
Abstract
The therapeutic effects of bortezomib in untreated and refractory/relapsed multiple myeloma have been demonstrated in several clinical trials, displaying superiority to the conventional treatments. However, many treatment-related toxicities, such as bone marrow suppression, infections and peripheral neuropathy, are well known and lead to treatment discontinuation and dose modification, especially in elderly patients. The purpose of this review is to summarize the published literature concerning the efficacy and safety of reduced-intensity induction therapy with bortezomib-based regimens in elderly patients with multiple myeloma. We used the VISTA trial as a reference and compared it with the seven trials identified in a systematic search. The data suggest that low-dose bortezomib significantly reduces therapy-related toxicities, especially neuropathy, and decreases the rate of discontinuation compared with the twice-weekly regimen, without losing efficacy. In light of this review, we suggest that once-weekly infusion of bortezomib in addition to melphalan–prednisone may be considered as a new standard of care in frontline treatment of elderly patients with symptomatic multiple myeloma.
Introduction
Bortezomib is a specific inhibitor of the 26S proteasome, and has been shown to induce apoptosis by inhibiting activation of nuclear factor kappa B (NF-κB) [Nencioni et al. 2007]. Since the activity of bortezomib is based on a reversible inhibition, continuous inhibition of the proteasome was investigated in preclinical trials. These studies demonstrated that continuous inhibition led to intolerable toxicity. After a single bortezomib injection, proteasome inhibition is detectable within 1 hour and is lost within 48 hours. This fact led to the twice-weekly schedule of bortezomib in an attempt to maximize the duration of proteasome inhibition, while avoiding the toxicity of continuous inhibition. After the initial phase I study results demonstrated activity, the twice-weekly schedule was developed as the standard treatment. This treatment consists of intravenous bolus injections of bortezomib 1.3 mg/m2 on days 1, 4, 8 and 11 and dexamethasone 20–40 mg/day on days 1, 2, 4, 5, 8, 9, 11 and 12 every 3 weeks [Richardson et al. 2003].
Clinical trials have shown that bortezomib has therapeutic effects in untreated and refractory/relapsed multiple myeloma (MM), displaying superiority to the conventional treatments [Richardson et al. 2005b; San Miguel et al. 2008]. Various combinations of bortezomib with other agents, such as melphalan, thalidomide and cyclophosphamide, have shown better outcome than conventional strategies [Bringhen et al. 2010; Mateos et al. 2010a; Reeder et al. 2010].
Attention must also be focused on treatment-related toxicities, which include bone marrow suppression, infections, gastrointestinal manifestations and, in particular, peripheral neuropathy (PN), which has been recognized as one of the major problems leading to dose modification and treatment discontinuation. In clinical trials, bortezomib-induced PN (BIPN) was documented in 30–50% of patients with MM under the twice-weekly schedule. It has been suspected that the dose intensity is related to the incidence of PN and other adverse effects [Mohty et al. 2010]. It is especially difficult for elderly patients with MM, who have a poor performance status, to complete aggressive combination treatments in clinical practice. Based on the fact that BIPN often improves or is resolved by discontinuation or reduction of bortezomib doses, treatment regimen modifications such as longer intervals between cycles have been proposed and tested in elderly patients [Bringhen et al. 2010; Mateos et al. 2010a, 2010b; Reeder et al. 2010; Tokuhira et al. 2011]
Methods
Based on this background we have performed a systematic search of the literature using MEDLINE databases from 2001 to October 2011, and a manual search of references. We used the following medical subject headings (MESHs) to identify potential studies: ‘Multiple Myeloma’ AND ‘Weekly Bortezomib’, which yielded 43 citations. One additional phase III study, Velcade as Initial Standard Therapy in Multiple Myeloma (VISTA) [San Miguel et al. 2008], was included, as it was judged relevant as a reference. We restricted the eligibility criteria to studies available as full publications only, and papers published in English. In total, seven studies were included: four phase II clinical trials, two phase III clinical trials and one case report. Three of them were conducted with elderly patients (≥65 years) and the rest included all ages; nevertheless the median age in these studies was 68 years. The main characteristics of the included trials are summarized in Table 1, as well as the main data extracted from the VISTA trial which we will use as the standard of the twice-weekly regimen.
Summarized data from the seven once-weekly bortezomib trials and VISTA trial which was used as a reference for the twice-weekly schedule.
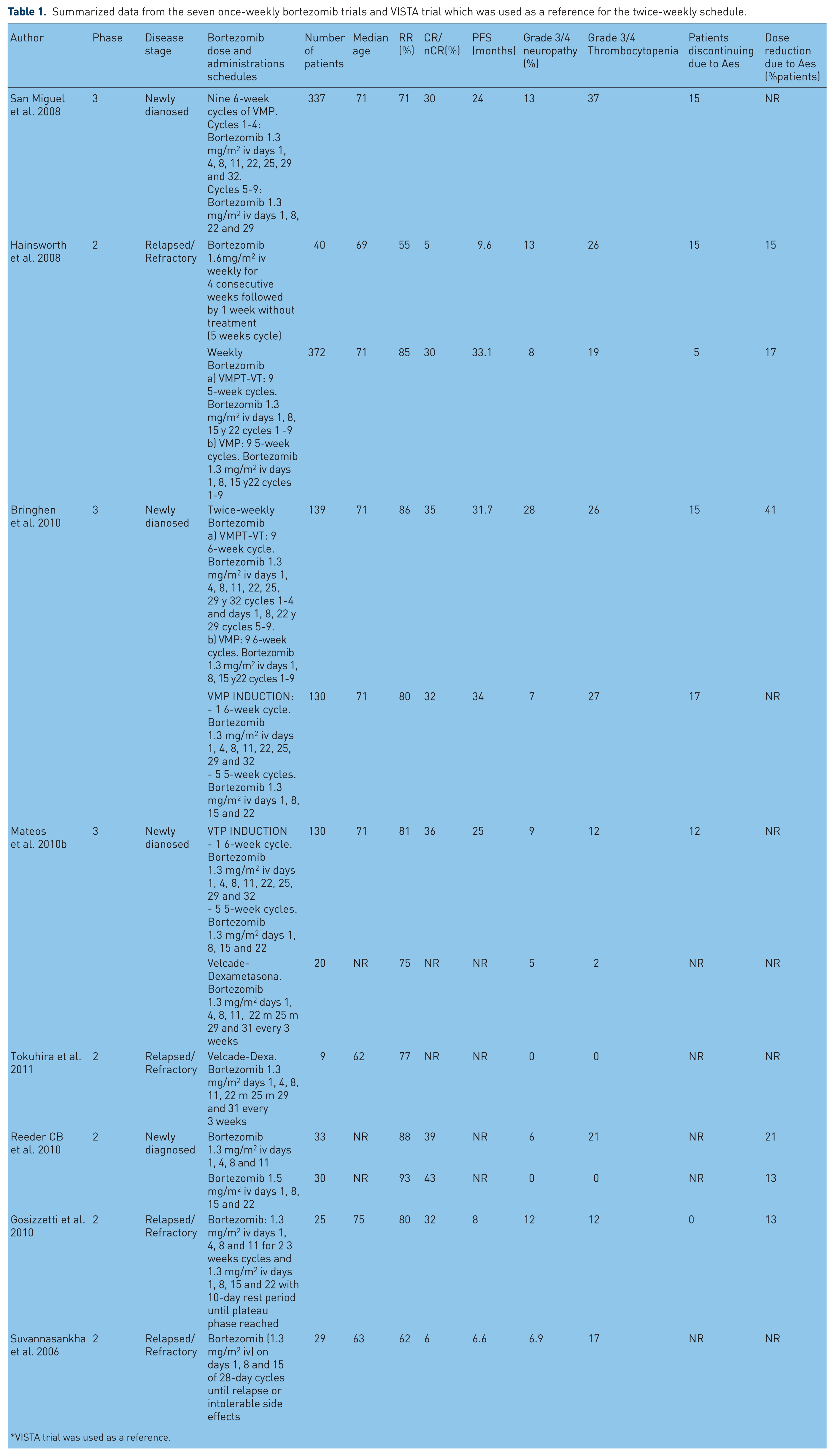
VISTA trial was used as a reference.
Results and discussion
Two studies explored bortezomib dose reduction before the VISTA trial was performed. The first, a phase II trial published in 2006 [Suvannasankha et al. 2006], explored weekly bortezomib/methylprednisolone in patients with relapsed MM. With 29 patients being included and a median number of treatments of 6 cycles, 62% of patients reached clinical response, including 3% complete response (CR), 3% near complete response (nCR) and 55% partial response (PR). In this trial, the median time to progression (TTP) was 6.6 months and the median overall survival (OS) was 20.2 months. These results were comparable with other salvage regimens and the reduced intensity of bortezomib did not decrease the clinical benefit (RR 35%, CR/nCR 10% and PR 18% published in the SUMMIT trial) [Richardson et al. 2003]. Bortezomib-induced toxicity was usually mild and grade 3/4 adverse effects were not frequent: neuropathy (7%), gastrointestinal side effects (3%), congestive heart failure (3%) and thrombocytopenia with transfusion requirements (17%).
In February 2008, the Minnie Pearl Cancer Research Network* designed a non-randomized phase II study to evaluate the efficacy and toxicity of weekly infusion of bortezomib alone in 40 patients with recurrent or refractory MM [Hainsworth et al. 2008]. In this trial, a response rate (RR) of 55% (95% confidence interval [CI] 40–70%) was documented; the median response duration in patients with objective response was 16 months; progression-free survival (PFS) for the entire group was 9.6 months, achieving a 1-year PFS rate of 39%. These efficacy parameters were similar to those reported in the pivotal trial using a twice-weekly bortezomib schedule (RR 43%, TTP 6.2 months) [Richardson et al. 2005a, 2005b], as well as the spectrum and incidence of toxicity. Treatment was well tolerated for most patients and the grade 3/4 side effects were similar to those reported with the twice-weekly schedule: 4 patients (10%) developed grade 3 neuropathy and 10 (26%) had a grade 3/4 thrombocytopenia. Six patients required dose reduction of bortezomib and another six discontinued treatment with bortezomib because of inacceptable related toxicity.
Since the large randomized phase III VISTA [San Miguel et al. 2008] trial (in transplantation-ineligible patients with newly diagnosed MM) demonstrated the superiority of bortezomib–melfalan–prednisone (VMP) versus melfalan–prednisone, this scheme has been considered a new standard of care for these patients. However, 46% of patients receiving VMP in VISTA had experienced serious adverse effects (38% thrombocytopenia, 20% gastrointestinal and 13% peripheral sensory neuropathy), yielding to a high rate of treatment discontinuation (34%). Consequently, the difference between the planned bortezomib dose and the finally delivered bortezomib dose was surprisingly high (67.6 mg/m2 and 38.5 mg/m2 respectively).
As a result of these findings, a less intensive bortezomib-based treatment regimen has been explored by the Spanish group (PETHEMA) [Mateos et al. 2010a]. A total of 260 elderly patients with untreated MM were randomised to receive six cycles of velcade–melphalan–prednisone (VMP) versus velcade–thalidomide–prednisone (VTP) as induction therapy. The schema consisted of one cycle of twice-weekly bortezomib for 6 weeks, followed by five cycles of once-weekly bortezomib; plus either melphalan (9 mg/m2 on days 1–4) or daily thalidomide (100 mg) and prednisone (60 mg/m2 on days 1–4). Maintenance therapy consisted of one conventional 3-week bortezomib cycle plus either thalidomide or prednisone.
Similar efficacy was obtained with VMP/VTP, with a mean CR rate during induction therapy of 24% (28% in VTP and 20% in VMP). There was no difference found in terms of PFS and OS between the two treatment arms on induction. Nevertheless, after a median follow up of 22 months from second randomization, a benefit of bortezomib plus thalidomide maintenance was found over bortezomib plus prednisone maintenance regimen (PFS 32 months versus 24 months, respectively). Furthermore, the use of maintenance therapy resulted in a substantial increase in CR rate to 42% (44% in VTP group and 39% in VMP) in patients randomly assigned for maintenance therapy. Regarding toxic effects, VMP produced more haematological toxicities than VTP, particularly neutropenia and thrombocytopenia. Treatment with VTP resulted in more serious adverse events (31% versus 15%) and discontinuations (17% versus 12%). The most common grade 3 or worse toxicities were infections (1% in the VTP group versus 7% in the VMP group), cardiac events (8% versus 0%) and peripheral neuropathy (7% versus 9%). No grade 3 or worse haematological toxicities were recorded during maintenance therapy. Considering these results, the study concluded that a reduced-intensity bortezomib schema is associated with a reduction in the incidence of grade 3 or worse peripheral neuropathy (8% versus 13% in VISTA) and gastrointestinal symptoms (4% versus 19% in VISTA) compared with the conventional schedule of VMP used in the VISTA trial and that the use of maintenance therapy results in an increased CR rate.
The most relevant study is from the Italian group GIMEMA (Gruppo Italiano Malattie Ematologiche dell’Adulto), who performed a randomized phase III trial to compare bortezomib–melphalan– prednisone–thalidomide followed by maintenance with bortezomib–thalidomide (VMPT-VT) versus VMP in elderly patients with newly diagnosed MM [Bringhen et al. 2010]. In both arms patients initially received a twice weekly bortezomib schedule, but after 139 patients, the protocol was changed to a weekly bortezomib scheme in order to reduce toxicity maintaining efficacy. Bringhen and colleagues have made a post hoc analysis of the trial comparing the initial twice-weekly with the once-weekly schedule. In total, 139 patients received the twice-weekly schedule, and 372 received the once-weekly schedule. When both arms where compared in terms of efficacy (within the limitations of a nonrandomized post hoc analysis) there was no difference found between once-weekly and twice-weekly bortezomib schemes. The ORR was 85% versus 86% in twice- and once-weekly group, which includes CR rates of 30% versus 35% and VGPR rates of 55% and 54%, respectively. The 3-year PFS was 50% versus 47% and the 3-year time-to-next-therapy rate was 72% versus 61% in the once- and twice-weekly schedules, respectively. Surprisingly, and probably due to the dose reduction and treatment discontinuation induced by toxic effects in the twice-weekly bortezomib arm, patients in both groups of treatment received a very similar median cumulative bortezomib dose (39.4 mg/m2 in the once-weekly group and 40.1 mg/m2 in the twice-weekly group), corresponding to 84% and 59%, respectively, of the planned total dose of bortezomib. The overall incidence of grade 3/4 PN was significantly reduced in the once-weekly versus twice-weekly group (8% versus 28%). In fact, once-weekly bortezomib was the only factor associated with a reduced incidence of any-grade PN and grade 3/4 PN. The incidence of any grade 3/4 haematologic toxicity was similar in the two groups (44% versus 45% in once- and twice-weekly patients, respectively), but severe thrombocytopenia was slightly less common in the once-weekly patients (19% versus 26%). The incidence of nonhaematologic grade 3/4 adverse events was also significantly reduced in the once-weekly versus twice-weekly group: 131 patients (35%) in the once-weekly group versus 68 (51%) in the twice-weekly group.
In addition to the conclusions mentioned previously, the GIMEMA trial also concluded that the onset of PN increased over time and reached a plateau after approximately 12 months of treatment, whether the once-weekly or twice-weekly scheme was used, suggesting that bortezomib can be used as maintenance therapy without increasing the risk of PN. This finding is in contrast with results of the risk of thalidomide-induced PN, which increases over the course of the treatment without reaching a plateau.
Tokuhira and colleagues published a report of nine cases of patients with refractory MM who needed a modified bortezomib administration schedule in order to avoid toxic effects and treatment discontinuation [Tokuhira et al. 2011]. In this study the treatment modification schedule was made according to the physician’s judgment. The complete series is made of 40 patients with refractory MM receiving bortezomib– dexamethasone with the standard twice-weekly schedule of bortezomib. Nine patients were treated with a modified bortezomib interval, consisting in a once-weekly or longer interval administration due to multiple reasons, mainly toxic effects and social factors. When two groups were compared, there was no difference found in the response rate (75% in the twice-weekly schedule versus 77% in the modified schedule) and a shorter overall survival was found in the twice-weekly group (10 months) compared with that in the modified group (16 months). All patients were alive with the modified schedules, but only 7 of 20 patients were alive with the twice-weekly schedules (13 cases died because of disease progression or infection). Regarding toxicity, no patients on the modified schedule experienced grade 3–4 adverse events, whereas 12 incidences of these events (5 PN, 4 infections, 2 thrombocytopenia and 1 elevated serum amylase) in 10 patients were observed with the twice-weekly administration. With these findings the authors suggest that the modified bortezomib schedule is well tolerated and safe, and achieves good responses even in patients with relapse/refractory myeloma.
Bortezomib has also been administered in combination with other drugs such as cyclophosphamide for the treatment of both relapsed and untreated multiple myeloma. A phase II trial has been performed to compare once versus twice-weekly bortezomib induction therapy with CyBorD in newly diagnosed MM [Reeder et al. 2010]. A total of 63 patients were included in this trial, 33 receiving twice-weekly bortezomib and 30 receiving once-weekly bortezomib schedule; 55 patients were evaluated after 4 cycles of treatment, obtaining a similar profile of response rate (ORR 93% versus 88%, VGPR 60% versus 61%) for the two groups of treatment (once-weekly versus twice-weekly bortezomib, respectively). Patients receiving once-weekly bortezomib experienced less grade 3/4 adverse events (37% versus 3%) compared with those receiving the twice-weekly scheme, which leads to fewer bortezomib dose reductions (21% versus 13%).
Weekly bortezomib was explored in combination with pegylated liposomal doxorubicin and dexamethasone by Gozzetti and colleagues in elderly patients with relapsed/refractory MM [Gozzetti et al. 2011]. A total of 25 patients were treated with two twice-weekly bortezomib cycles followed by a median of two once-weekly bortezomib cycles. As we have seen in the other studies, bortezomib dose reduction did not lead to a loss of efficacy (ORR 80%, CR 32%, PFS 8 months) but it was involved in a significant reduction of grade 3/4 toxicity (PN 12%, thrombocytopenia 12%). No drug discontinuation was required in this study and only 4 patients required bortezomib dose reduction because of grade 3 toxicity.
Conclusions
In summary, standard twice-weekly schedule is effective but has high therapy-related toxicities, especially in elderly patients. In order to reduce toxicity maintaining efficacy, these seven studies have explored low-dose bortezomib-based therapies. Comparing the results of these seven studies to those reported in the VISTA trial (one of the standard regimens in elderly patients), similar efficacy is observed: PFS in the standard dose group is close to the low-dose group in studies where only new diagnosed patients where included (not in studies with relapsed MM patients, which seems to be plausible); ORR is also similar in the VISTA trial (75%) versus the low-dose regimen studies, which obtained a response rate between 71% and 93%. This demonstrates that a less intensive bortezomib-based treatment regimen could be administered to elderly patients maintaining its efficacy.
Regarding toxicity, a low-dose bortezomib regimen is better tolerated than the standard schema. Once-weekly schedule results in less toxicity, particularly grade 3–4 adverse events as thrombocytopenia (in the VISTA trial was 37% and in the other studies varies from 2% to 26%) and neuropathy (17% observed in the standard regimen and 5–13% in low-dose regimes) in most of the studies (less neuropathy was not found in the VMP induction schema in the PETHEMA trial). This optimum tolerance to the therapy decreases the rate of discontinuation and the proportion of patients who need dose reduction due to adverse effects (13–17% in all patients receiving a once-weekly schedule versus 41% in the VISTA trial). We can conclude that low-dose bortezomib significantly reduces therapy-related toxicities, especially neuropathy, and decreases the rate of discontinuation compared with the twice-weekly regimen. This improvement in the safety profile is not associated with a reduction in efficacy.
In light of this review, we suggest that once-weekly infusion of bortezomib in addition to melphalan–prednisone in the VMP combination is a valuable treatment schedule and may be considered as a new standard of care in the frontline treatment of elderly patients with symptomatic MM.
Footnotes
Funding
This work was supported by Fundacion CRIS against cancer.
Conflict of interest statement
The authors declare no conflicts of interest in preparing this article.