful tool for dealing with refractory increased intracranial pressure, but all emphasize that this can only be done when there are discernable basal cisterns. There are questions to be asked in this regard, in particular, why was a patent ventricular drain not more productive, assuming constant CSF production, and still measuring a dangerously high intracranial pressure? Intermittent dilation of the pupils confirmed that the values were right. The rapid fall of intracranial pressure when the lumbar drain was inserted supports the validity of the intracranial pressure measurements. We feel that the lesson to be learned is that a lumbar drain may be part of the treatment for an intracranial pressure crisis in which there are open basal cisterns.
Conclusion
Fulminant meningococcal bacterial meningitis is a life-threatening illness. Affected patients are mostly young and may recover to be able to lead independent lives if given optimal treatment. The importance of raised intracranial pressure must always be considered. An external ventricular drain is a simple procedure and gives valuable information regarding the actual intracranial pressure. It also allows the opportunity to lower intracranial pressure by letting out cerebrospinal fluid, and repeated bacteriological examination can be easily performed.
In this paper, we describe a patient in whom lumbar drainage in addition to open external ventricular drainage was necessary to control a late rise in intracranial pressure. We assume that the CSF could not flow freely from the posterior fossa, due to inflammation. High and rising pressure in the posterior fossa was causing raised intracranial pressure by direct pressure on the brain stem. According to the recent literature, performing lumbar drainage may be life-saving in patients with discernible basal cisterns.
Author Contributions
Analysed the data: GG. Wrote the first draft of the manuscript: GG. Contributed to the writing of the manuscript: GG, ASO, HE. Agree with manuscript results and conclusions: GG, ASO, HE. Jointly developed the structure and arguments for the paper: GG, ASO, HE. Made critical revisions and approved final version: GG, ASO, HE. All authors reviewed and approved of the final manuscript.
Funding
Author(s) disclose no funding sources.
Competing Interests
Author(s) disclose no potential conflicts of interest.
Footnotes
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest.