
Abstract
ADHD is the most common neuropsychiatry disorder affecting children and adolescents, and may cause impairment in many domains of social and occupational functioning. Despite proven efficacy of existing treatments, recent focus has been on the development of newer, once-daily medications. Lisdexamfetamine (LDX) was first released in 2007 and is approved for the treatment of ADHD in ages 6 and above. LDX is a uniquely formulated stimulant, a prodrug which requires an enzymatic hydrolytic reaction to be converted to active dextroamphetamine. LDX has a longer duration of action compared to other stimulants and has less potential to be misused or abused. LDX has repeatedly demonstrated improvement in ADHD symptoms compared to placebo, and seems to be at least as effective as other stimulants. LDX still carries the risks and disadvantages of other stimulants and may be more expensive than other stimulants. LDX can be expected to be increasingly used as a first-line agent for the treatment of ADHD.
Keywords
Introduction
Attention-Deficit/Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder marked by inattention, hyperactivity, and impulsivity which leads to impairment in social, educational, or occupational functioning. 1 ADHD is among the most common disorders affecting children, and has an estimated prevalence of 5%-8% of school-age children. 2 ADHD has three sub-classifications: Predominantly Inattentive Type (IT), Predominantly Hyperactive Type (HT), and Combined Type (CT), which meets criteria for both Inattentive and Hyperactive types. 1 Children with ADHD are more prone to developing delayed learning and academic difficulties as well as disruptive and socially inappropriate behaviors. 2 Although some children have remission of symptoms as they age, ADHD is considered a chronic condition. Other children are at significant risk for serious sequelae including educational difficulties, relationship problems, legal problems, employment difficulties, and substance use and abuse. 2 Children with ADHD are also more at risk for the development of other psychiatric disorders, including mood disorders, anxiety disorders, and other disruptive behavior disorders. 2 Medications classified as stimulants, derivatives of either methylphenidate (MPH) or amphetamine (AMP), have been the established gold-standard pharmacotherapy for ADHD. 3 Despite the efficacy of these medications, immediate-release formulations tend to “wear off” over the course of the day. 4 This may require multiple doses of immediate-release medication, including doses being given at school. 4 Short-acting medications, with their quick onset of action and a high peak of effect, present themselves as possible targets of abuse or misuse. Long-acting stimulant formulations may eliminate the need for in-school doses and decrease the propensity for these medications to be abused. One such example is Lis-dexamfetamine dimesylate (Vyvanse®, LDX), which was released in 2007 as a novel prodrug formulation of dextroamphetamine. 5 LDX was intended to have similar efficacy to other long-acting stimulant formulations, reduced risk of side effects and toxicity, and reduced potential for misuse/abuse. 6 This article is designed to help clinicians understand the pharmacology of LDX, the evidence supporting its efficacy and safety, its potential for abuse, and its place in therapy for treating ADHD.
Mechanism of Action, Metabolism, and Pharmacokinetic Profile
Dysfunctional transmission of the catecholamines norepinephrine and dopamine has been widely accepted as pertinent to the pathophysiology of ADHD. 7 Evidence of this includes the use of methylphenidate (MPH) and dextroamphetamine (AMP) as the main first-line treatments for ADHD over the past half century. 7 Methylphenidate acts as a dopamine-and norepinephrine-reuptake inhibitor, thereby increasing extrasynaptic concentrations of both molecules. Dextroamphetamine not only inhibits reuptake, but also increases the presynaptic release of both dopamine and norepinephrine. Dextro-amphetamine also inhibits monoamine oxidase, the main enzyme responsible for the breakdown of dopamine and norepinephrine. Either methylphenidate- or dextroamphetamine-based formulations can be considered first-line treatment for ADHD. 7
Lisdexamfetamine (LDX) is a pharmacologically inactive prodrug which consists of dextroamphetamine covalently bound to the amino acid lysine. Upon oral administration, LDX is steadily absorbed through the gastrointestinal tract.8,9 The lysine is cleaved off through enzymatic hydrolysis, forming l-lysine and the active drug, dextroamphetamine. The active dextroamphetamine stimulates neurotransmitter release of norepinephrine and dopamine from presynaptic neurons, and also competitively inhibits reuptake of norepinephrine and dopamine at the level of the nerve terminal.8,10 In this matter, dextroamphetamine exerts its action in the CNS via the cerebral cortex and reticular activating system to cause increased mental alertness. 8
Although the time to reach maximum concentration level (Tmax) of dextroamphetamine can be prolonged with administration of fatty foods, it is not thought to slow its therapeutic effect, nor is it believed that food has an effect on the maximum drug concentration or the bioavailability. There is also no reported alteration in the absorption pattern secondary to changes in gastric acidity.6,11 LDX is absorbed primarily through the small intestine, 12 and due to the covalently-bound lysine, absorption is likely mediated through peptide transporters. 13 Although a minimal amount of LDX is hydrolyzed to dextroamphetamine in the GI tract, the majority of the conversion occurs after absorption once the prodrug is in the bloodstream, specifically on the erythrocyte. 13 Since LDX is metabolized to l-lysine and dextroamphetamine nearly immediately after absorption, there is no “first pass” metabolism by the liver, as conversion to dextroamphetamine occurs before the molecule reaches the liver.10,13
LDX undergoes gradual release by the rate-limiting hydrolysis to l-lysine and dextroamphetamine. 14 The metabolism of LDX to dextroamphetamine in erythrocytes occurs linearly and appears to be a high-capacity system and is unlikely to become saturated at therapeutic doses. 13 The fact that the enzymatic conversion cannot easily be saturated and is not determined by variations in factors of absorption like gastric pH or GI transit produces a consistent rate of hydrolysis and delivery, which results in the consistent and predictable pharmacokinetic profile of LDX. 13
The pharmacokinetic profile of LDX is similar in children and adults. The plasma half-life of the active dextroamphetamine is 6-8 hours in children and 10-12 hours in adults, with LDX, the inactive form, being available less than one hour.8,10 An open-label study of adult volunteers administered 14C-radiolabelled LDX showed LDX to be quickly absorbed and converted to dextroamphetamine. 4 Following administration of the radiolabelled LDX, systemic concentrations of dextroamphetamine were found to be nearly 20 times higher than that of the original LDX prodrug. 4 Of the radio-active oral dose, 96% was recovered in the urine within 120 hours. 4 LDX reaches steady-state concentration in 2-3 days. 15 The duration of efficacy was found to be similar with up to 13 hours post dose in children (6 to 12 years) and up to 14 hours post dose in adults (18 to 55 years). LDX was not found to inhibit any of the cytochrome P450 enzymes and appears to have low potential for drug-drug interactions.5,16 The drug is eliminated via urinary excretion,8,10 with an elimination half-life of the LDX prodrug less than 30 minutes. 4 Urinary excretion of LDX can be affected by urinary pH.8,10 It has been reported that for every one unit of increase of urinary pH, the half-life is increased by 7 hours. 8
The prodrug formulation of LDX is unique, as other long-acting stimulant formulations rely on encapsulated matrix or beaded formulations to prolong absorption and duration of action. 4 As an example, mixed amphetamine salts–-extended release (MAS-XR) is a formulated capsule containing two types of beads, one released immediately and the other on a delayed-release caused by pH changes in the GI tract. Thus, consistent drug delivery of MAS-XR may be altered through changes in gastric acidity, whereas this should not affect the absorption or distribution of LDX. 4
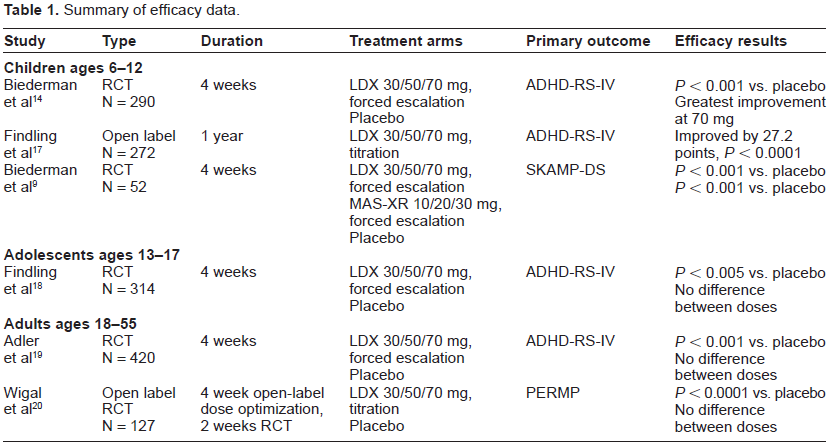
Clinical Studies of Efficacy (Table 1)
Summary of efficacy data.
Children
Biederman and colleagues 9 performed a double blind, randomized, multicenter, cross over study with LDX (30, 50, 70 mg combined) and mixed amphetamine salts extended-release (MAS-XR, 10, 20, and 30 mg combined). The study included 52 children ages 6 to 12 years diagnosed with ADHD, Combined Type or Hyperactive/Impulsive type. Scales used in the study included the Swanson, Kotkin, Agler, M-Flynn and Pelham (SKAMP) Deportment Rating Scale (SKAMP-DS), and the Attention Rating Scale (SKAMP-AS); the Permanent Product Measure of Performance-Attempted (PERMP-A) and Correct (PERMP-C) scores; and Clinical Global Impressions (CGI) Scales scores. In this study, LDX was comparable to MAS-XR, and had greater benefit as compared to placebo in treating ADHD symptoms in school age children. Improvement was seen up to 12 hours after dose received. 9 It was reported that LDX provided a more consistent drug delivery as comparatively to MAS-XR, 10 which is likely attributable to the benefits of the prodrug formulation of LDX compared to the mixed bead formulation of MAS-XR.
Findling and colleagues 17 performed an open label, multicenter, study of 272 children with ADHD aged 6 to 12 years to assess long term safety, tolerability, and effectiveness of various doses of LDX, titrated over a 4 week period and maintained for 11 months. Changes in the Attention Deficit/Hyperactivity Disorder-Rating Scale (ADHD-RS) were noted from baseline to post baseline visits and mean improvement was 27.2 points. Improvements continued during each of the first four weeks and were maintained throughout the remaining 11 months of treatment. 17 Results from the CGI-I indicated that 80% of subjects were considered “improved” or “very much improved” at endpoint.
Biederman and colleagues 14 executed a randomized, double-blind, study with 290 children between the ages of 6 to 12 years randomized to 4 weeks of forced dose escalation of LDX 30, 50, and 70 mg or placebo for 4 weeks. The scales used included the ADHD Rating Scale, fourth version (ADHD-RS-IV) and the Connors’ Parent Rating Scale-Revised: Short Form (CPRS-R). There was significant improvement within the first week in ADHD-RS-IV and CPRS-R scores with those taking LDX 30 mg compared to placebo, with continued improvement in escalating doses, with greatest improvement seen in LDX 70 mg (effect size of 1.21 in 30 mg and 1.60 in 70 mg). There were similar findings of efficacy and tolerability of LDX as compared to previous reports of mixed amphetamine salts and was well tolerated. 14
Adolescents
Another study by Findling and colleagues 18 evaluated 314 adolescents ages 13-17 with moderate-to-severe ADHD symptoms (baseline ADHD-RS-IV ≥ 28) who were randomly assigned to placebo or LDX 30, 50, or 70 mg in a 4-week, forced dose escalation, double blind study. Primary outcome measures were the ADHD Rating Scale (ADHD-RS-IV) and the Clinical Global Impressions-Improvement (CGI-I). At all weeks of the study, all doses of LDX resulted in statistically significant improvement in ADHD-RS-IV and CGI-I scores compared to placebo. 18 Mean changes from baseline on the ADHD-RS-IV were -18.3, -21.1, and -20.7 for 30, 50, and 70 mg/d of LDX, respectively; and -12.8 for placebo (P < 0.005 for each). On the CGI-I, 69% of participants received doses of LDX were rated as much improved or very much improved, compared to 39% of those receiving placebo. However, there were not statistically significant differences between the different doses of LDX. This is in contrast to the aforementioned studies with children ages 6-12 which typically showed increasing efficacy at higher doses of LDX. 14
Adults
Adler and colleagues 19 organized a randomized, double-blind, placebo-controlled trial evaluating the efficacy of LDX in 420 adults ages 18-55 with moderate-to-severe ADHD. Following a 1-4 week washout period, participants were randomized to LDX 30, 50, or 70 mg of LDX or placebo for 4 weeks. Participants in the 50 and 70 mg groups underwent forced dose escalation. The primary outcome was the ADHD Rating Scale (ADHD-RS) total score. Treatment with all three doses of LDX was significantly more effective than placebo at reducing ADHD-RS total scores. 19 Significant changes occurred as early as the first week, and each additional week of treatment resulted in more participants who achieved significant reduction in ADHD symptoms. However, and perhaps surprisingly, there was no statistical significance between the dosage groups. Although all three groups differed significantly from placebo in terms of the percentage of participants who were rated as “improved” or “very much improved,” (30 mg = 57%, 50 mg = 62%, and 70 mg = 61%), the three groups did not differ from each other. 19
Wigal and colleagues 20 performed a randomized, double-blind, placebo-controlled, crossover study of efficacy and safety of LDX in adults with ADHD using a simulated adult workspace. After an open-label, 4 week dose optimization period of LDX 30-70 mg/d, 127 participants entered a two-week randomized, double-blind controlled crossover phase. Primary outcome measure was the Permanent Product Measure of Performance (PERMP) total scores averaged for all post-dose time points. In this study, LDX demonstrated significant efficacy in improving PERMP scores compared to placebo. 20
A recent study by DuPaul and colleagues 21 examined the efficacy of LDX compared to placebo in ameliorating ADHD symptoms in college students with ADHD compared to college students without ADHD. Twenty-four college students with ADHD were randomized to receive one-week each of placebo and LDX doses 30, 50, and 70 mg. To prevent the onset of side effects by first giving the highest dose of LDX, the 50 mg dose always preceded the 70 mg dose. At baseline and at the end of each 1-week phase, participants were administered the Conners’ Adult ADHD Rating Scale (CAARS), the Behavior Rating Inventory of Executive Functioning–-Adult Version (BRIEF-A), among other rating scales. The study found a linear relationship between LDX dose and reduction in ADHD symptoms, namely inattention and hyperactivity, as well as improvement in executive functioning. These results were comparable to other studies of efficacy for LDX. 21 There was a significant placebo effect for the ADHD symptoms, with 40% of the placebo group showing improvement, but only 13% of the placebo group showed improved in the BRIEF-A in executive functioning. Results were compared to 26 non-ADHD controls, which consistently outperformed the ADHD group in all dosage groups. Despite treatment, college students with ADHD showed a large deficit when compared to age-matched control subjects without ADHD. 21
Safety (Table 2)
Summary of safety data.
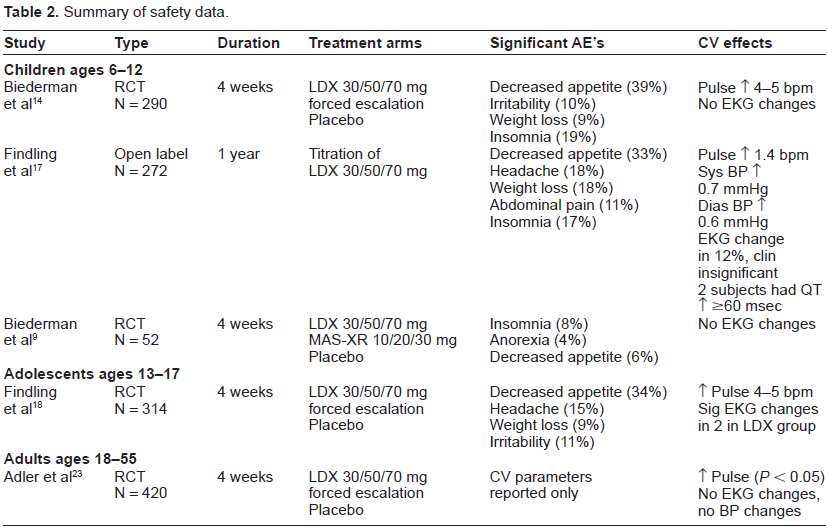
LDX's side effect profile is found to be consistent with other stimulants. The most common adverse reactions reported in children are decreased appetite, insomnia, abdominal pain, and irritability14,17; there was one case of alopecia reported. 22 As with other stimulants, there is controversial concern in regards to cardiovascular side effects from the use of stimulants.
In the Biederman study of 290 children ages 6-12, 14 adverse events (AEs) were experienced by participants receiving LDX more than those receiving placebo, with the highest rate of AEs occurring with the highest dose of LDX. The most frequently reported AEs of LDX that were significantly increased from placebo were decreased appetite (39%), insomnia (19%), irritability (10%), and weight decrease (9%). 14 More than 95% of AEs were deemed mild or moderate, and no serious AEs were reported. The majority of AEs occurred during the first week of treatment and dissipated over time. Twenty-one (7.2%) participants withdrew due to AEs, nearly half of which were in the 70 mg LDX group, the highest dose. LDX treatment was not associated with any significant changes in EKG or vital signs. There was a significant increase in heart rate in the 70 mg LDX group compared to placebo of 4-5 beats per minute, but this was felt to be clinically insignificant. 14
In the long-term efficacy and safety study by Find-ling in colleagues, 17 78% of the 272 participants, children ages 6-12, experienced a treatment-emergent adverse event (TEAE), 97.5% of which were considered mild or moderate. The most common TEAEs reported were decreased appetite (33%), headache and weight loss (18% each), insomnia (17%), and abdominal pain (11%). The majority of AEs occurred during the first 4 weeks of treatment. Insomnia and nausea appeared to be dose-related. 17 Of the 272 subjects, 25 (9%) discontinued due to AEs, with the most common reasons given being aggression, irritability, and decreased appetite (1.1% each). All five serious AEs, occurring in four patients, were considered unrelated to the study medication. 17 No deaths were reported. In terms of vital signs, changes from baseline included a mean increase in pulse by 1.4 beats per minute and mean increases of 0.7 mmHg and 0.6 mmHg for systolic and diastolic blood pressure, respectively. All EKG changes, observed in a total of 33 subjects, were considered clinically insignificant. Two subjects had a QT-interval change from baseline of at least 60 msec; no participants had a QT-interval of greater than 500 msec at any point during the treatment study.
A separate report by Adler and colleagues 23 evaluated the short term effect of LDX on cardiac parameters in adults with attention deficit hyperactivity disorder. The study was conducted via a multicenter, randomized, double-blind, placebo-controlled trial with a sample size of 420 patients and divided into four groups. Healthy adults were between ages of 18-55 who were randomly assigned to placebo or LDX 30, 50, or 70 mg for 4 weeks. Subjects underwent three phases during the study, screening and washout, baseline, and double-blind treatment. All four treatment groups were well matched at baseline and had no significant differences in baseline ADHD-RS total scores and Clinical Global Impression-Severity of Illness Scale scores. The study did not find a statistically significant change in systolic blood pressure and diastolic blood pressure from baseline to endpoint between each LDX group and placebo, although there was statistically significant difference between LDX groups and placebo for pulse (P < 0.05) and heart rate (P < 0.05). 23 Each LDX group had increases of pulse, starting from week 2 and persisting to week 4, from baseline to endpoint, with placebo showing no change. There were no significant effects on EKG parameters such as PR, RR and QT intervals. These findings are consistent with other recent studies of stimulant use in children and adults with ADHD that resulted in a lack of significant effects on EKG parameters. 23
Ermer and colleagues 24 performed a study with 20 adults between ages 18-55 with dose escalation from 50 mg up to 250 mg of LDX if tolerated. Ten of the 20 patients were eliminated from treatment due to elevation of blood pressure above defined, with all 10 being on doses above the FDA-recommended range. There were no clinically significant changes in EKG or laboratory changes noted. This study observed that the linear kinetics of LDX indicated a lack of saturation of the enzymatic conversion of LDX to dextroamphetamine, and the prodrug formulation did not protect against overdose if the drug was administered in supratherapeutic ranges. 24 A similar study by Boellner and colleagues 25 performed a randomized, open label, cross over study with LDX 30, 50, and 70 mg doses in 18 children ages 6 to 12 years. This study also revealed linear dose proportional increase in dextroamphetamine level. There was no reported intersubject variability, showing that LDX provided a consistent and predictable delivery system. 25
LDX is contraindicated in patients with known hypersensitivity to sympathomimetic amines. 5 Other contraindications include anorexia nervosa, bipolar disorder, psychotic disorders, symptomatic cardiac disease, structural cardiac anomalies, cardiac arrhythmias, cardiomyopathy, advanced arteriosclerosis, symptomatic heart failure, hyperthyroidism, glaucoma, and breast feeding. 5 LDX should not be used concomitantly with tricyclic antidepressants or within 14 days of using a monoamine oxidase inhibitor (MAOI).5,8 Combining LDX with another stimulant should be avoided due to the potential for additive effects such as irritability, nervousness, insomnia, and cardiac arrhythmias.5,8 There have been reported cases of sudden cardiac death of children on stimulants with normal dosing with concomitant structural cardiac anomalies. 8 There is no specific recommendation on how often to monitor cardiac parameters such as blood pressure and heart rate; the average heart rate can increase by 3-6 beats per minute and blood pressure by 2-4 mmHg. Any patient being considered for initiation of stimulants should have a careful history obtained including family history of sudden death, ventricular arrhythmias. A physical examination should be performed to assess for presence of cardiac disease with further evaluation via EKG and echocar-diogram as indicated. LDX comes under classification of FDA pregnancy category C, and is secreted in breast milk. 5 Teratogenic effects include increased incidence of premature birth, low birth weight, and withdrawal symptoms in the neonate.
Abuse Liability
The potential for medication abuse is a significant drawback of most stimulant medications, which is commonly known by families and is often sought to avoid in medication selection.26,27 Additionally, ADHD is frequently co-morbid with substance use disorders, 28 Utility of Lisdexamfetamine for ADHD which presents a challenging dilemma when many of the medications used to treat ADHD have abuse potential themselves. 28 The limited abuse potential of LDX is considered one of its greatest advantages compared to other stimulants. In fact, LDX is the only FDA-approved treatment for ADHD that includes abuse liability data in the package insert.4,5 The rate-limiting hydrolysis of LDX to active dextroamphetamine is likely responsible for the medication's limited abuse potential. Once swallowed, a delayed and reduced peak of effect, as evidenced by time to maximum concentration of 3.7 hours, makes LDX an unlikely choice for those who wish to abuse medications.28,29
It was previously thought that the conversion of LDX to dextroamphetamine occurred in the GI tract, which explained the limited abuse potential of other modes of administration such as snorting or IV injection.28,29 However, as previously discussed, this reaction takes place in the bloodstream, and therefore is not specifically protective against IV drug use. As mentioned, it is believed that the consistent rate of hydrolyzing LDX to l-lysine and dextroamphetamine is responsible for its limited abuse potential. To test this hypothesis, Jasinski and Krishnan 30 conducted a randomized, double-blind study to determine abuse liability of intravenous doses of LDX and immediate release d-amphetamine sulphate in adult stimulant abusers compared to placebo. Doses of 25 mg or 50 mg of LDX single doses, and 10 or 20 mg of immediate-release d-amphetamine sulphate or placebo were administered with a minimum of 48 hours between doses in a three way cross over design. Intravenous administration of LDX did not result in significant abuse in any of the 12 males in the study. 30
Jasinski and Krishnan 31 conducted a similar double-blind, randomized, placebo-controlled trial to determine abuse liability of oral LDX in patients with history of stimulant abuse. Participants were given single oral doses of LDX (50, 100, and 150 mg); or two active controls, d-amphetamine (40 mg), diethylpropion (200 mg); and placebo in 36 individuals. Abuse liability was statistically lower in patients administered LDX 100 mg as compared to dextroamphet-amine 40 mg. In supratherapeutic doses of 150 mg of LDX, abuse potential was similar to dextroamphet-amine 40 mg and diethylpropion 200 mg. Thus, abuse of LDX is still possible, but higher-than-expected doses are required to produce the same effect as lower doses of short-acting dextroamphetamine. 31
Patient Preference
The importance of patient preference in deciding on treatment options is receiving increasing attention. 26 Several studies have illustrated that more active patient participation in medical decision-making leads to increased adherence to treatment, improvement in symptoms, and increased quality of life. 26 Although there are several medications approved for the use of ADHD, there is not an overwhelming “dominant” choice that is considered first-line in most patients. 26 Therefore, patient and parental preferences can play a pivotal role when deciding between treatment options.
Studies comparing the active use of ADHD medications have illustrated the patient preference for once-daily dosing of stimulants compared to multiple daily dosing.26,32 Longer duration of action and decreased risk of side effects were also found to be desirable qualities.26,27 LDX's particularly long duration of action with medication effects lasting until the early evening is a significant advantage of this medication.29,33 A potential downside to this attribute, however, is if clinical efficacy is warranted more immediately. The onset of clinical effect of LDX was noted to be 2 hours, which is comparable to other long-acting formulations, 34 but longer than that of immediate-release formulations which can be as early as 30 minutes after the initial dose is given. 35 Thus LDX may not be as preferred for a patient whose ADHD symptoms merit more immediate amelioration. In terms of side effects, the rate-limiting hydrolysis that converts LDX to active dextroamphetamine can be saturated and halted with high doses, thus minimizing the potential for adverse effects.5,29 As LDX is converted to active dextroamphetamine, the side effect profile for LDX is expected to be similar to that of other amphetamine formulations. 34 These attributes would make LDX seem to meet many patients’ preferences.
On the other hand, there are studies indicating patient preference for methylphenidate products over amphetamine products, 26 as well as studies indicating preference for non-stimulants such as atomoxetine for patients who had previously tried a stimulant. 26 Many of these studies are based on “hypothetical” administration of medications for ADHD, as opposed to families who have had direct experience with such medications. When compared on efficacy, non-stimulants tend to have a lower response rate than their stimulant counterparts. Most participants in these studies were basing their decisions on the “hypothetical” scenario that efficacy was equal among medication classes, which may explain why those who have had direct experience with medications seen increased benefit and prefer stimulants over stimulants, particularly once-daily dosing. 26
In some of these studies, the majority of families preferred the idea of non-stimulant medication even when controlled for efficacy and side effect profile. 26 This may be correlated with low abuse potential, a drawback which is commonly known and sought to avoid in medication selection.26,27 Additionally, ADHD is frequently co-morbid with substance use disorder, 28 which presents a challenging dilemma when many of the medications used to treat ADHD have abuse potential themselves. 28 Due to LDX needing to be activated in the GI tract, the medication is less likely to be abused through other methods such as snorting or IV injection due to diminished availability of the active product.28,29 Additionally, once swallowed, a delayed and reduced peak of effect, as evidenced by time to maximum concentration of 3.7 hours, further reduces the abuse potential of this medication.28,29
Place in Therapy
LDX is a long-acting prodrug of dextroamphet-amine, which can be used once daily for the treatment of ADHD in children, adolescents, and adults. According to the FDA, LDX can be dissolved in water, and therefore still an option for patients with difficulty swallowing whole pills. The consistent pharmacokinetics, long duration of action, and limited abuse potential are the main advantages of LDX. As previously mentioned, either MPH or AMP products can be considered first-line for treatment of ADHD. Jain and colleagues 36 showed that children with significant ADHD symptoms despite treatment with an MPH product showed improved when switched to LDX, more improvement then could have been achieved by switching to a non-stimulant. There are also cross-over studies which show that patients who do not initially respond to an amphetamine-based product show improved symptomology when switched to MPH. Therefore there is evidence to suggest that certain patients may be more likely to ‘respond’ to one class than the other. The ADHD Practice Parameter for the Assessment and Treatment of ADHD developed by the American Academy of Child and Adolescent Psychiatry (AACAP) does not show preference for either the MPH or AMP classes of stimulants because evidence suggests there is no difference in efficacy. 37
The advantages of LDX do not come without a price; the price range for the current available dosage forms of LDX is slightly higher than other long-acting stimulant formulations, which in general are more expensive than short-acting stimulants. 34 Depending on the patient population being considered, this factor may inhibit LDX's more widespread use.
LDX has the advantages of a once-daily dosing of a stimulant, increased duration of action, and decreased potential for abuse. For families focused on efficacy and adherence, LDX is advantageous, and is being increasingly used as a first-line agent. For families who are more concerned with the risk of side effects of stimulants compared to non-stimulant medications, LDX and other stimulants may not be desirable.
Conclusions
ADHD is the most common neuropsychiatric disorder affecting children and adolescents, and may persist throughout adulthood and cause impairment in many domains of social and occupational functioning. Treatment strategies have included stimulants and non-stimulant medications, with stimulants remaining the gold-standard. Despite proven efficacy, the need for multiple daily dosing, concerns for the side effect profile, and the risk of abuse of these medications spurred the development of newer, once-daily medications.
LDX was first released in 2007 for the treatment of children with ADHD ages 6-12 and has since has gained FDA approval for adolescents ages 13-17 as well as adults. LDX is a uniquely formulated stimulant, a prodrug which requires an enzymatic hydrolytic reaction to be converted to active dextroamphetamine. Although this step delays the onset of action of LDX, it also allows for longer duration of action, once-daily dosing, and decreased risk for side effects compared to other stimulants. The prodrug formulation and required enzymatic reaction is also a deterrent for misuse and abuse, which is a significant advantage if substance use is a concern. Please see Table 3 for a summary points regarding the use of LDX in treating ADHD.
Summary points.
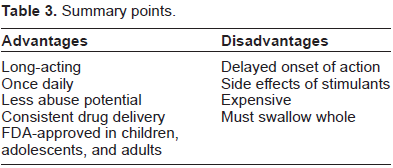
In terms of efficacy, LDX has repeatedly demonstrated improvement in ADHD symptoms and has shown improvement in behavior, executive functioning, and school/work performance. In children, statistically significant benefits have been seen with increasing doses of the medication, while this is questionable with adolescents and adults. The benefits of LDX are comparable to or at times better than other once-daily stimulant formulations such as MAS-XR. Specifically, the duration of effect for LDX was found to be significantly longer than most other stimulant formulations, up to 13-14 hours after the initial dose.
It is worth noting that the six placebo-controlled trials listed in Table 1, the trials used to obtain FDA approval for LDX, were either directly funded by or had authors who received financial support from the pharmaceutical company which manufactures LDX.9,14,17–20 Likewise, several of the other studies and trials referenced in this paper also directly or indirectly received funding from the pharmaceutical company.13,21,24,35,36
LDX still carries the risks and disadvantages of other MPH- and AMP-based stimulants, including decreased appetite, irritability, insomnia, abdominal pain, and weight decrease. There have been occasional observations of increases in cardiovascular parameters such as pulse and blood pressure, but these have been deemed clinically insignificant, as have EKG changes observed in several of the studies. There have been no deaths or serious adverse events related to medication administration in the major placebo-controlled trials of LDX. A minority of patients will likely discontinue due to side effects. On the other hand, the studies show that a significant portion of patients who have not found benefit with MPH-based stimulants may find substantial benefit by switching to LDX.
LDX may be more expensive than other stimulants, which is perhaps its most limiting factor for widespread use. Secondary to the prodrug formulation and rate-limiting enzymatic hydrolysis, LDX has a favorable abuse liability profile compared to other stimulant formulations. Results of long-term, open-label studies of LDX in children and adults have proven LDX to be clinically effective in reducing symptoms of ADHD throughout the duration of drug administration over a range of doses. LDX is generally well-tolerated, and demonstrates a side effect profile similar to other long acting stimulants. LDX can be expected to be increasingly used as a first-line agent for the treatment of ADHD.
Author Contributions
Conceived and designed the experiments: MN. Analysed the data: MN, MS. Wrote the first draft of the manuscript: MS, ST Contributed to the writing of the manuscript: MN, MS, ST. Agree with manuscript results and conclusions: MN, MS, ST. Jointly developed the structure and arguments for the paper: MN, MS, ST. Made critical revisions and approved final version: MN, MS, ST. All authors reviewed and approved of the final manuscript.
Funding
We have no conflicts of interests or financial ties to disclose.
Competing Interests
We have no conflicts of interests or financial ties to disclose.
Disclosures and Ethics
As a requirement of publication author(s) have provided to the publisher signed confirmation of compliance with legal and ethical obligations including but not limited to the following: authorship and contributorship, conflicts of interest, privacy and confidentiality and (where applicable) protection of human and animal research subjects. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. Any disclosures are made in this section. The external blind peer reviewers report no conflicts of interest. Provenance: the authors were invited to submit this paper.