
Abstract
In patients with severe pelvic fractures, exsanguinating hemorrhage represents the major cause of death within the first 24 hours. Recently, multiple management algorithms have been proposed; however, the optimal treatment modalities, in particular, in the hemodynamically unstable patient with pelvic fracture are still a matter of debate. Mechanical pelvic stabilization by pelvic binder, anterior external fixator, and/or pelvic C-clamp constitutes the first treatment option in the hemodynamically unstable patient with pelvic fractures. The mechanically stabilized pelvic ring provides the basis for pelvic packing through a minimal extraperitoneal approach, which effectively controls venous bleeding and bleeding from the fractured bony surface. Patients with persistent hypotension and/or transfusion requirements should undergo angiography and selective embolization for definitive arterial control if necessary. This review article describes the current trend in the initial management of patients with pelvic fractures and hemodynamic instability, and focuses on the role of pelvic packing.
Keywords
Introduction
Pelvic fractures represent a significant challenge for the trauma surgeon in terms of life-threat and functional outcome. An increased recognition of pelvic fractures as a marker of injury severity and improved management algorithms of volume resuscitation, skeletal fixation, and critical care monitoring have done much to advance the care of these often severely injured patients. 1 Nevertheless, the mortality rate still remains significantly high in this patient group; the overall mortality rate of patients with any pelvic fracture ranges between 5 and 10%;2–4 in hemodynamically unstable pelvic fractures, it is up to 60%;5–7 and in patients with open pelvic fracture, it is as high as 70% as a result of complete loss of the self-tamponade effect. 8
In recent years, a wide variety of strategies to treat the hemodynamically unstable patient with pelvic fractures has been proposed.2,9–21 However, there is still no clear consensus as to the best management strategy for these patients. Basically, differences in the trauma system development between Europe and the Anglo-American area have led to different experiences in the management of patients with complex pelvic trauma, and subsequently, to different favored pathways. In the United States, pelvic packing has fallen into disfavor over the recent years, mainly because of the increasing availability of arteriography. In Europe, however, where trauma surgeons are more likely to be orthopedic trained, early pelvic stabilization has been combined with packing techniques. Therefore, two different fundamental treatment modalities have been advocated to address a persistent hemodynamic instability because of pelvic fractures: angiography with sequential embolization controlling arterial hemorrhage versus pelvic packing, which mainly controls venous bleeding and bleeding from the fracture-sites.
This review article describes the current trend in the initial management of patients with pelvic fractures and hemodynamic instability, and focuses on the role of pelvic packing.
Methods
The Medline database was searched for medical literature addressing the initial management of pelvic fractures, in particular in the situation of hemodynamic instability. Search terms included pelvic fracture AND hemodynamic instability AND/OR external fixation and pelvic packing. Specific attention was given to recent, clinically relevant publications focusing on the role of pelvic packing.
Results
Mechanical Stabilization of the Pelvic Ring
There is a substantial agreement that immediate external stabilization of the pelvic ring is the first treatment option in hemodynamically unstable pelvic fracture patients. Fracture reduction leads to a reduction in fracture-site-associated hemorrhage. Furthermore, pelvic ring stabilization plays an essential part in the concept of pelvic packing as only a stable pelvic ring can sufficiently act as an abutment for the pelvic tamponade.
Basically, three methods for mechanical stabilization of the pelvis are available.
Pelvic Binder/Sheet Wrapping.
Pelvic binders, tied around the greater trochanter to apply pressure with internal rotation of the legs, are simple to apply, cost-effective, and of non-invasive character. 22 Biomechanical studies on cadaveric specimens provided evidence of effective pelvic reduction with binders tensioned to 140–200 N in open book or anterior posterior compression injuries.23–25 There has been little study of clinical outcome measures, although there are some data to support improved hemodynamic status with binder use in the immediate resuscitative period. 11 The binder allows lower extremity and abdominal access throughout the ongoing evaluation and resuscitation of the patient; it does likewise not have to be removed while other, more definitive forms of pelvic fixation are applied or inserted. 26 However, with the binder in place, there is restricted access to the small pelvis and femoral vessels for angiography. Therefore, a binder applied in the prehospital or the initial in-hospital resuscitation period should be changed within 24–36 hours into stabilization with an anterior external fixator and/or pelvic C-clamp if pelvic packing is necessary. Further shortcomings of the binder are the risk of skin necrosis and pressure ulcerations as the time of the binder application increases.27,28
External Fixation.
Pelvic fixation with an anterior external fixator is the most frequently available method and is, in particular, efficient in B-type fractures (open book fractures, lateral compression fractures). In C-type fractures (vertical shear fractures), anterior external fixators can stabilize the anterior pelvic ring in addition to a C-clamp. In children, they are generally used for all types of stabilization.29,30 The pins are placed in the iliac crest under direct palpation or in the supra-acetabular bones with fluoroscopic imaging. Placing the pins in the iliac crest is easier than in the supra-acetabular bones; however, supra-acetabular placement is biomechanically stronger and does not interfere with acetabular fracture surgical incisions. Experimental studies have shown that external fixation provides only a small pelvic volume change, and thus, external fixation is thought to contribute to hemostasis primarily by decreasing bony motion at the fracture-site, reopposing the fracture fragments, and thus allowing stable clot formation.31,32 Disadvantages of the external fixation include the inability to sufficiently stabilize the posterior pelvic ring, as well as aseptic pin loosening and pin site infections, which can compromise subsequent definitive open reduction and internal fixation.
Pelvic C-Clamp.
As it has first been described by Ganz et al, the pelvic C-clamp can be used posteriorly for direct reduction of vertically and rotationally unstable fractures. 33 By exerting transverse compression across the sacroiliac joint, the basis for effective pelvic tamponade is achieved.34–37 Ertel and colleagues from the Zurich group reported their experiences in managing multiply injured patients with severe pelvic fracture by application of a C-clamp and pelvic packing following laparotomy.14,15 They concluded that the combination of a pelvic C-clamp and transabdominal pelvic packing can effectively control pelvic hemorrhage in patients in extremis. The use of the pelvic C-clamp, however, is limited to a subset of indications, and requires in C-type fractures often a completion by an anterior external fixator or an anterior plate. In fractures of the ilium and in transiliac fracture dislocations, the C-clamp is not applicable. Pelvic penetration or misplacement through the greater sciatic notch that caused iatrogenic nerve and vascular injuries has been reported. Furthermore, in children, the application of a C-clamp is dangerous and should be avoided. 29
Historical Overview of Pelvic Packing
Historically, open surgical exploration and addressing of arterial bleeding from internal iliac arteries by ligation was advocated in the treatment of severe pelvic fractures. 38 However, as a result of the difficulty in accessing the bleeding arteries and the ineffectiveness because of widely distributed anastomoses, this procedure often produced massive, uncontrollable bleeding resulting in fatalities.4,39–41 Therefore, instead of ligating internal iliac arteries, pelvic packing was employed, which was performed following an exploratory laparotomy when the pelvic hematoma ruptured intraperitoneally.42–44 However, routinely performing a laparotomy in these cases increased the pelvic volume and—by decompression of the retroperitoneum—aggravated the pelvic hemorrhage.31,32 Employing this transabdominal approach for pelvic packing, the potentially intact peritoneum was opened and subsequently disrupted the tamponade effect of the retroperitoneal space. Further concerns mentioned in the literature included the risk of infection in the pelvic hematoma following transperitoneal packing. 41 Finally, packing was often performed late in the course of resuscitation with the patients being already severely coagulopathic, and therefore, packing was essentially a futile maneuver. These reasons led to the general opinion that a fractured pelvis should not be opened to control bleeding.4,40,42
On the other side, in the past decade, the European trauma surgeons have recommended exploratory laparotomy followed by pelvic packing, which was shown in several reports to be particularly successful in patients in extremis.14,15,34,36 Ertel and colleagues reported success in controlling both arterial and venous bleeding by tightly packing the pelvis in 20 multiply injured patients in severe hemorrhagic shock.14,15 The pelvis was posteriorly stabilized by C-clamp in all patients; a total of 14 patients with persistent or massive hemorrhage underwent laparotomy with pelvic packing. Overall, four patients died of exsanguinating hemorrhage in the early course (5.4 ± 3.3 hours from arrival) and one patient died because of septic multiorgan failure 23 days after injury (total mortality, 25%). Similarly, Pohlemann et al retrospectively analyzed 1,899 patients with pelvic fractures and concluded that complex pelvic trauma requires early, aggressive surgical management with surgical hemostasis by localized packing of the pelvis. 36
This European experience incorporated pelvic packing early in the resuscitation course in multidisciplinary, predetermined algorithms. These algorithms considered that pelvic packing is a volume control and pressure-related measure, and therefore, the pelvis itself must be mechanically stabilized in some fashion before packing is performed, otherwise a volume control cannot be achieved. However, these techniques were invasive, with sometimes not insignificant blood loss. To minimize the abovementioned downsides of pelvic packing via the transperitoneal approach, the more controlled, direct preperitoneal and paravesical method has been described, which does not violate the intraperitoneal space and leaves the peritoneum intact as shown below.
Preperitoneal Pelvic Packing
A 6–8 cm midline incision is made from the symphysis pubis extending cranially. The linea alba is incised with the peritoneum left intact. Usually, all parapelvic fascias are already disrupted and direct manual access through the right or left paravesical space down to the presacral region can be achieved without further soft tissue dissection. The retroperitoneal hematoma is then opened anteriorly, and blood and clots are evacuated. The bladder is retracted laterally, and the pelvic brim is carefully palpated and manually dissected. The key is to pack the true pelvis below the pelvic brim, and not the false pelvis above the pelvic brim. The reason is that packing above the pelvic brim has only minimal tamponade effect since the major venous bleeding occurs in the plexus of vessels located in the true pelvis. Care should also be taken to avoid avulsing any vascular connections between the iliac and obturator vessels. After the pelvic brim is palpated as posteriorly as possible, three laparotomy packs are placed sequentially deep to the pelvic brim. The first is placed posteriorly just below the sacroiliac joint, the second sponge is placed anteriorly to the first (in the middle of the pelvic brim), and the third sponge is placed in the retropubic space, deep and lateral to the bladder. When one side is completed, the bladder is retracted laterally toward that side and the other side is packed in the same way. When the acute bleeding is under control, the integrity of the bladder and urethra is inspected. It must be kept in mind that the initial procedure might need to be repeated in order to achieve adequate hemorrhage control. Afterward, the skin incision is closed.4,45,46 Total time for the packing procedure should be less than 20 minutes. The packs are changed or removed after 24–48 hours (Fig. 1).

Infraumbilical incision to perform preperitoneal pelvic packing following mechanical stabilization of the pelvis with pelvic C-clamp and anterior external fixator. The incision was extended to surgically address the completely disrupted urinary bladder.
This modified technique of packing directly addresses the primary source of pelvic bleeding and is different from earlier attempts of direct surgical control. It is quick, relatively easy to perform, and less invasive compared to the transabdominal approach. The value of this treatment concept has led to a paradigm shift in the Anglo-American area in recent years. In multiple case reports and small series, this technique was rediscovered and described.5,47–49
Cothren et al reported on 28 consecutive patients with pelvic fractures and hemodynamic instability; in all patients, external fixation and preperitoneal pelvic packing was performed. 5 The first 4 patients underwent routine angiography (with 1 therapeutic embolization) following direct packing and 4 of the subsequent 24 patients underwent angioembolization because of clinical concern of ongoing pelvic hemorrhage. Importantly, no deaths as a result of acute blood loss were noted. The authors concluded that preperitoneal packing is an effective method to quickly control hemorrhage and serves as a triage tool for emergent angiography.
The same group later compared angiography/embolization versus preperitoneal pelvic packing as different management protocols (20 cases in each group matched by Injury Severity Score (ISS) and age stratifications). 6 They found packing to be as effective as pelvic angiography for stabilizing hemodynamically unstable patients with pelvic fractures. Patients in the packing group underwent operative preperitoneal pelvic packing at a median of 45 minutes from admission; the median time to angiography in the angiography group was 130 minutes. It is noteworthy, that 40% of the patients in the packing group underwent post-packing angiography, while 25% of them required embolization for arterial lesion. The packing group, but not the angiography group, demonstrated a significant decrease in blood transfusion over the next 24 hours post intervention. In the angiography group, two patients died from acute hemorrhage and no patient died from uncontrolled bleeding in the packing group. Thus, the authors concluded that preperitoneal pelvic packing decreases the need for pelvic embolization and post-procedure blood transfusions, and may reduce early mortality because of exsanguination from pelvic hemorrhage. Other authors reported that pelvic packing provided a statistically significant increase in systolic blood pressure immediately after packing. 49
In a recent systematic review assessing the role of pelvic packing as an emergency therapeutic intervention in patients with pelvic fractures and concomitant hemodynamic instability, three studies were eligible and further analyzed (one study with transperitoneal pelvic packing 15 and two studies with preperitoneal pelvic packing).5,49,50 The pooled estimates of effect size for early mortality rate was 10% (95% CI: 3–18%) and for late mortality rate was 13% (95% CI: 5–22%). The authors summarize that pelvic packing, as a part of a damage control protocol, could potentially aid in early intrapelvic bleeding control and provide crucial time for a more selective management of hemorrhage. In two of the three studies included, pelvic angiography played a significant complementary role to pelvic packing for final hemorrhage control.
Disadvantages of Pelvic Packing
There are also, however, disadvantages of pelvic packing. It is a relatively invasive procedure, and it may not be completely effective for control of bleeding from large-bore arteries, especially those ruptured outside the true pelvis. Furthermore, there is the necessity of a reoperation for removal of the packs 24–48 hours following the first operation. However, in most cases, internal fixation of the anterior pelvic ring can be performed at the time of packing removal through the same incision. Some authors have also reported abdominal compartment syndrome as a complication following pelvic packing.15,51
The Complementary Role of Pelvic Packing and Angiography
While vascular lesions in pelvic fractures are thought to be more frequently of venous (90%, mostly lesions of the presacral or prevesical veins) than arterial origin (10%), in cases of hemodynamic instability, arterial lesions are much more frequent and a higher incidence of arterial extravasation is found. Eastridge and colleagues reported that 58.7% of patients with both a severely unstable pelvic fracture and persistent hypotension had arterial bleeding. 7 Likewise, in the study by Miller et al, 67.9% of patients with persistent hemodynamic compromise demonstrated arterial bleeding. 12 However, there are a number of drawbacks to angiography, which, in particular, limit its use in the hemodynamically unstable patient with pelvic fracture. Angiography is a time-consuming procedure precluding the simultaneous performance of other diagnostic or therapeutic interventions. It requires the immediate availability of a skilled interventional radiologist and associated technical staff, and involves the transportation of a severely injured patient to an angiography suite. In one series, 20% of hemodynamically unstable patients with pelvic fractures suffered from cardiopulmonary arrest during angiography and could not be resuscitated. 52 Furthermore, multiple authors have pointed out that considerable delays exist in the performance of angiography (ranging from 50 minutes to 5.5 hours), which may not be tolerated by hemodynamically unstable patients.4,10,13 In a multicenter review of 11 major trauma centers in Australia and New Zealand describing the management practice of hemodynamically unstable pelvic trauma patients, only 14.7% of the pelvic angiographies were performed within 90 minutes of arrival. 53
In the resuscitation phase, immediate and precise identification of the major source of pelvic hemorrhage that is responsible for hemodynamic instability (venous versus arterial bleeding) is not possible. Furthermore, venous bleeding from the fractured bone and the ruptured presacral plexus almost always accompanies severe pelvic fractures. Therefore, considering the abovementioned downsides of angiography, it seems reasonable that pelvic packing should be the first line of treatment for hemodynamically unstable patients with pelvic fractures. During pelvic packing, concomitant injuries can be addressed with damage control techniques (ie, craniotomy, thoracotomy, laparotomy). Patients who demonstrate persistent hypotension and/or transfusion requirements after packing will then need angioembolization for definitive arterial control. Therefore, pelvic packing is an intervention that stabilizes the hemodynamic situation of the patient and then allows the patient to be transported to the angiography suite for selective embolization of arterial bleeding. Furthermore, the packing process may buy time for emergent angiography preparations. Thus, both treatment modalities—pelvic packing and angioembolization—are important techniques to improve patient outcome in bleeding pelvic fractures, and as such, they are not antagonistic but should be seen as complementary.
Initial angiography may be indicated in hemodynamically stable patients or in cases where hemodynamic stability can be achieved with volume replacement but ongoing pelvic bleeding is suspected. However, it is crucial to have in mind that up to 80% of initial hypotensive pelvic fracture patients are non-responders.4,7,12
The Authors’ Approach—The Frankfurt Algorithm
The authors’ general approach to the patient with pelvic fracture is based on the patient's hemodynamic stability and the patient's response to volume resuscitation (Fig. 2, further developed from Ref. 13). 54
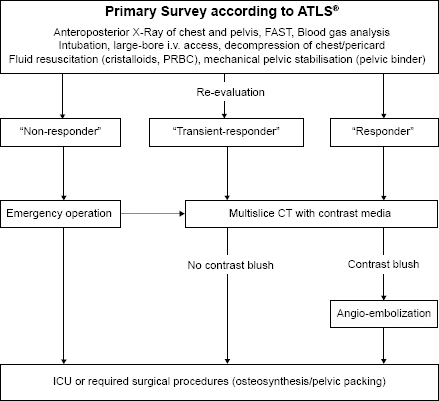
Emergency department algorithm in patients with severe pelvic fracture.
The evaluation of the trauma pattern and the initial management strictly follows the Advanced Trauma Life Support (ATLS®) guidelines. Surgeon-performed focused assessment with sonography for trauma (FAST) is performed in the emergency room upon arrival. Further assessment includes plain radiographs of the chest and pelvis. In parallel, a definitive airway is obtained (liberal intubation in patients with severe pelvic trauma) and a large-bore intravenous access is established (preferably, large-bore central catheters). In terms of volume resuscitation, 2 L of crystalloid solution is immediately administered in the hemodynamically unstable patient with pelvic fracture (systolic blood pressure <90 mmHg). In case of ongoing hemodynamic instability, the transfusion of packed red blood cells (PRBCs) and fresh frozen plasma (FFP) is started. For temporary mechanical fracture stabilization, a pelvic binder is placed on arrival if it has not been done in the prehospital phase. Constant reassessment of the patient's hemodynamic status is performed in order to avoid late recognition of his/her bleeding.
The Non-Responder.
If the patients’ systolic blood pressure remains less than 90 mmHg despite administration of 2 L of crystalloid solution and two units of PRBC, the patient is considered as a non-responder. These patients are not amenable to further diagnostic procedures and undergo urgent exploration, mechanical stabilization of the pelvic fracture (pelvic C-clamp, anterior external fixator), and preperitoneal pelvic packing. During pelvic packing, associated injuries that contribute to mortality, such as intra-abdominal hemorrhage, hemopneumothoraces, and long bone fractures, are simultaneously assessed and treated with damage control techniques. In case of persistent hemodynamic instability with ongoing need of volume resuscitation following definitive packing, ruling out other sources of bleeding by a subsequent angiography is performed in a transiently stabilized patient. If extravasation of contrast is seen, selective embolization with coils or foam is performed. Evidences of vessel spasm or abrupt cutoffs of vessels are likewise seen as signs of injury, and embolization is carried out. If the patient stabilizes after angioembolization, he/she then completes the trauma evaluation, including CT scans and any needed plain radiographs (case report, Fig. 3).

A 54-year-old woman sustained a complex C-type pelvic fracture following fall from 5 m (
The Responder.
Patients adequately responding to fluid boluses and holding the systolic blood pressure >90 mmHg after administration of 2 L of crystalloid solution and, if necessary, two units of PRBC undergo contrast-enhanced CT scan evaluation following the primary survey. In case of contrast extravasation, a pelvic angiography with embolization is subsequently performed with the pelvic binder in place. Patients with ongoing need of volume replacement to achieve hemodynamic stability, with ongoing suspicion of pelvic hemorrhage following angioembolization, or with the need for a mechanical stabilization of the pelvic ring are urgently transferred to the operating room for pelvic stabilization and preperitoneal pelvic packing.
The Transient-Responder.
Similar to the responder, in the patient with at least temporarily achieved hemodynamic stability by volume resuscitation (blood pressure >90 mmHg, however, only with continuous volume replacement), an additional multislice Computed Tomography (CT) scan with contrast is performed and—according to the results—is followed by angiography, surgical damage control procedures, and/or Intensive Care Unit (ICU) admission similar to the responder situation.
Although these treatment algorithms describe the authors’ standard practice in the management of patients with severe pelvic fractures, the care of any patient must be individualized with alteration of this schema for associated injuries.
Conclusions
In hemodynamically unstable patients with pelvic fractures, early exsanguination and the late sequela of shock and massive transfusion represent the major cause of death. The initial decision depends on the shock status of the patient. According to our management protocol, hemodynamically unstable patients (non-responders) are directly transferred to the operating room, where mechanical stabilization of the pelvic ring, pelvic packing, and, in case of ongoing signs of bleeding, a subsequent angioembolization are carried out. The decision whether pelvic angiography or pelvic packing should be primarily performed depends on the careful assessment of the patient's hemodynamic status and the result of the contrast media-enhanced CT scan. Angiographic embolization as a first-line treatment is—in our opinion—reasonable only in transient responders and in responders with an arterial blush seen in the CT scan, indicating acute arterial bleeding. The pelvic binder should remain in place until a definitive surgical stabilization is performed.
Author Contributions
Conceived and designed the experiments: TL, SW. Wrote the first draft of the manuscript: TL. Contributed to the writing of the manuscript: TL, SW, PS, IM. Agree with manuscript results and conclusions: TL, SW, PS, IM. Jointly developed the structure and arguments for the paper: TL, IM. Made critical revisions and approved final version: TL, SW, PS, IM. All authors reviewed and approved of the final manuscript.