
Abstract
Introduction:
In patients with severe pelvic fractures, exsanguinating hemorrhage represents the major cause of death within the first 24 h. Despite advances in management, the mortality rate in these patients remains significantly high. Recently, multiple treatment algorithms have been proposed for patients with severe pelvic fractures; however, the optimal modalities in particular in the hemodynamically unstable patient are still a matter of lively debate.This review article focuses on the recent body of knowledge on the different treatment options in patients with severe pelvic fractures and proposes the possible role of each modality in the management of these patients.
Methods:
The MEDLINE database was searched for medical literature addressing the management of severe pelvic fractures with specific attention given to recent, clinically relevant publications.
Results:
Angiography and embolization have emerged as excellent methods for addressing arterial bleeding. Mechanical pelvic stabilization and surgical hemostasis by pelvic packing, on the other hand, may effectively control venous bleeding and bleeding from the fractured bony surface. However, since there is no precise way to determine the major source of bleeding that is responsible for the hemodynamic instability, controversy remains over the timing and optimal order of angiography, mechanical pelvic stabilization, and packing.
Conclusions:
The author’s own approach to these patients includes angiographic embolization as a first-line treatment only in hemodynamically stable patients with an arterial blush seen in the computed tomography scan, indicating acute arterial bleeding. Hemodynamically unstable patients are immediately transferred to the operating room, where pelvic packing and mechanical stabilization of the pelvic ring are carried out. Optionally, a subsequent postoperative angio-embolization is performed if signs of further bleeding remain present.
Keywords
Introduction
Pelvic fractures represent a significant challenge for the trauma surgeon in terms of life-threat and functional outcome. The complex anatomic relations that exist within the bony pelvis put a myriad of structures at risk when the pelvis is broken. An increased recognition of pelvic fractures as a marker of injury severity, as well as improved algorithms for resuscitation, skeletal fixation, and critical care monitoring, has done much to advance the care of these often severely injured patients (1). However, the mortality still remains significantly high; the overall mortality rate of patients with any pelvic fracture ranges between 5% and 10% (2–4), in hemodynamically unstable pelvic fractures, it is up to 60% (5–7), and in patients with open pelvic fracture as high as 70% as a result of the loss of the self-tamponade effect (8).
While, in recent years, a wide variety of strategies to treat the hemodynamically unstable patient with pelvic fractures have been proposed (2, 9–18), there is still no clear consensus as to the best management strategy for these patients. Basically, two different fundamental treatment modalities have been advocated to address a persistent hemodynamic instability due to pelvic fractures: angiography with sequential embolization controlling arterial hemorrhage versus pelvic packing, which mainly controls venous bleeding and bleeding from the fracture sites. However, the establishment of gold standard treatment guidelines is difficult due to the associated multisystem injury pattern in these patients.
Methods
This review article describes trends in the initial management of hemodynamically compromised patients with severe pelvic fractures, including the evolving concept of pre-peritoneal pelvic packing and angio-embolization. The MEDLINE database was searched for medical literature with specific attention given to recent, clinically relevant publications.
Results
Identifying Pelvic Hemorrhage
Early identification of those patients with pelvic fractures who are at highest risk for pelvic bleeding is imperative. In general, patients with an injury that increases the bony volume of the pelvis (“open book fractures”) are much more likely to have significant bleeding than those with injuries that reduce the volume of the pelvis (“lateral compression fractures”) (1). However, severe bleeding can occur in all pelvic fracture patterns, and, unfortunately, there is a poor correlation between the radiologically estimated severity of the pelvic fracture and the need for emergent hemostasis (2, 3, 10, 15–17). In children, the incidence of life-threatening bleeding from pelvic or acetabular fractures seems to be very low (19). Therefore, the physiological status of the patient rather than the pelvic X-ray should dictate the early resuscitation management. Sequential measurements of base deficit and lactate levels in the early phase may help estimating the severity of pelvic hemorrhage. In the study by Abt et al. (20), base deficit levels measured within 1 h of admission best predicted severe bleeding and early mortality. Salim et al. (21) suggested that a sacroiliac joint disruption, female gender, and the duration of hypotension (systolic blood pressure <100 mmHg) would reliably indicate ongoing bleeding requiring angiographic embolization. Blackmore et al. (22) found an emergency department hematocrit of 30 or less, a pulse rate of 130 or greater, displaced obturator ring fracture, and pubic symphysis diastasis to be good predictors of major pelvic hemorrhage. Miller et al. (15) suggested that patients should be taken to the angiography suite based on the recurrence of hypotension within 2 h of an initially successful resuscitation.
Pelvic Binder/Sheet Wrapping
Pelvic binders, tied around the greater trochanter to apply pressure with internal rotation of the legs, are simple to apply, cost-effective, and of non-invasive character. Biomechanical studies on cadaveric specimens provided evidence of effective pelvic reduction with binders tensioned to 140–200 N in “open book” or anterior posterior compression injuries (23–25). There has been little study of clinical outcome measures, although there are some data to support improved hemodynamic status with binder use in the immediate resuscitative period (11, 26). Croce et al. (11) compared stabilization with a pelvic binder to emergent pelvic external fixation and found a significantly reduced transfusion requirement in the pelvic binder group at 24 and 48 h. Length of hospital stay and mortality were reduced in the binder group, although this did not reach statistical significance. Virtually all the advantages of the pelvic binders can be achieved by using something as simple as a bedsheet; however, a recent study comparing different stabilization techniques found pelvic binders to be superior to sheet wrapping in addressing significant pelvic bleeding (27). In addition, a correct positioning of the pelvic binder has to be performed (28). Downsides of the binder include skin necrosis and pressure ulcerations as the time of the binder application increases. Tissue damage, sufficient to cause pressure sores and skin necrosis, is believed to occur when a contact pressure above 9.3 kPa is sustained continuously for more than 2–3 h (29). This threshold was found to be exceeded at the binder–skin interface at the anterior superior iliac spine, greater trochanters, and sacrum in a study on 10 healthy individuals (30). The polytraumatized patient is likely to be at increased risk of soft-tissue damage due to systemic factors promoting tissue breakdown (31). However, up to now, there is no clear evidence how long a pelvic binder can be safely maintained and how often it should be released periodically to relieve and clinically inspect the soft-tissues.
External Fixation
Pelvic anterior external fixators are easy to handle and can be applied rapidly in 15–20 min by placing the pins in the iliac crest or in the supra-acetabular bones (4, 32). They are in particular efficient in B-type fractures (open book fractures and lateral compression fractures). In C-type fractures (vertical shear fractures), they can stabilize the anterior pelvic ring in addition to a C-clamp. In children, they are generally used for all types of stabilization (33). Experimental studies, however, have shown that external fixation provides only a small pelvic volume change, and thus, external fixation is thought to contribute to hemostasis primarily by decreasing bony motion at the fracture site, re-opposing the fracture fragments, and allowing stable clot formation (34, 35). Disadvantages of the external fixation include the inability to sufficiently stabilize the posterior pelvic ring and pin site infections, which can compromise subsequent definitive open reduction and internal fixation.
Pelvic C-Clamp
The pelvic C-clamp is a specific form of external fixation. As it first has been described by Ganz et al. (36), it can be used posteriorly for direct reduction of vertically and rotationally unstable fractures. By exerting transverse compression across the sacroiliac joint, the basis for effective pelvic tamponade is achieved (37–40). Ertel et al. (12, 13) from the Zurich group reported their experiences in managing multiple injured patients with severe pelvic fracture by application of a C-clamp and pelvic packing. They concluded that the combination of a pelvic C-clamp and packing can effectively control pelvic hemorrhage in patients in extremis (12, 13). In an analysis of 28 patients, Tiemann et al. (41) reported their experience using the pelvic C-clamp for emergency treatment of patients with unstable disruption of the posterior pelvic ring. Overall, seven (25%) patients died. The surviving patients showed blood circulation stabilization as well as consolidation of the oxygenation level 6 h after C-clamping. Five hours after the use of the C-clamp, the number of required blood units decreased significantly (41). The use of the pelvic C-clamp, however, is limited to a subset of indications, and requires often a completion by an anterior external fixator or an anterior plate in C-type fractures. In fractures of the ilium and in trans-iliac fracture dislocations, the C-clamp is not applicable; in children, the application of a C-clamp is dangerous and should be avoided (33).
Pelvic Angiography
Patients who remain hemodynamically unstable after appropriate fluid resuscitation and mechanical stabilization of the pelvis are possible candidates for pelvic angiography. Further indications for performing a pelvic angiography include contrast medium extravasation on the arterial phase of the computed tomography (CT) scan (4, 18, 42). The identification of a contrast blush on the CT scan has been shown to have an accuracy of 98% for identifying patients requiring embolization (43).
While vascular lesions in pelvic fractures are thought to be more frequently of venous (90%, mostly lesions of the presacral or prevesical veins) than arterial origin (10%), in cases of hemodynamic instability, arterial lesions are much more frequent, and a higher incidence of arterial extravasation is found in these instances. Eastridge et al. (7) reported that 58.7% of patients with both persistent hypotension and a severely unstable pelvic fracture had arterial bleeding. Likewise, in the study by Miller et al. (15), 67.9% of patients with persistent hemodynamic compromise demonstrated arterial bleeding. In the early report by Agolini et al. (9), of 806 patients admitted with pelvic fractures, 35 underwent pelvic angiography, and 15 (1.9%) required embolization. Bleeding was successfully stopped in all of the patients embolized. Embolization within 3 h of arrival resulted in a significantly greater survival rate (14% vs 75% if angiography was performed after 3 h) (9). Velmahos et al. (44) recently reported on 100 patients evaluated by angiography for bleeding from major pelvic fractures or solid visceral organ injuries. In total, 80 patients were embolized due to hemodynamic instability, active contrast extravasation, or indirect signs of vascular injury. Angiographic embolization was safe and effective in 95% of these patients (44). Based on these results, early angiography and embolization have been recommended by many authors to improve patient outcome (7, 9, 45).
However, there are a number of drawbacks to angiography mentioned in the literature, and none of the investigators recommend the indiscriminate use of angiography in all hemodynamically unstable patients with pelvic fracture. Angiography is a time-consuming procedure precluding the simultaneous performance of other diagnostic or therapeutic interventions, it requires the immediate availability of a skilled interventional radiologist and associated technical staff, and involves the transportation of a severely injured patient to an angiography suite. In one series, 20% of hemodynamically unstable patients with pelvic fractures suffered cardiopulmonary arrest during angiography and could not be resuscitated (46). Furthermore, multiple authors have pointed out that considerable delays exist in the performance of angiography (ranging from 50 min to 5.5 h), which may not be tolerated by hemodynamically unstable patients (4, 9, 10, 18). In a multicenter review of 11 major trauma centers in Australia and New Zealand describing the management practice of hemodynamically unstable pelvic trauma patients, only 14.7% of the pelvic angiographies were performed within 90 min of arrival (47). Considering these downsides, the question of which patients should undergo angiography and the most appropriated timing of angiography with respect to other treatment options remains a matter of controversy and one of the most difficult aspects of the management in these patients.
Pelvic Packing
For the past decade, European trauma surgeons in particular have recommended exploratory laparotomy followed by pelvic packing (12, 13, 37, 38). The rationale behind pelvic packing derives from the fact that the source of pelvic bleeding in the majority of cases has been identified as predominantly venous. Posterior pelvic ring stabilization with a pelvic C-clamp or an external fixator provides mechanical stability for the pelvic tamponade and fracture reduction leads to a reduction in fracture hemorrhage. Ertel et al. (12, 13) reported success in controlling both arterial and venous bleeding by tightly packing the pelvis. However, the initially described transabdominal approach for pelvic packing included the disadvantage of opening the potentially intact peritoneum with disruption of the pelvic hematoma, and therefore disrupting the tamponade effect of the retroperitoneal space (4). To minimize these downsides of pelvic packing via the transperitoneal approach, the retroperitoneal method has recently been described (48). Not violating the intraperitoneal space and leaving the peritoneum intact, the presacral and paravesical regions are packed from posterior to anterior using three sponges on each side. In the study by Cothren et al. (5), using the technique of pre-peritoneal pelvic packing in hemodynamically unstable patients not responding to 2 units of packed red blood cells (PRBCs), no deaths were reported as a result of acute blood loss. In their study, angio-embolization was only used in 4 of 24 non-responders as a rescue intervention after everything else has failed. They concluded that packing is an effective method that can quickly control pelvic bleeding and can serve as a triage tool for emergent angiography (5). In a study of 40 hemodynamically unstable patients with pelvic ring fractures, external pelvic fixation in combination with direct retroperitoneal pelvic packing effectively stabilized the hemodynamic situation and significantly reduced post-procedure blood transfusion (6).
There are, however, as well disadvantages of pelvic packing. Compared to angiography, it is a relatively invasive procedure, it may not be completely effective for control of bleeding from large-bore arteries, and there is the necessity of a reoperation for removal of the packs 24–48 h following the first operation.
Pelvic Angiography Versus Pelvic Packing
It is difficult to compare the effectiveness of pelvic angiography and packing, mainly because the published reports included patient cohorts with different severity and complexity of their injuries. In particular, the patients undergoing pelvic packing represented a group of extremely unstable patients with massive pelvic bleeding. However, both treatment modalities are important techniques to improve patient outcome in bleeding pelvic fractures, and they are not antagonistic but should be seen as complementary. Our own experience shows that ongoing signs of bleeding following pelvic packing and mechanical pelvic stabilization indicate the need for a pelvic angiography on the way from the operating room to the intensive care unit (ICU) (manuscript in preparation). Angio-embolization of small bleeding arteries will then stop blood loss definitely as indicated in an illustrated case (Fig. 1).
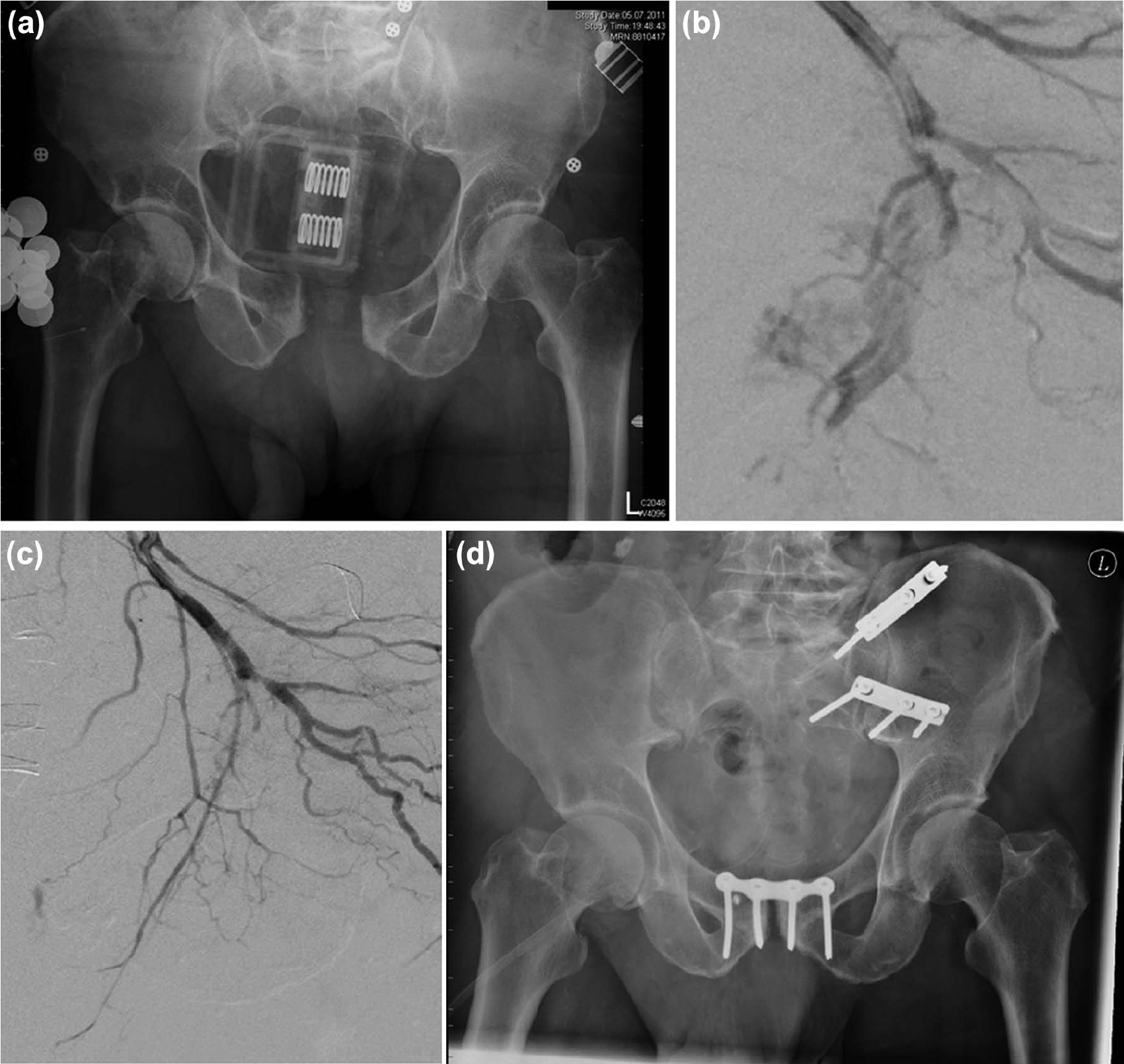
(A) A 74-year-old man sustained a complex pelvic trauma with an anterio-posterior compression and vertical shear injury. A pelvic sling was placed in a local hospital. Within 1 h of the accident, the patient arrived in severe hemorrhagic shock in the level-I-trauma center. Mechanical stabilization of the pelvis was performed by posterior application of a pelvic C-clamp and an anterior external fixator. Retroperitoneal pelvic packing and a suture of the urinary bladder were carried out additionally.(B) Due to signs of further slow, but continuous bleeding postoperatively, a selective pelvic angiography was performed and demonstrated multiples contrast blushes from bleeding branches of the internal iliac artery. (C) Following superselective embolization, the patient was hemodynamically completely stable. (D) The definitive pelvic osteosynthesis was carried out on hospital day 6.
The Hemodynamically Unstable Patient: Abdomen or Pelvis First?
Severe pelvic fractures commonly occur in association with other significant injuries, in particular in the abdomen. In the study by Ertel et al. (13), analyzing 41 patients in an “extremis” clinical condition, 61% of the patients demonstrated concomitant abdominal injuries. Therefore, the hemodynamically unstable patient with a severe pelvic fracture presents a particularly difficult dilemma with regard to the determination of intra- versus retroperitoneal blood loss. In unstable patients with a positive focused assessment sonography for trauma (FAST) exam, it is prudent to perform a laparotomy to treat intra-abdominal bleeding, however, having in mind that performing a laparotomy may increase pelvic volume and directly aggravate pelvic hemorrhage due to the decompression of the retroperitoneum. Nevertheless, clearly, not all intra-abdominal injuries require emergency laparotomy and retroperitoneal blood in the FAST exam should not automatically lead to a laparotomy, as retroperitoneal hematomas often come from the pelvic fracture. Some authors, therefore, recommend the use of diagnostic angiography to identify ongoing blood loss and to achieve hemostasis with embolization. However, this is only possible in hemodynamically stable patients. Angiography is usually not indicated in patients in uncontrolled hemodynamic conditions where immediate surgical interventions are required. In these combined situations, laparotomy and pelvic packing should be performed which further allows the simultaneous assessment and treatment of abdominal injuries. In the presence of multiple massive bleeding points, tamponade of these areas or even temporary aortic compression can be carried out (14). Furthermore, a closure of the abdomen in order to close both compartments at least temporarily seems wise.
The Author’s Approach—the Frankfurt Algorithm
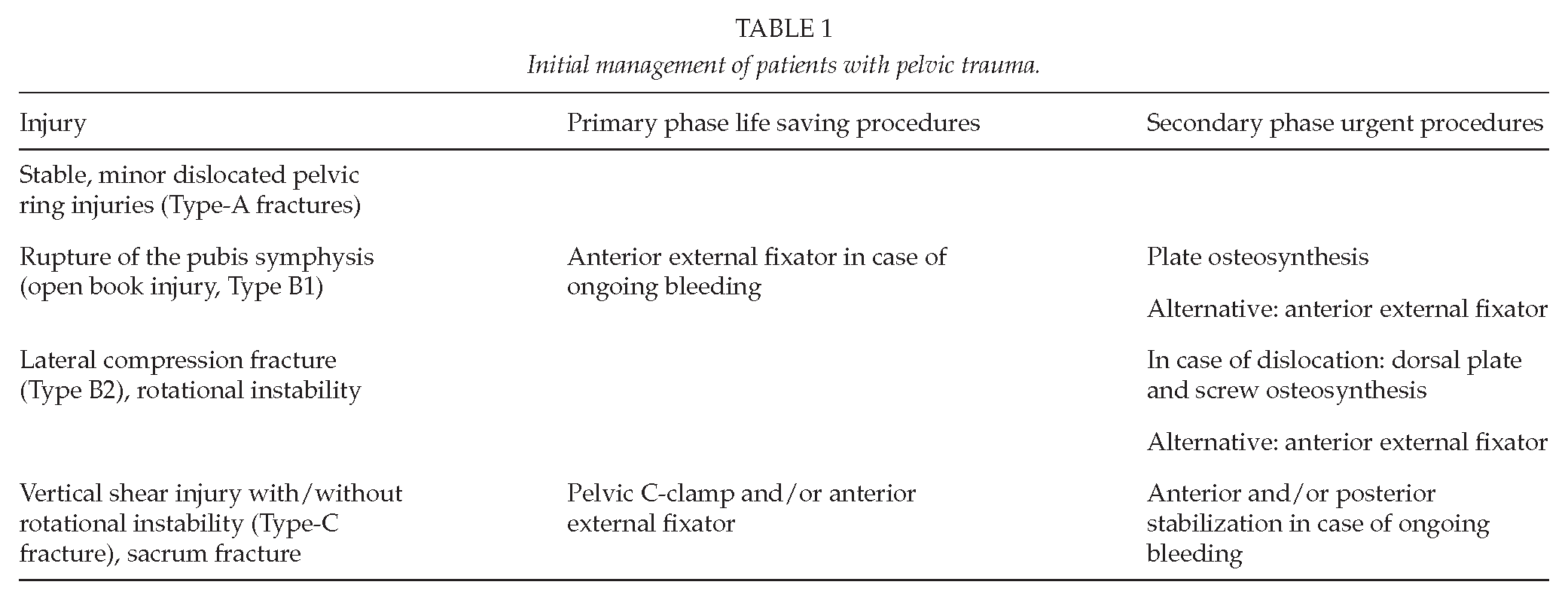
The author’s general approach to the patient with pelvic fracture is based on the patient’s hemodynamic stability and the patient’s response to volume resuscitation (Fig. 2, further developed from (18) considering the type of pelvic fracture additionally (Table 1)).
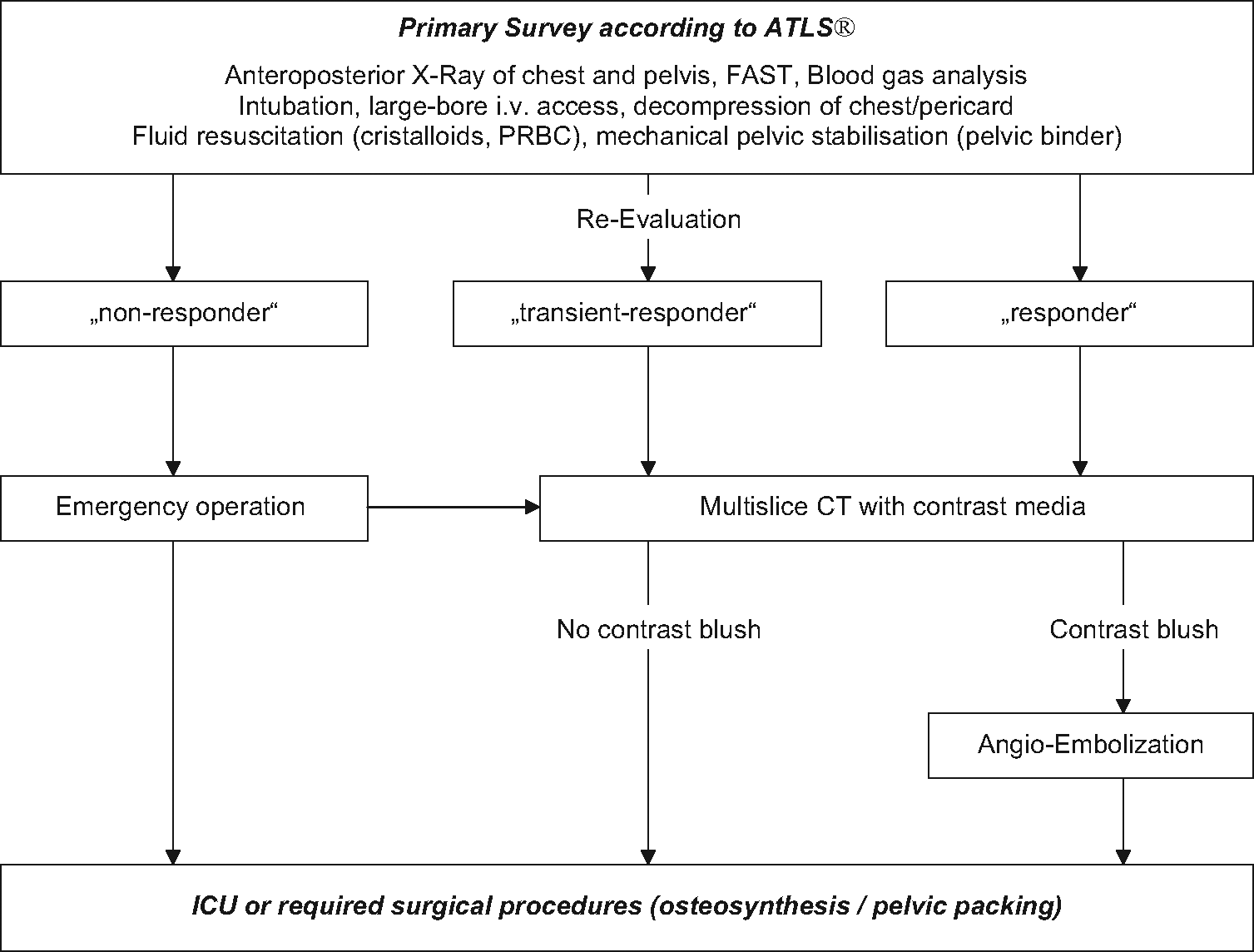
Emergency department algorithm in patients with severe pelvic fracture.
Initial management of patients with pelvic trauma.
The evaluation of the trauma pattern and the initial management strictly follows the Advanced Trauma Life Support (ATLS®) guidelines. Surgeon-performed FAST is performed in the emergency room upon arrival. Further assessment includes plain radiographs of the chest and pelvis. In parallel, a definitive airway is obtained (liberal intubation in patients with severe pelvic trauma) and a large-bore intravenous access is established (preferably large-bore central catheters). In terms of volume resuscitation, 2 L of crystalloid solution is administered followed by PRBCs and fresh frozen plasma (FFP) in the hemodynamically unstable patient. For temporary mechanical fracture stabilization, a pelvic binder is placed on arrival if it has not been done in the pre-hospital phase. Constant reassessment of the patient’s hemodynamic status is performed in order to avoid late recognition of a bleeding patient.
The non-responder
If the patients’ systolic blood pressure remains less than 90 mmHg despite administration of 2 L of crystalloid solution and 2 units of PRBC, the patient is considered as a “non-responder.” These patients are not amenable to further diagnostic procedures and undergo urgent exploration, pre-peritoneal pelvic packing, and mechanical stabilization of the pelvic fracture (pelvic C-clamp and anterior external fixator). During pelvic packing, associated injuries that contribute to mortality, such as intra-abdominal hemorrhage, hemo-pneumothoraces, and long bone fractures, are simultaneously assessed and treated with damage control techniques. In case of persistent hemodynamic instability with ongoing need of volume resuscitation following surgery, a subsequent angiography is performed. If extravasation of contrast is seen, selective embolization with coils or foam is performed. Evidence of vessel spasm or abrupt cutoffs of vessels are likewise seen as signs of injury and embolization is carried out. If the patient stabilizes after angio-embolization, the patient then gets completion of the trauma evaluation including CT scans and any needed plain radiographs (case report; Fig. 1).
The responder
Patients adequately responding to fluid boluses and holding the systolic blood pressure > 90 mmHg after administration of 2 L of crystalloid solution and if necessary 2 units of PRBC undergo contrast-enhanced CT scan evaluation following the primary survey. In case of contrast extravasation, a pelvic angiography with embolization is subsequently performed with the pelvic binder in place. Patients with ongoing need of volume replacement to achieve hemodynamic stability, with ongoing suspicion of pelvic hemorrhage following angio-embolization, or with the need for a mechanical stabilization of the pelvic ring are urgently transferred to the operating room for pelvic stabilization and pre-peritoneal pelvic packing.
The transient responder
Similar to the “responder”, in the patient with at least temporarily achieved hemodynamic stability by volume resuscitation (blood pressure > 90 mmHg, however, only with continuous volume replacement), an additional multi-slice CT scan with contrast is performed and—according to the results—followed by angiography, surgical damage control procedures, and/or ICU admission similar to the “responder” situation.
Although these treatment algorithms describe the authors’ standard practice in the management of patients with severe pelvic fractures, the care of any patient must be individualized with alteration of this schema for associated injuries.
Conclusion
In hemodynamically unstable patients with pelvic fractures, early exsanguination and the late sequela of shock and massive transfusion represent the major cause of death. The initial decision depends on the shock status of the patient. In non-responders, only a direct transfer to the operating room, pelvic packing, mechanical stabilization of the pelvic ring, and optionally a subsequent angio-embolization is possible. The decision of whether pelvic angiography or pelvic packing should be performed depends on the careful assessment of the patient’s hemodynamic status and the result of the contrast media-enhanced CT scan. Angiographic embolization as a first-line treatment is reasonable only in transient responders and in responders with an arterial blush seen in the CT scan, indicating acute arterial bleeding. The pelvic binder should remain in place until a definitive surgical stabilization is performed.
Footnotes
Declaration of Conflicting Interests
The authors hereby declare that they have no conflicts of interest to disclose.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.