
Abstract
The identification of the ubiquitin–proteasome system as a new therapeutic target has been one of the most recent successes in cancer treatment. The development and clinical approval of the first-in-class proteasome inhibitor, bortezomib has revolutionized the treatment of multiple myeloma (MM) and mantle cell lymphoma (MCL). In MM, bortezomib is now integrated in induction, conditioning, consolidation, maintenance, and salvage treatment protocols. Bortezomib-based regimens provide high remission rates and confer significant survival advantage compared to conventional chemotherapy in both the bone marrow transplant and non-transplant setting. In MCL, overall response rates in patients who have received at least one prior therapy range from 30 to 45%, even in chemotherapy resistant patients. Clinical trials to further improve the sequencing of bortezomib-containing combination therapies are ongoing. Until recently, intravenous injection was the standard route of bortezomib administration. However, severe adverse side effects, peripheral neuropathy in particular, were observed in up to 16% of MM patients and up to 54% of MCL patients treated with intravenous bortezomib, with grade 3 and 4 in 11 and 12% of patients, respectively. Moreover, complete remission rates, if at all, are low and duration of response is short both in MM and MCL. These limitations may be overcome by changing the method of bortezomib administration as well as by rationally combining bortezomib with other therapeutic agents. Indeed, recent data demonstrate that subcutaneous bortezomib administration is non-inferior to intravenous administration, with an improved systemic safety profile, good local tolerance, and a more convenient route of administration. Based on these data, subcutaneous bortezomib injection was approved as a supplemental new drug application for all approved indications in MM and MCL after at least one prior therapy. More than 30 clinical trials in MM and MCL are currently ongoing to evaluate the efficacy and safety profile of subcutaneous bortezomib also in induction, maintenance, and salvage therapy.
Introduction
A new era of research was triggered by the identification of the ubiquitin–proteasome pathway nearly four decades ago. Specifically, Etlinger and Goldberg were the first to identify a soluble, non-lysosomal proteolytic complex responsible for the energy-dependent degradation of intracellular proteins. 1 Pioneering work by Aaron Ciechanover, Avram Hershko and Irwin Rose, in particular, characterized the proteasome and the concept of controlled proteolysis of ubiquitin-tagged substrates. 2 Moreover, functional deregulation of the proteasome has been identified to be intimately associated with the pathogenesis of multiple diseases. To translate basic knowledge of the proteasome into potential novel therapeutic agents, Alfred Goldberg together with Kenneth Rock, Michael Rosenblatt, and Tom Maniatis, founded the biotechnology company Myogenics/ProScript in 1992. Initial attempts of this company aimed at retarding protein degradation, which according to these investigators was responsible for the loss of muscle strength associated with diseases such as AIDS and muscular dystrophy. Between 1994 and 1995, a scientific team at Myogenics/ProScript led by Julian Adams had already generated the first proteasome inhibitors, among them the N-pyrazinecarbonyl-L-phenylalanaine-L-leucine boronic acid MG-341 (PS-341, LDP-341, MLM341), today known as bortezomib (Velcade®, Millenium Pharmaceuticals, Inc. Takeda Oncology Company). However, it was not until the finding that the activation of NF-kappa B, a molecule intimately linked to tumor cell signaling pathways, is dependent on proteasome function, that the attention of Adams’ team turned also onto cancer. 3 Excitingly, broad-spectrum antitumor activity of bortezomib was observed in a 60-cell line panel from the National Cancer Institutes (NCI), 4 and subsequent preclinical studies demonstrated its remarkable cytotoxic activity against multiple myeloma (MM) cells. 5 Based on the encouraging results of two clinical phase I trials in solid tumors, 6 non-Hodgkin's lymphoma, and refractory MM, 7 Millenium Pharmaceutics funded two multicenter clinical phase II trials in MM, the Study of Uncontrolled MM Managed with proteasome Inhibition Therapy (SUMMIT) 8 and the Clinical Response and Efficacy Study of bortezomib in the Treatment of relapsing MM (CREST). 9 The results of these trials together with data of a clinical phase III study, the Assessment of Proteasome inhibition for EXtending remissions (APEX), 10 fundamentally changed treatment strategies in relapsed/refractory and relapsed MM and significantly improved MM patient survival. Less than one decade after its generation, bortezomib was granted accelerated approval for the treatment of refractory MM in 2003 by the US Food and Drug Administration (FDA) and in 2004 by the European Medicines Agency (EMA); and in 2005 for the treatment of progressive MM after at least one prior therapy. In 2004, one year after bortezomib's first approval in the US, Aaron Ciechanover, Avram Hershko, and Irwin Rose received the Nobel Prize in Chemistry. 11
However, complete remission rates of bortezomib are low and its duration of response is short both in MM and mantle cell lymphoma (MCL).12,13 Moreover, intravenous use of bortezomib is limited by severe toxic effects, peripheral neuropathy in particular. These limitations may be overcome by changing the method of bortezomib administration as well as by rationally combining bortezomib with other therapeutic agents. Importantly, recent data demonstrate that subcutaneous bortezomib administration is non-inferior to intravenous administration, with an improved systemic safety profile, good local tolerance, and a more convenient route of administration. Subcutaneous bortezomib injection has therefore been approved by the FDA as a supplemental new drug application (sNDA) in 2012 for all approved indications in MM and MCL after at least one prior therapy. It therefore represents yet another advance in the management of patients with MM and MCL. This review article summarizes up-to-date knowledge on the clinical use of bortezomib in general, the efficacy as well as the systemic and local safety, and ongoing clinical trials of subcutaneous bortezomib, in particular.
Update on the Use of Bortezomib in MM and MCL
Bortezomib's unprecedented single agent activity is further enhanced by its combination with other drugs. For example, in 2007 the combination of bortezomib with pegylated liposomal doxorubicin was approved for the treatment of MM patients who have not previously received bortezomib and have had at least one prior line of anti-MM therapy.14,15 Moreover, striking advantages in progression free survival (PFS), time to progression (TTP), overall survival (OS), overall response rate (ORR), and complete response (CR) in a randomized phase III trial, the Velcade as Initial Standard Therapy in MM Assessment (VISTA), confirmed the superiority of bortezomib plus melphalan plus prednisone (VMP) versus melphalan plus prednisone (MP) and led to the approval of VMP for the treatment of newly diagnosed MM patients ineligible for transplant in 2008.16,17 In this year's final analysis of the VISTA trial, after five years of observation, a striking 31% reduced risk of death with VMP versus MP (median OS 56.4 versus 43.1 months) was reported. Importantly, no increased risk of second malignancies with VMP occurred. 18
Bortezomib-based therapies provide high remission rates and confer significant survival advantage compared to conventional chemotherapy also in the stem cell transplant setting. Ongoing studies investigate the role of bortezomib for induction therapy of transplant-eligible patients, but also for conditioning, maintenance, and salvage therapy. Specifically, in induction therapy, recent data demonstrate that the combination of bortezomib plus dexamethasone (VD) achieves higher response rate compared to previous standard chemotherapeutic induction strategies (vincristine–adriamycin–dexamethasone, VAD) both before and after autologous stem cell transplantation (ASCT), and shows a trend towards improvement of PFS. 19 Importantly, VD induction improves the outcome of MM patients with t(4;14) but not with del(17p). 20 Other strategies achieving high remission rates before transplant include bortezomib plus doxorubicin/adriamycin plus dexamethasone (PAD) 21 ; cyclophosphamide plus bortezomib plus dexamethasone (CyBorD/VCD) 22 ; bortezomib plus thalidomide plus dexamethasone (VTD)23,24; and bortezomib plus thalidomide plus dexamethasone plus cyclophosphamide (VTDC). 25 Importantly, a subgroup analysis from the HOVON-65/GMMG-HD4 trial demonstrated that bortezomib before and after ASCT overcomes the negative prognostic impact of renal impairment in newly diagnosed MM. 26 A comparison of combinations with bortezomib, dexamethasone, cyclophosphamide, and lenalidomide (VDC, VDR, VDCR) in previously untreated MM patients (multicenter EVOLUTION trial) showed high activity and good tolerability of all combinations. However, no substantial advantage was noted with VDCR over three-drug combinations. 27 Bortezomib-induction followed by ASCT and lenalidomide consolidation-maintenance may be a valuable option for elderly MM patients, with the greatest benefit in those younger than 70 years of age. 28 For secondary induction and mobilization in MM patients who had an incomplete and stalled response to, or had relapsed after, previous immunomodulatory drug-based induction, bortezomib plus dexamethasone plus liposomal doxorubicin (DoVeD) could represent an alternative strategy. 29 To overcome the problem of bortezomib-associated toxicity, a regimen with low dose bortezomib plus thalidomide plus dexamethasone (vTD) has been proposed. Compared to VD, vTD achieves a significantly higher response rate before ASCT, with comparable toxicity. 30 In consolidation therapy, two cycles of VTD after the second transplant induced high rates of durable molecular response associated with a better outcome.23,31 Importantly, VTD consolidation, without bisphosphonates, reduced bone resorption and was associated with a very low incidence of skeletal-related events (SREs) in MM patients post ASCT. 32 Furthermore, bortezomib and high-dose melphalan (Bor-HDM) is a safe and promising conditioning regimen. However, randomized studies are needed to assess whether this conditioning is superior to high dose melphalan alone. 33 The Nordic Myeloma Study Group showed that bortezomib consolidation therapy is beneficial for patients not achieving at least a very good partial response (VGPR), but not for patients in the ≥VGPR category at randomization. Moreover, consolidation with bortezomib after ASCT in bortezomib-naïve patients improved PFS without interfering with quality of life (QOL). 34 In maintenance therapy, bortezomib is well tolerated. A survival advantage was reported in MM patients with negative prognostic features such as gain 1q21 and t(4;14). 21 Long-term treatment of bortezomib in combination with thalidomide indicates an advantage in PFS and suggests a favorable safety profile. 35 In salvage therapy, new data show that the combination of vorinostat and bortezomib prolongs PFS relative to bortezomib and placebo; however, the clinical relevance of the difference in PFS between the two groups is not clear. 36 Moreover, VTD is more effective than TD in the treatment of patients with MM with progressive or relapsing disease post-ASCT. However, VTD is associated with a higher incidence of grade 3 neurotoxicity. 37 Furthermore, based on promising anti-MM activity in a phase I clinical trial, 38 the combination of the oral pan-deacetylase inhibitor panobinostat plus bortezomib was evaluated in a phase II clinical trial program (Panobinostat or Placebo with Bortezomib and Dexamethasone in Patients with Relapsed Multiple Myeloma [PANORAMA]) to treat patients with relapsed and bortezomib-refractory MM (with ≥2 prior lines of therapy, including an immunomodulatory drug, and patients who had progressed on or within 60 days of the last bortezomib-based therapy). The ORR was 34.5% (1 patient with nCR and 18 patients with PR). An additional 10 patients achieved minimal response, for a clinical benefit rate of 52.7%. Median exposure and PFS were 4.6 and 5.4 months, respectively. 39 Finally, a phase I/II clinical trial evaluated the combination of bendamustine plus bortezomib. This combination was well tolerated and showed an ORR of 48% in a heavily pretreated population of MM patients. 40 In addition, a multitude of ongoing studies evaluate bortezomib-containing double, triple, and quadruple combinations with existing as well as additional targeted novel agents. For example, the combination of the anti-CS1 monoclonal antibody elotuzumab plus bortezomib was generally well-tolerated and showed encouraging activity in patients with relapsed/refractory MM in a phase I clinical trial. 41 Results of the clinical phase II/III clinical trial are eagerly awaited.
In MCL, five independent studies including the PINNACLE study used bortezomib in first relapse and beyond. Based on ORR ranging from 30 to 45% and durable remissions despite the inclusion of many chemotherapy-resistant patients, the US FDA granted approval to bortezomib for treatment of patients who had received at least one prior therapy in 2006.42–49 Subsequently, Lamm et al. showed promising activity and manageable toxicity of bortezomib plus rituximab plus dexamethasone in patients with heavily pretreated MCL. 50 Specifically, the ORR was 81.3% (13 patients), with seven patients achieving a CR (43.8%). The median PFS and OS were 12.1 and 38.6 months, respectively. In patients achieving a CR, the median PFS and OS had not been reached at the time of publication. Adverse events (greater than grade 2) included thrombocytopenia (37.5%), fatigue (18.8%), and peripheral neuropathy (12.5%). Two patients discontinued bortezomib because of grade-3 neuropathy. Another study by the Groupe Ouest Est d'Etude des Leucémies et Autres Maladies du Sang (GOELAMS group) suggested the combination of rituximab, bortezomib, doxorubicin, dexamethasone, and chlorambucil (RiPAD+C) as first-line therapy for elderly MCL patients. 51 Similarly, the combination of fludarabine, bortezomib, and rituximab seems to be an active regimen with manageable toxicity for patients with relapsed and/or refractory MCL. 52
Subcutaneous Administration of Bortezomib–- Efficacy and Systemic Toxicity Profiles
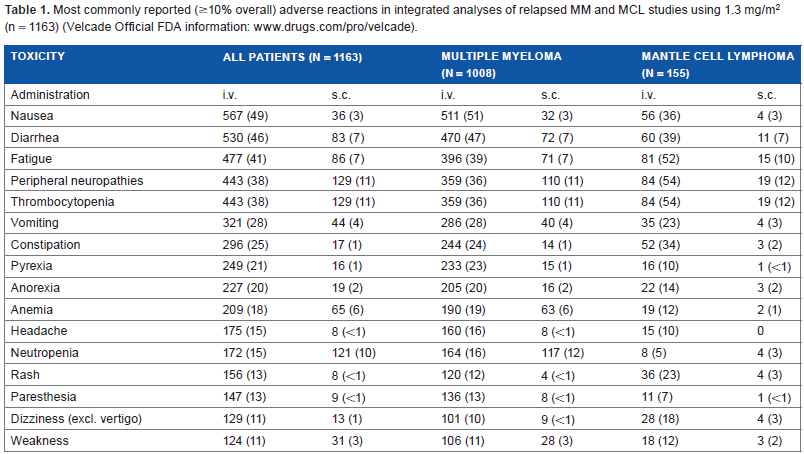
When administered intravenously, the use of bortezomib has two major drawbacks. First, its side effects, disabling peripheral neuropathy in particular, are a frequent cause for treatment discontinuation. Nausea, vomiting, diarrhea, and hypotension were also reported, requiring the use of anti-emetics or anti-diarrheals as well as the replacement of fluids and electrolytes. Specifically, in an integrated analysis of 1163 patients with relapsed MM and MCL in clinical phase I and II studies of intravenous bortezomib, the most commonly reported adverse reactions included nausea (49%), diarrhea (46%), fatigue (41%), peripheral neuropathy (38%), and thrombocytopenia (32%). A total of 26% of patients experienced serious adverse reactions. The most commonly reported serious side effects included diarrhea, vomiting, and pyrexia (each 3%); nausea, dehydration, and thrombocytopenia (each 2%); and pneumonia, dyspnea, peripheral neuropathies, and herpes zoster (each 1%) (Table 1) (http://www.velcade.com; www.drugs.com/pro/velcade). Bortezomib-induced peripheral neuropathy is dose-related and predominantly sensory, although severe cases of mixed sensory motor and autonomic neuropathy have been reported as well. Patients with pre existing symptoms (numbness, pain, or a burning feeling in the feet or hands) and/or signs of peripheral neuropathy may experience worsening during treatment with bortezomib. Neuropathy appears to be reversible in most patients.
Most commonly reported (≥10% overall) adverse reactions in integrated analyses of relapsed MM and MCL studies using 1.3 mg/m2 (n = 1163) (Velcade Official FDA information: www.drugs.com/pro/velcade).
Second, the intravenous route and twice per week schedule of administration requires frequent hospital visits and thereby significantly restricts the patients’ QOL. Importantly, significant reduction in the incidence of peripheral neuropathy has been achieved both by a once-per-week schedule of intravenous bortezomib17,35,47,48,53 as well as by subcutaneous administration of bortezomib. In contrast to MM, the weekly schedule of intravenous bortezomib in MCL, although less toxic, yielded fewer and lower quality responses than twice-weekly bortezomib. 47 However, the authors suggest that given the similar PFS, the weekly schedule may still be appropriate for some patients.
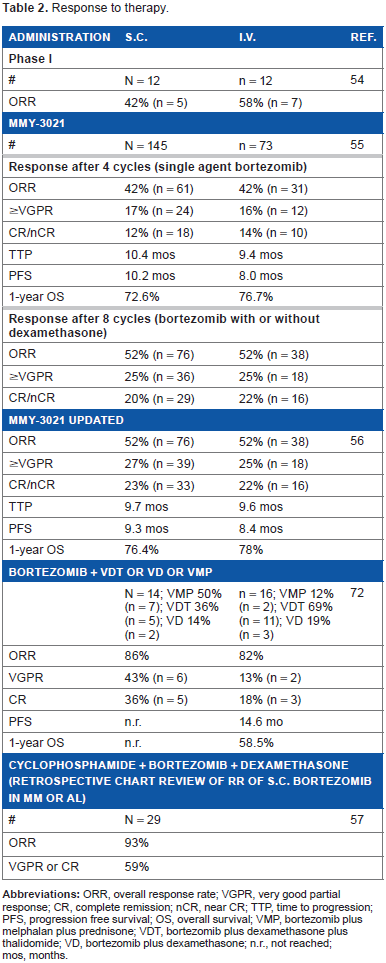
In 2008, Moreau et al. hypothesized that subcutaneous administration of bortezomib could be a good alternative option of administration for patients with poor venous access to improve convenience for patients and physicians. A subsequent randomized clinical phase I trial of subcutaneous (n = 12) versus intravenous bortezomib (n = 12) in patients with relapsed or refractory MM at the recommended dose and schedule (1.3 mg/m2, days 1, 4, 8, 11; eight 21-day cycles) showed similar systemic bortezomib exposure and 20S proteasome inhibition levels. Importantly, the safety profile and response rate in the subcutaneous arm did not appear inferior to the intravenous arm, with good local tolerance of subcutaneous injection. 54 Based on these promising results, the MMY-3021 phase III clinical trial (n = 222) was undertaken at 53 centers in ten countries in Europe, Asia, and South America. Specifically, 222 patients aged 18 years or older with measurable, secretory MM, who had received one to three previous lines of therapy and had evidence of disease progression were randomly assigned to receive subcutaneous (n = 148) or intravenous (n = 74) bortezomib. Of this, 16% had high-risk cytogenetics, ie any of t(4;14) or del17p by FISH or karyotype, t(14;16) by FISH, or del13 by karyotype. The response-evaluable population consisted of 145 patients in the subcutaneous group and 73 patients in the intravenous group. Patients received a median of eight cycles (range 1–10) in both groups. ORR after four cycles was 42% in both groups (61 patients in the subcutaneous group and 31 in the intravenous group; ORR difference: 0.4%, 95% CI: 14.3–13.5), showing non-inferiority (P = 0.002). After a median follow-up of 11.8 months (interquartile range, IQR 7.9–16.8) in the subcutaneous group and 12.0 months (8.1–15.6) in the intravenous group, there were no significant differences in TTP (median 10.4 months, 95% CI 8.5–11.7, versus 9.4 months, 7.6–10.6; P = 0.387) and one-year OS (72.6%, 95% CI 63.1–80.0, versus 76.7%, 64.1–85.4; P = 0.504) with subcutaneous versus intravenous bortezomib. 55 An updated outcome analysis after prolonged follow-up of up to ten cycles of bortezomib +/- dexamethasone showed ORRs of 52% in each arm (including 23 and 22% CR or nCR with subcutaneous and intravenous bortezomib, respectively), TTP of a median 9.7 versus 9.6 months (hazard ratio 0.872, P = 0.462), PFS of a median 9.3 versus 8.4 months (hazard ratio 0.846, P = 0.319), and a one-year OS of 76.4 versus 78.0%, P = 0.788) 56 (Table 2). Most importantly, the MMY-3021 trial was the first to demonstrate an improved safety profile of subcutaneous bortezomib versus intravenous delivery, with markedly lower rates of peripheral neuropathy of any grade (56 [38%] versus 39 [53%]; P = 0.044), grade 2 or worse (35 [24%] versus 30 [41%]; P = 0·012), and grade 3 or worse (nine [6%] versus 12 [16%]; P = 0·026). 55 In the follow-up analysis of this trial, peripheral neuropathy remained significantly lower with subcutaneous versus intravenous bortezomib, and increased rates of improvement/resolution at the time of final analysis. Specifically, in the subcutaneous arm, 74% of peripheral polyneuropathy improved or resolved in a median of 2.5 months (range 1.1–5.1); in the intravenous arm, 83% of peripheral polyneuropathy events resolved or improved in a median of 8.4 months (range 0.8–2.7) 56 (Table 3). Taken together these data show that, while a lower incidence of peripheral neuropathy is associated with the subcutaneous administration of bortezomib, its resolution over time is similar in both treatment arms. Based on these data, subcutaneous administration of bortezomib has been approved as a sNDA for all approved indications in MM and MCL after at least one prior therapy, first in the US (January 2012), later in the EU (September 2012).
Response to therapy.
Rates of adverse events.
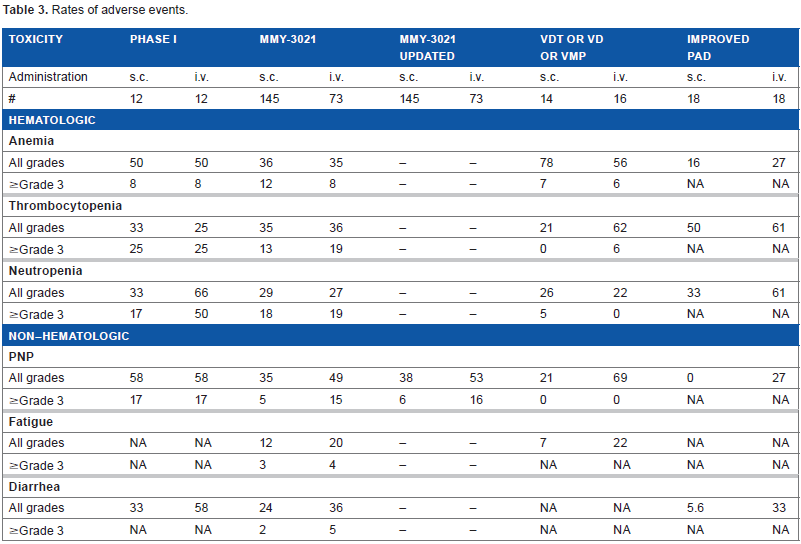
The first retrospective analysis of the efficacy and safety of subcutaneous versus intravenous bortezomib in combination therapies (VDT, VD, and VMP) in newly diagnosed MM patients showed ORR of 86 versus 82%. Importantly, an improved toxicity profile of subcutaneous versus intravenous bortezomib was also observed in combination regimens. Of interest, no notable gastrointestinal toxicity (nausea, emesis) was observed with subcutaneous bortezomib. Therefore no intravenous hydration or anti-emesis was required. In contrast, grade 1–2 nausea and emesis were recorded in 61.1% of patients treated with intravenous bortezomib despite of antiemetic prophylaxis. Peripheral polyneuropathy occurred in only 21% of patients treated with subcutaneous bortezomib versus 69% of patients treated with intravenous bortezomib. Consistent with these data, a retrospective chart review of RR and toxicity in newly diagnosed patients with MM or systemic light-chain amyloidosis receiving CyBorD showed high ORR of 93%, with 59% of patients achieving VGPR or CR 57 (Table 2). None of the patients developed grade 3/4 peripheral neuropathy, whereas one patient experienced grade 3 diarrhea, and two patients developed grade 3 thrombocytopenia requiring dose reductions. The efficiency and safety of subcutaneous bortezomib as part of the PAD regimen in induction therapy was demonstrated most recently. The improved PAD regimen using subcutaneous instead of intravenous bortezomib significantly reduced adverse side events, and improved the safety of clinical bortezomib application with non-inferior efficacy. Specifically, peripheral neuropathy occurred in none versus 27% of patients; anemia in 16.7 versus 27%; and diarrhea in 5.6 versus 33.3% of patients 58 (Table 3).
Effective induction therapy was also observed in a 56-year-old Chinese man with newly diagnosed Polyneuropathy, Organomegaly, Endocrinopathy, Monoclonal gammopathy and Skin changes (POEMS) syndrome, who was treated with subcutaneous bortezomib in combination with dexamethasone (BDex). Specifically, peripheral neuropathy and laboratory-test results of the patient improved dramatically with four cycles of treatment, resulting in CR. As expected, the treatment was well tolerated; and adequate peripheral blood hematopoietic stem cells were collected for an ensuing ASCT. 59
Subcutaneous Administration of Bortezomib–-Local Reactions
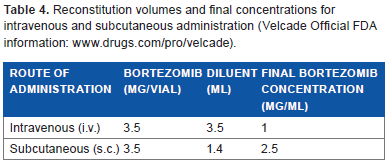
In the MMY-3021 trial, only 9 of 147 (6%) patients had one or more subcutaneous injection-site reactions, with the majority of reactions being mild hyperpigmentation, and resulting in discontinuation or dose withholding in two (1%) patients. All reactions completely resolved in a median of six days. 55 Kamimura et al. retrospectively analyzed the incidence and severity of injection site reactions (ISRs) following subcutaneous bortezomib administration in 15 Japanese patients with MM. Grade 1 ISRs occurred following 40 of 158 (25.3%) subcutaneous bortezomib injections in ten patients, whereas grade 2 ISRs occurred following seven injections (4.4%) in five patients. Five patients did not develop ISR. Of note, grade 2 ISR occurred in 6 of 65 (9.2%) thigh injections but only in 1 of 93 (1.1%) abdominal injections. These data show that grade 2 ISRs were more common in the thigh compared with the abdomen, possibly because the thigh contains lesser adipose tissue than the abdomen. Importantly, grade 2 ISRs resolved without any sequelae within a median of seven days. Based on these data the authors recommend to perform abdominal subcutaneous injections of bortezomib instead of injections into the thigh, especially for emaciated patients. 60 If bortezomib-induced ISRs occur, the subcutaneous use of a less concentrated solution (1 mg/mL instead of 2.5 mg/mL) or intravenous administration should be considered. External steroid therapy improves itching and phlebitis around the local injection site. 60 Similarly, topical evening primrose oil may be efficient to reduce bortezomib-induced skin reactions. 61 It is recommended that injections of bortezomib (2.5 mg/mL corresponding to 3.5 mg bortezomib reconstituted with 1.4 ml 0.9% saline) (Table 4) should be rotated among eight different sites, the right and left abdomen, upper and lower quadrant, as well as the right and left thigh, and proximal and distal sites. New injections should be administered at least 1 inch from an old site and never into areas where the skin is tender, bruised, erythematous, or indurated. When an injection is administered, the injection number should be recorded in the corresponding area of the “VELCADE® (bortezomib) for Subcutaneous Administration Site Tracker” diagram provided by Millenium Pharmaceuticals, together with the date and comments, if any, in the accompanying table. The information sheet should be placed in the patient's file and referred to for the mapping of future sites. Stickers that indicate the route of administration are provided with each bortezomib vial. These stickers should be placed directly on the syringe of bortezomib once it is prepared to help alert practitioners of the correct route of administration (http://www.velcade.com). Needles that are between 4 and 6 mm should be administered at a 90° angle. Use of the air-sandwich technique will lock the drug into the subcutaneous fat, avoiding sheering of drugs through the subcutaneous fat on injection. 62
Reconstitution volumes and final concentrations for intravenous and subcutaneous administration (Velcade Official FDA information: www.drugs.com/pro/velcade).
Subcutaneous Administration of Bortezomib–- Ongoing Clinical Trials
More than 30 clinical trials currently evaluate the efficacy of subcutaneous bortezomib application in combination therapies, weekly dosing, or long-term maintenance administration in MM and other hematologic malignancies. For example, clinical trials in MM currently evaluate the efficacy and safety of subcutaneous versus intravenous bortezomib as part of the PAD regimen in induction therapy; in consolidation treatments after induction therapy, and ASCT in newly diagnosed MM patients; as part of oral cyclophosphamide-based induction and sequential bortezomib and lenalidomide for maintenance treatment in newly diagnosed non-transplantable MM patients; and in combination with lenalidomide and dexamethasone for relapsed and/or refractory MM, followed by subcutaneous bortezomib maintenance. 63
In MCL, a clinical trial that is now recruiting participants aims to evaluate first line MCL treatment with rituximab, subcutaneous bortezomib, bendamustine, and dexamethasone (RiBVD) in patients older than 65 years or 18–65 years old who cannot or refuse to receive a conditioning regimen followed by ASCT. 63
Malignancies other than MM or MCL in which the efficacy of subcutaneous bortezomib is evaluated as part of combination therapies include relapsed/refractory adult acute lymphoblastic leukemia (ALL); high-risk acute myeloid leukemia (AML) in remission; KRas-mutant non-small cell lung cancer (NSCLC); diffuse large B-cell lymphoma (DLBCL) with poor IPI score; and relapsed/refractory indolent B-cell non-Hodgkin lymphoma (NHL), and CLL. 63
Concluding Remarks and Future Perspectives
The availability of bortezomib, the first-in-class proteasome inhibitor, has radically changed MM treatment and significantly improved patient outcome. Today, bortezomib is integrated in induction, conditioning, consolidation, maintenance, and salvage protocols and bortezomib-based therapies provide high remission rates and confer survival advantage compared to conventional chemotherapy in both the BM transplant and non-transplant setting. Indeed, a recent meta-analysis in MM patients demonstrates that bortezomib-containing induction regimens in transplant-eligible patients result in an improved depth of response, which translates into improved post-transplant PFS and OS outcomes, despite a higher incidence of toxicity. 64 Patient survival increased from 3–4 to 7–8 years as a direct result. 65 Several preclinical and more than 130 clinical studies combining bortezomib with other conventional and novel therapies are ongoing to further enhance treatment-induced antitumor activity and overcome the development of drug resistance in MM.
Until recently, the standard route of bortezomib administration was the intravenous route. However its side effects, peripheral neuropathy in particular, and the route of administration, significantly restrict patients’ QOL. One way to overcome this obstacle is subcutaneous bortezomib administration. Specifically, the anti-MM efficacy of subcutaneous bortezomib has been demonstrated to be non-inferior to intravenous bortezomib, while associated with a significantly lower incidence of neuropathy. 54 Whether neuropathy triggered by intravenous bortezomib may be improved by switching from intravenous to subcutaneous bortezomib remains to be investigated. Discontinuation of bortezomib therapy because of disabling neuropathy may thereby be avoided. 66 Longer time of absorption, significantly lower maximum serum concentrations and the longer median time to reach the final plasma concentration of subcutaneously versus intravenously administered bortezomib seem to be, at least in part, causative for the reduced peripheral neuropathy. In contrast, 20S proteasome inhibition and cumulative pharmacodynamics activity are similar after subcutaneous and intravenous bortezomib administration.54–56 Interestingly, peripheral neuropathy was less severe in patients receiving bortezomib in induction therapy than in patients with relapsed or refractory disease. 17 35 One reason may be the aggravation of disease-related neuropathy by intravenous bortezomib. Functionally, bortezomib reduces neurite length, and inhibits the serine protease HtrA2/Omi, which is known to be involved in neuronal survival. 67 Moreover, bortezomib induces a depolarizing shift in resting membrane potential prior to the development of neuropathy. Membrane depolarization could be associated with impairment of the electrogenic Na+-K+-ATPase-dependent pump caused by toxic effects of bortezomib on mitochondria. 68 More recently, Azoulay et al. demonstrated that bortezomib-induced peripheral neuropathy is related to altered levels of brain-derived neurotrophic factor in the peripheral blood of patients with MM. 69 However, exact molecular mechanisms, which trigger bortezomib-induced neuropathy are to date unknown. A recently developed in vitro model of peripheral neuropathy using rat dorsal root ganglia neuronal cultures recapitulates clinical sensory axonopathy and demonstrates that bortezomib induces an alteration in microtubules and axonal transport. Future mechanistic studies using this model to elucidate peripheral neuropathy and its prevention are eagerly awaited. 70 Importantly, in contrast to subcutaneous bortezomib, which improves peripheral neuropathy and decreases gastrointestinal side effects, fatal events occurred in patients treated with inadvertent intrathecal bortezomib administration. 71 This finding further highlights the neurotoxic effect of bortezomib. The recently updated label of bortezomib now includes a contraindication for intrathecal administration; bortezomib is for intravenous or subcutaneous use only (http://www.velcade.com). To evaluate improvements of the QOL of patients treated with subcutaneous bortezomib, the effect of subcutaneous administration on practice efficiency variables as well as patient preferences and satisfaction was recently determined at the Winship Cancer Institute of Emory University, Atlanta. Analysis of 92 medical records indicated a 38% reduction in chair time (143 versus 89 minutes) and a 27% reduction in infusion centre visit time (169 versus 123 minutes), with subcutaneous versus intravenous administration of bortezomib. Of the 60% of patients completing the survey, 68% preferred and were more satisfied with subcutaneous bortezomib administration. Further multicentre studies in a large patient cohort are required to confirm these data. 66 Investigations to test the feasibility of self-administering bortezomib at home are ongoing. Moreover, more than 30 clinical trials in MM and MCL are ongoing to evaluate the efficacy of subcutaneous bortezomib in induction, maintenance, and salvage therapy.
In summary, 11 years after its initial approval, ongoing clinical trials aim to further improve bortezomib-containing regimens in order to further improve anti-MM and anti-MCL efficacy and reduce toxicity. Subcutaneous bortezomib administration has become an attractive alternative to intravenous bortezomib administration due to its lower incidence and severity of peripheral neuropathy and non-inferior efficacy.
Author Contributions
Conceived the concept: KP. Analyzed the data: KP. Wrote the first draft of the manuscript: KP. Made critical revisions: KP. The author reviewed and approved of the final manuscript.
Disclosures and Ethics
As a requirement of publication the author has provided signed confirmation of compliance with ethical and legal obligations including but not limited to compliance with ICMJE authorship and competing interests guidelines, that the article is neither under consideration for publication nor published elsewhere, of their compliance with legal and ethical guidelines concerning human and animal research participants (if applicable), and that permission has been obtained for reproduction of any copyrighted material. This article was subject to blind, independent, expert peer review. The reviewers reported no competing interests. Provenance: the authors were invited to submit this paper.